Download presentation
Presentation is loading. Please wait.

1
Overview of Chemical and Biological Weapons/Terrorism Tucker Greene, MD, FAAEM, ACMT Cape Coral, FL

2
Introduction Long History of humans using both agents Long History of humans using both agents Precedents Precedents –Ancient »Middle Ages - Anthrax contaminated livestock –Recent »Southeast Asia – Tricothecenes »Iran/Iraq – Sarin »Arum Shryinko – Tokyo subway attack

3
Introduction Agent Progression Agent Progression –Chemical »Industrial process –Biological »Agents, offspring »toxins Different Results than predicted for both Different Results than predicted for both

4
Introduction Persistent v. Non-Persistent Biological: Persistent v. Non-Persistent Biological: –Persistent: Anthrax –Non-Persistent: Viruses Persistent v. Non-Persistent Persistent v. Non-Persistent –Persistent: Mustard, VX –Non Persistent: Phosgene, CN

5
Introduction Stability or Infectivity Stability or Infectivity –Anthrax Spores: stable, reasonably infective, lethal? –Tularemia, Q-Fever, Brucellosis: unstable, very infective, non-lethal

6
Introduction Biological Agents Biological Agents –Mimic other natural diseases –Usually incapacitating Chemical Agents Chemical Agents –Exaggerate or Isolate a particular clinical feature of chemical agents in general –I.e organophosphates and nerve agents KEY: Mechanism of Intoxication KEY: Mechanism of Intoxication –Dermal, Inhalation, Ingestion

7
(brief) History Definitions Definitions –Kill: Soman, VX –Injure: Phosgene –Incapacitate: CS, BZ Countermeasures Countermeasures –Until WWI, US not concerned or interested
 History Definitions Definitions –Kill: Soman, VX –Injure: Phosgene –Incapacitate: CS, BZ Countermeasures Countermeasures –Until WWI, US not concerned or interested")
8
(brief) History Pre-WWI Developments Pre-WWI Developments Ancient: hellebore, mandrake in water 1000-200 b.c Ancient: hellebore, mandrake in water 1000-200 b.c Recent: Recent: –1700-1850: Chlorine, Mustard (dichloroehtylsulfide), chloropicrin –Civil War: Dougherty: Chlorine, 3 qts in shell
 History Pre-WWI Developments Pre-WWI Developments Ancient: hellebore, mandrake in water b.c Ancient: hellebore, mandrake in water b.c Recent: Recent: – : Chlorine, Mustard (dichloroehtylsulfide), chloropicrin –Civil War: Dougherty: Chlorine, 3 qts in shell")
9
(brief) History Biological: Biological: –Mongols in Caffa 1346, bubonic plague bodies –Spanish v French 1495, Leprosy Blood in Naples against French
 History Biological: Biological: –Mongols in Caffa 1346, bubonic plague bodies –Spanish v French 1495, Leprosy Blood in Naples against French")
10
Protection, Control US Civil War: agreed but not adhered to US Civil War: agreed but not adhered to Hoffman Respirator in 1866 Hoffman Respirator in 1866 Archduke Francis murder in 1914, control among WWI participants Archduke Francis murder in 1914, control among WWI participants

11
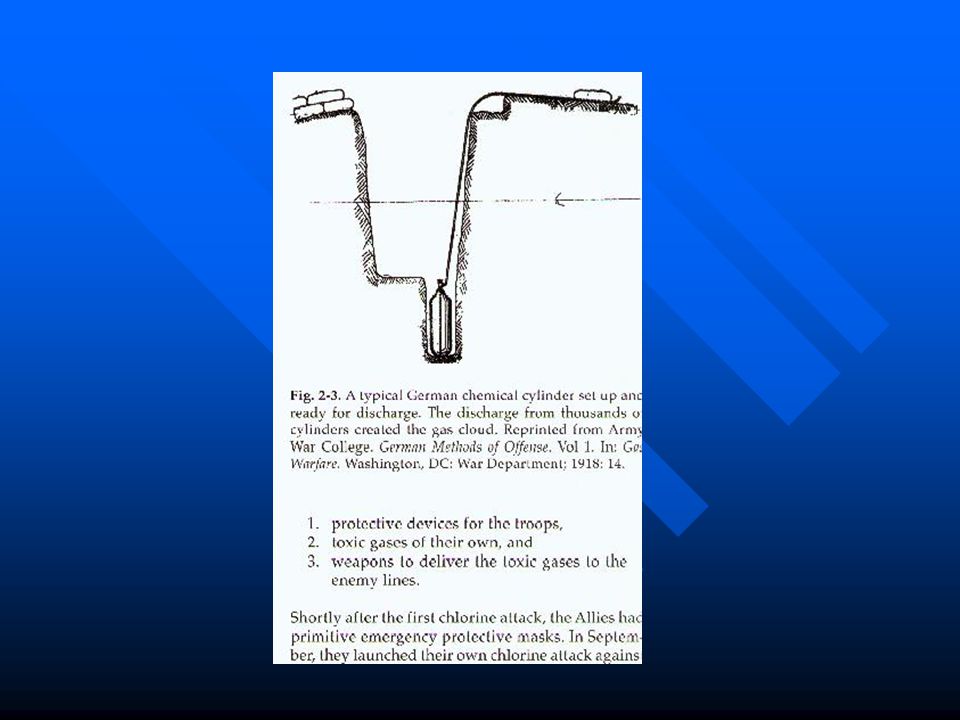
Protection, Control WWI Chemical WWI Chemical –German Wilhelm: Gas cloud due to lack of shells –Allies: Chlorine response Biological: Biological: –Both sides attempting to use anthrax and glanders

