Download presentation
Presentation is loading. Please wait.

1
GERD Panel Coordinator:Dr Afshin Shafaghi
Gastrointestinal and Liver Diseases Research Center (GLDRC) January 2015
 January")
2
Mr. A. is a 32 year-old bank clerk. He suffered from long standing GERD . He takes off a few days a month from his job and this problem has been the concern of his chief. Mr. A. fears the consequences of his illness . He will spend hours on the Internet searching to find more data about his disease.

3
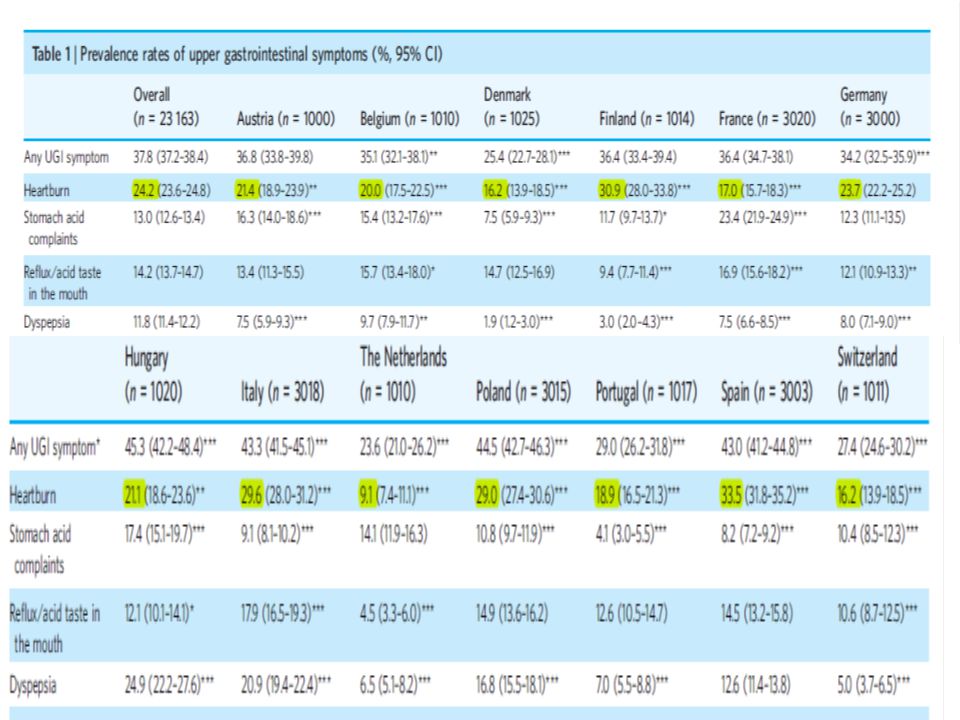
What is the prevalence of GERD worldwide, in our country and in our province, respectively ?
How about disease burden on society ?

10
The GI disease with the highest annual direct costs in the United States was GERD ($9.3 billion), followed by gallbladder disease ($5.8 billion), colorectal cancer ($4.8 billion), and peptic ulcer disease ($3.1 billion)* * Sandler R.S. et al. The burden of selected digestive diseases in the United States . Gastroenterology Volume 122, Issue 5, 2002, Pages 1500–1511

11
The overall prevalence of GERD in North America has been estimated at 18.6 million. GERD causes significant decrements in health-related quality of life that are directly related to symptom severity. Reduced work productivity is seen in a large proportion of subjects on prescription medication for gastro-oesophageal reflux disease. Symptom severity and nocturnal heartburn are significantly associated with reduced work productivity, particularly when nocturnal heartburn interferes with sleep.* * Dean B. B. et al. The burden of illness of gastro-oesophageal reflux disease: impact on work productivityAliment Pharmacol Ther 2003; 17: 1309–1317

12
Mr. A. was visited by his family doctor
Mr. A. was visited by his family doctor. He has a longtime history of chronic acid regurgitation and heartburn from adolescence that took OTC H2RA and AlMgS for his symptoms relief. He wakes up frequently at night and had daytime cough. He has a sedentary lifestyle and should eat fast foods and much tea due to his working conditions .He smokes cigarette. FH of gastric cancer in his grandfather was positive . He had a BMI=30 kg/M2 , His physical examination was unremarkable except mild wheezing in both lungs .