12
US Chemical Warfare Service (CWS) and New Age Chemical Agents placed in Artillery Shells Chemical Agents placed in Artillery Shells –Cl2, Choropicrin, Mustard, Phosgene Biological Agents Biological Agents –Ricin –Brucellosis
 and New Age Chemical Agents placed in Artillery Shells Chemical Agents placed in Artillery Shells –Cl2, Choropicrin, Mustard, Phosgene Biological Agents Biological Agents –Ricin –Brucellosis")
13
US Chemical Warfare Service (CWS) and New Age Detection, Alarms, Treatment Detection, Alarms, Treatment –Human and Animal –Treatment »Inhalation Vomiting Vomiting Venesection Venesection KI KI Steam Tents Steam Tents »Skin: ZnO, Starch, Boric Acid, Calamine
 and New Age Detection, Alarms, Treatment Detection, Alarms, Treatment –Human and Animal –Treatment »Inhalation Vomiting Vomiting Venesection Venesection KI KI Steam Tents Steam Tents »Skin: ZnO, Starch, Boric Acid, Calamine")
21
US Chemical Warfare Service (CWS) and New Age Biologicals get new start in late 1930s after skepticism Biologicals get new start in late 1930s after skepticism Nuclear Age comes and biologicals take a back seat (where someone was sitting) Nuclear Age comes and biologicals take a back seat (where someone was sitting) Chemical Warfare takes second Priority Chemical Warfare takes second Priority –Edgewood (Aberdeen), MD –McClellan, AL –Rocky Mountain, CO
 and New Age Biologicals get new start in late 1930s after skepticism Biologicals get new start in late 1930s after skepticism Nuclear Age comes and biologicals take a back seat (where someone was sitting) Nuclear Age comes and biologicals take a back seat (where someone was sitting) Chemical Warfare takes second Priority Chemical Warfare takes second Priority –Edgewood (Aberdeen), MD –McClellan, AL –Rocky Mountain, CO")
22
US Chemical Warfare Service (CWS) and New Age Near ending of CWS: Near ending of CWS: –Binary weapons –Disposal at Sea –Disseminated Danger of lesser nations? –Johnston Atoll Destruction program