13
What is your drug free recommendations according to this step ?

14
Minimal therapy for GERD patients is comprised of lifestyle modification, dietary modification, as needed antacid use, over-the-counter H2 receptor antagonists, and over-the-counter proton pump inhibitors. Lifestyle modifications are aimed at enhancing esophageal acid clearance, minimizing the incidence of reflux events, or both as with cessation of smoking and avoidance of late meals:

15
Dietary modification may be helpful, but prohibition of many enjoyable foods virtually ensures noncompliance. It is more practical to suggest avoidance of a core group of reflux-inducing foods (fatty foods, chocolate, peppermint, and excessive alcohol, which may reduce lower esophageal sphincter pressure) and then to suggest that the patient selectively avoid foods known to cause symptoms. A number of beverages have a very acidic pH and can exacerbate symptoms. These include colas, red wine, and orange juice (pH 2.5 to 3.9).
 and then to suggest that the patient selectively avoid foods known to cause symptoms. A number of beverages have a very acidic pH and can exacerbate symptoms. These include colas, red wine, and orange juice (pH 2.5 to 3.9).")
16
Head of bed elevation, which can be achieved either by putting 6- to 8-inch blocks under the legs at the head of the bed or a Styrofoam wedge under the mattress. Head of bed elevation is important for individuals with nocturnal or laryngeal symptoms; its necessity in other situations is questionable.

17
Refraining from assuming a supine position after meals and avoidance of meals two to three hours before bedtime, both of which will minimize reflux. Avoidance of tight fitting garments, which reduces reflux by decreasing the stress on a weak sphincter. Obesity is a risk factor for GERD, erosive esophagitis, and esophageal adenocarcinoma . However, improvement in symptoms following weight loss is not uniform Nevertheless, because of a possible benefit, , weight loss should be recommended.

18
Promotion of salivation by either chewing gum or use of oral lozenges may also be helpful in mild heartburn. Restriction of alcohol use and elimination of smoking; smoking is deleterious in part because it diminishes salivation.

19
He was prescribed omeprazole 20 mg BD and Theophylline G syrup ,Ranitidine was stopped.
Do you agree with this prescription?

20
In patients with mild to moderate GERD, symptom severity and previous treatments can guide the selection of an initial acid suppressive regimen The most common and effective treatment of peptic esophagitis or symptomatic GERD is to reduce gastric acid secretion with either an H2 blocker or a proton pump inhibitor The medication dose is titrated to the severity of disease for each patient, with the goal being to raise the intragastric pH above 4 during the periods of the day that reflux is likely to occur

21
The proton pump inhibitors are more effective in healing esophagitis than the H2 receptor antagonists, with a therapeutic gain of 57 to 74 percent relative to placebo. In addition, proton pump inhibitors lead to more rapid healing and symptom relief than H2 receptor antagonists A systematic review demonstrated that for treatment of regurgitation among patients with GERD, proton pump inhibitor (PPI) treatment was superior to placebo or an H2 receptor agonist
 treatment was superior to placebo or an H2 receptor agonist.")
23
GERD and Asthma

24
Eight weeks later, Mr. A. did not improved well
Eight weeks later, Mr. A. did not improved well. He was referred to specialist . An upper GI endoscopy was performed and his medications was changed into Pantoprazole 20 mg BD , Salbutamol Inhaler 2puff Q6h and 10 mg Metoclopramide before each meals. What is your Idea about this treatment? Do you agree with upper GI endoscopy in GERD patients ?