23
US Chemical Warfare Service (CWS) and New Age Gulf War Gulf War –Iraq with known biological and chemical weapons –MARK I Kit »2-PAM, atropine, valium –Pryidostigmine Bromide –Kamisiyah arsenal detonation »Mustard »sarin
 and New Age Gulf War Gulf War –Iraq with known biological and chemical weapons –MARK I Kit »2-PAM, atropine, valium –Pryidostigmine Bromide –Kamisiyah arsenal detonation »Mustard »sarin")
24
US Chemical Warfare Service (CWS) and New Age Aum Shinrikyo Cult Aum Shinrikyo Cult –Experiments with botulinum and anthrax in subways yields no impact –Later sarin attack kills 50 but injures 5000
 and New Age Aum Shinrikyo Cult Aum Shinrikyo Cult –Experiments with botulinum and anthrax in subways yields no impact –Later sarin attack kills 50 but injures 5000")
25
DEFENSE (WWI) Mask against Chemical Agents Mask against Chemical Agents Plume identification Plume identification Mobile Decontamination Mobile Decontamination –5% of Division strength Psychological aspect of persistence: mustard (low volatility, low dose effect, still used) Psychological aspect of persistence: mustard (low volatility, low dose effect, still used) –“Gas Mania”
 Mask against Chemical Agents Mask against Chemical Agents Plume identification Plume identification Mobile Decontamination Mobile Decontamination –5% of Division strength Psychological aspect of persistence: mustard (low volatility, low dose effect, still used) Psychological aspect of persistence: mustard (low volatility, low dose effect, still used) – Gas Mania")
26
DEFENSE (WWI) Mustard Mustard –Conjunctivitis –Skin burns –Inhalation (worse than phosgene and chlorine) –Accounted for up to 30% of casualties but 1500 deaths/52,900 US AEF Force deaths
 Mustard Mustard –Conjunctivitis –Skin burns –Inhalation (worse than phosgene and chlorine) –Accounted for up to 30% of casualties but 1500 deaths/52,900 US AEF Force deaths")
27
DEFENSE (WWII) Germans thought US possessed secret gases beyond GA< GB< GD and feared reprisal Germans thought US possessed secret gases beyond GA< GB< GD and feared reprisal Continued Vigilance Continued Vigilance –Walt Disney example
 Germans thought US possessed secret gases beyond GA< GB< GD and feared reprisal Germans thought US possessed secret gases beyond GA< GB< GD and feared reprisal Continued Vigilance Continued Vigilance –Walt Disney example")
28
Chemical Warfare and the HealthCare Provider

29
National Warfare Capability

30
Chemical Warfare Agents

32
Nerve Agents

33
Organophoshates History History –Ethanol + Phosphoric Acid –Tabun - GA –Sarin - GB –Soman- GD –VX

34
Organophosphates Examples Examples

35
Organophosphates Absorption Absorption –inhalation –dermal –oral Activation Activation –ie parathion Metabolism Metabolism –cholinesterase

37
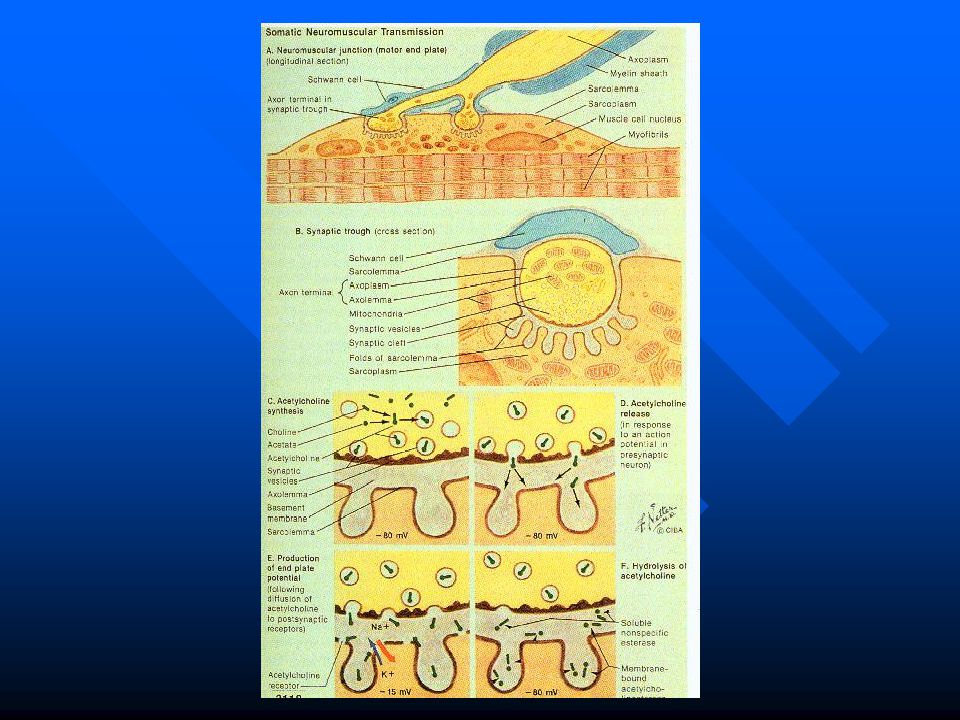
Mechanism of Toxicity Mechanism of Toxicity Organophosphates