25
A number of studies have compared the various proton pump inhibitors to one another. While some differences have been reported, the magnitude of differences has been small and of uncertain clinical significance. Prokinetic drugs (eg, bethanechol , metoclopramide , azithromycin ) increase lower esophageal sphincter pressure, enhance gastric emptying, and improve peristalsis. They may also reduce hiatus hernia size and therefore impact the position of the gastric acid pocket, which serves as a reservoir for acid reflux However, it is unclear if treatment with prokinetics leads to a reduction in GERD symptoms. In addition, their use is limited by side effects .There is currently no role for the use of prokinetics as monotherapy or adjunctive therapy for the treatment of GERD
 increase lower esophageal sphincter pressure, enhance gastric emptying, and improve peristalsis. They may also reduce hiatus hernia size and therefore impact the position of the gastric acid pocket, which serves as a reservoir for acid reflux. However, it is unclear if treatment with prokinetics leads to a reduction in GERD symptoms. In addition, their use is limited by side effects .There is currently no role for the use of prokinetics as monotherapy or adjunctive therapy for the treatment of GERD.")
26
INDICATIONS FOR UPPER ENDOSCOPY
•Men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting). •Men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton pump inhibitor therapy. •Men older than 50 years with chronic GERD symptoms (symptoms for more than five years) and additional risk factors for Barrett’s esophagus and esophageal adenocarcinoma (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat). .
. •Men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton pump inhibitor therapy. •Men older than 50 years with chronic GERD symptoms (symptoms for more than five years) and additional risk factors for Barrett’s esophagus and esophageal adenocarcinoma (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat). .")
27
EGD revealed sliding hiatal hernia , Distal esophagitis ,and Gastritis
EGD revealed sliding hiatal hernia , Distal esophagitis ,and Gastritis .Biopsies were taken from distal esophagus, proximal and distal parts of stomach

28
His symptoms improved but still persist
His symptoms improved but still persist. Endoscopic gastric biopsy specimen showed HP antral predominant gastritis and distal esophageal biopsy was shown below:

29
Should we treat H. pylori infection in this patient?

30
A possible role for H. pylori in the pathogenesis of GERD has been suggested in a number of studies. However, the link between GERD and H. pylori is complex and incompletely defined. The main linkage is in the effect that H. pylori has on gastric acid secretion. Hence, eradication of H. pylori is associated with mild worsening of GERD in patients with pan-gastritis (hyposecretors) and improvement in those with antral-predominant gastritis (hypersecretors). These effects must be balanced against the risks of continued infection.
 and improvement in those with antral-predominant gastritis (hypersecretors). These effects must be balanced against the risks of continued infection.")
31
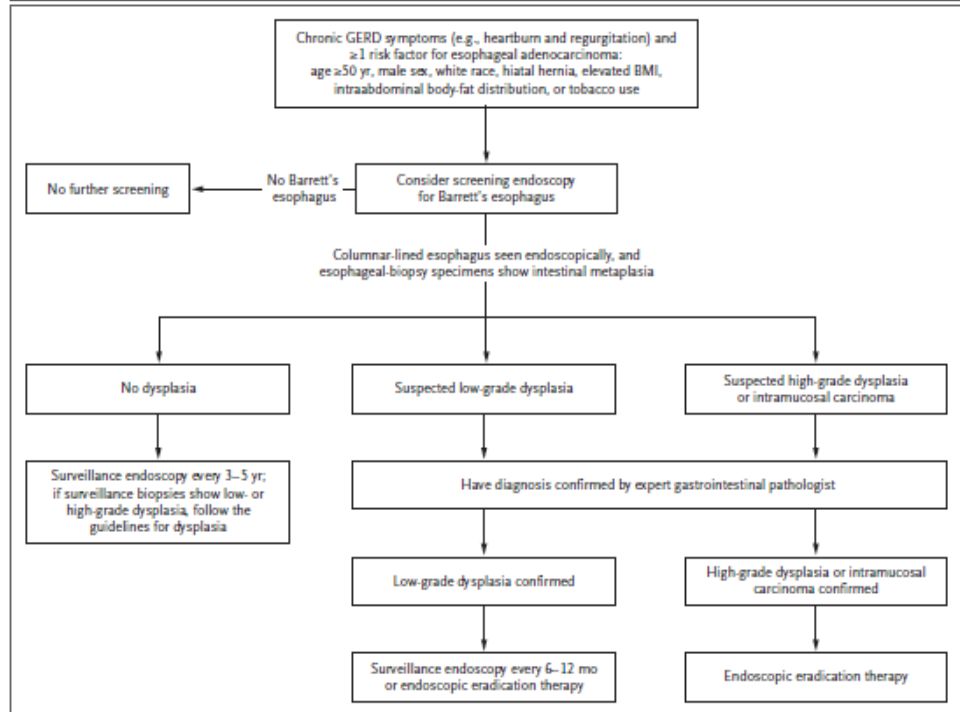
He referred to a gastroenterologist for careful follow up , he asked about another endoscopy? and worried about esophageal cancer, Does he need recent another EGD ? Which risk factors should be mentioned to him? How should we scheduled surveillance program for him?