38
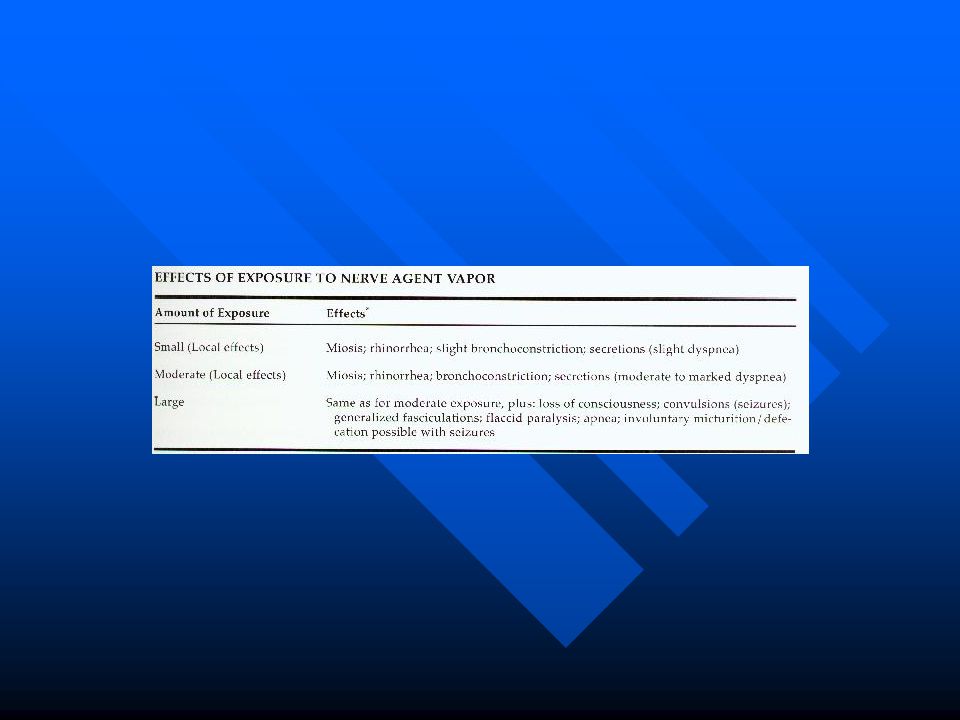
Organophosphates Clinical Effects Clinical Effects

39
–Muscarinic (postganglionic parasympathetic) »“SLUDGE” »miosis, bronchorrhea, bradycardia –Nicotinic (neuromuscular junction) –Nicotinic (autonomic ganglion ) Organophosphates
 » SLUDGE »miosis, bronchorrhea, bradycardia –Nicotinic (neuromuscular junction) –Nicotinic (autonomic ganglion ) Organophosphates")
40
Organophosphates Management/Treatment Management/Treatment –Decontamination –Stabilization –Antidotes »Atropine »Pralidoxime Pralidoxime

41
Organophosphates Delayed Toxicity Delayed Toxicity –Intermediate Syndrome –Peripheral Neuropathy »Tri -o-cresyl phosphate (TOCP) »Tri -o-cresyl {tolyl} phosphate TOTP »Neurotoxic Esterase
 »Tri -o-cresyl {tolyl} phosphate TOTP »Neurotoxic Esterase")
42
Organophosphates Delayed Toxicity Delayed Toxicity –Intermediate Syndrome –Peripheral Neuropathy »Tri -o-cresyl phosphate (TOCP) »Tri -o-cresyl {tolyl} phosphate TOTP »Neurotoxic Esterase
 »Tri -o-cresyl {tolyl} phosphate TOTP »Neurotoxic Esterase")
43
Organophosphates Laboratory Laboratory –Don’t Need To Treat!!! –Cholinesterase Levels »RBC v Plasma »Variation from Baseline

47
Pretreatment Pyridostigmine (carbamate) Pyridostigmine (carbamate) Used in Gulf War Used in Gulf War
 Pyridostigmine (carbamate) Used in Gulf War Used in Gulf War")
48
Vesicants

54
Sulfur Mustard

61
Phosgene

62
Lewisite

63
Inhalational Agents

64
Upper Airway Upper Airway –Water soluble Middle Airway Middle Airway Alveolar Alveolar –Non-soluble in water Cellular Asphyxiants Cellular Asphyxiants