32
Repeat endoscopy after this follow-up examination is not indicated in the absence of Barrett's esophagus unless patients have bleeding, dysphagia, or a significant change in symptoms while on effective therapy

36
Gastroenterologist add 10 mg Nortryptiline, nightly to PPI , 3 months later he was visited again, he was well but worried about cancer .He was reassured. Three months later he was visited , he arbitrarily discontinued his drugs and restarted Ranitidine twice a day ,What is your idea about this manner?

37
In patients with Barrett’s metaplasia, refluxed gastric acid can cause chronic inflammation, double-strand DNA breaks, and increased cell proliferation, all of which may contribute to carcinogenesis. This suggests that GERD should be treated aggressively in patients with Barrett’s esophagus, and there is indirect evidence to suggest that proton-pump inhibitors (PPIs) decrease the risk of cancer development. A recent cohort study involving 540 patients with Barrett’s esophagus who were followed for a median of 5.2 years showed that PPI use was associated with a 75% reduction in the risk of neoplastic progression
 decrease the risk of cancer development. A recent cohort study involving 540 patients with Barrett’s esophagus who were followed for a median of 5.2 years showed that PPI use was associated with a 75% reduction in the risk of neoplastic progression.")
38
PPI was restart, after 1 year Mr. A
PPI was restart, after 1 year Mr. A. was visited again , he searched web in recent year and read some articles about prophylactic effect of surgery on the formation of cancer in Barrett s esophagus , Do you recommend it ?

39
Bile acids can also cause double-strand DNA breaks and might contribute to carcinogenesis in patients with Barrett’s metaplasia, and PPIs do not prevent bile reflux. Antireflux surgery can prevent reflux of all gastric contents (acid and bile), but the best available data suggest that surgery is not more effective than PPI therapy in preventing cancer. Thus, antireflux surgery is not advised solely for protection against cancer
, but the best available data suggest that surgery is not more effective than PPI therapy in preventing cancer. Thus, antireflux surgery is not advised solely for protection against cancer.")
40
After first 3-5 year follow up endoscopic study , he expressed his sorrow about PPI complications ,and requested about non operational alternative for PPI , what is your recommendation?

41
Bard The first approved method of treating GERD was the Bard endoscopic sewing machine. The sewing machine is advanced to the GE junction (GEJ) under vision Suction is applied, which pulls a fold of tissue into the jaws of the device
 under vision Suction is applied, which pulls a fold of tissue into the jaws of the device.")
42
Curon’s Stretta In this method, a special catheter is delivered to the GEJ. A balloon inside the tip inflates, and inserts small hooks into the muscles. These hooks serve as antennae for applying radiofrequency heat directly into the muscle. The radiofrequency-induced burns scar down eventually. This scarring seems to create a reflux barrier.

Similar presentations











 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")


 AND HEARTBURN (ACID REFLUX)>")





>")



 Rory Loveland Paramedic class ’08-’09.>")


 Stomach ulcer or peptic ulcer is the damage of the protective layer (lining) of stomach or gastrointestinal tract It may be.>")