65
Inhalational Agents

68
Cyanide Treatment Cyanide Treatment –Nitrites –Thiosulfate –Hydroxycobalamin –Hyperbaric O2

69
Incapacitating Agents

70
Anticholinergics Anticholinergics LSD, other Indoles LSD, other Indoles Opiates Opiates

71
Riot Control Agents Rapid Onset, Upper Airway and GI Symptoms Rapid Onset, Upper Airway and GI Symptoms CS (o-Chlorobenzylidene) CS (o-Chlorobenzylidene) CN (1-Chloroacetophenone) CN (1-Chloroacetophenone) Other Other –DM (Diphenylaminearsine) –CR (Dibenzo(b,f)-1:4oxazepine –CA (Bromobenzylcyanide)
 CS (o-Chlorobenzylidene) CN (1-Chloroacetophenone) CN (1-Chloroacetophenone) Other Other –DM (Diphenylaminearsine) –CR (Dibenzo(b,f)-1:4oxazepine –CA (Bromobenzylcyanide)")
72
Riot Control Agents CS CS –Solid, low Vp –“Tear Gas” –Airway irritation –Conjunctival tearing –Dermal effects can cause blistering –IV/Oral can liberate cyanide moeities CN –Solid powder –Same symptoms as CS –Highly sensitizing to skin with deaths reported with large exposures

73
Riot Control Agents Treatment Treatment –Alkaline decon of skin; no hypochlorite –Topical steroids for skin –Local anesthetics for eyes

74
Field Management of Chemical Casualties Hot Zones Hot Zones Clean v Decontamination areas Clean v Decontamination areas Counter-current or Reverse Airflow for Decontamination Areas Counter-current or Reverse Airflow for Decontamination Areas Triage Triage –Potential ID –Look for Combined Agents/Injuries –Difficult to Treat Combinations

77
Decontamination Chemical Chemical –Desirable Traits for Dermal Decon –Physical Removal –Aqueous –Adsorbent Biological –Dermal not as Important (T-2 is exception) –Hypochlorite –Environmental UV
 –Hypochlorite –Environmental UV")
78
BIOLOGICALS

79
History Secret US Weapons Program Secret US Weapons Program Response to Japan during WWII Response to Japan during WWII –Stockpiling 400 kg anthrax bombs Experiments Experiments –San Francisco (Serratia marcenscens) –New York Subway (B. subtilis) –African Americans exposed to Aspergillus f.
 –African Americans exposed to Aspergillus f..")
83
Use of Biological Weapons Requirements Requirements –Ease of Production –Lethality/Incapacitation –Particle size –Ease of Dispersion –Stability Methods of Delivery –Food –Water –Air

84
Use of Biological Weapons Advantage/Disadvantage Advantage/Disadvantage –Predominantly concerns of the pathogen occurring in aggressors –Persistence –Insidious, low cost, minimal detection Tactical Concerns –Hard to Trace or Fingerprint –Terrorism as we now have known the anthrax cases

85
Biological Agents Anthrax Anthrax Plague Plague Tularemia Tularemia Brucellosis Brucellosis Q Fever Q Fever Smallpox Viral Encephalitides Viral Hemorrhagic Fevers Toxins –Plants –Animals –Mycotoxins

86
Anthrax History History –Bacillus anthracis –Zoonotic:goats sheep, cattle, swine, horses –5 th and 6 th plagues of Exodus –Isolated 1876: Koch –Vaccine 1881: Pasteur Organism –1-5 mic x 5-10 mic –Capsule forms in presence of CO2, HCO3 –Sporulation occurs in dead tissue exposed to oxygen

87
Anthrax Epidemiology Epidemiology –1958: 20-100,000 cases worldwide –Since 1970 one case/decade –Woolsorter’s Disease Pathogenesis –Antiphagocytic Capsule –Lethal Toxin –Edema Toxin –Mechanism by cell binding and then active toxin

88
Anthrax Clinical Disease Clinical Disease –Cutaneous –Inhalational –Gastointestinal –Meningeal Diagnosis –CLINICAL SUSPICION OF EXPOSURE

89
Anthrax Treatment Treatment –Pen G –Doxycycline –Ciprofloxacin –Many other possibly effective Recombinants may possess resistance as the native vegetative state has lactamases

90
Plague History History –Pandemics of the 6 th, 14 th, 20 th century –24 Million died from 1346-1352 –Endemic throughout history –Zoonotic »Enzoontic »Epizootic Infectious Agent –Yersinia pestis –Gram-neg, non- sporulating, coccobacillus –pH 6 antigen induced at low pH for virulence –Antiphagocytic capsule –Complex interspecies toxins

91
Plague Epidemiology Epidemiology –Oriental rat flea most common vector –Multiple animals serve as vectors –US rat squirrel fleas –Endemic in Western US Pathogenesis –1-10 organism can infect via bites –Multiple Virulence factors –Spread via lymph –Sepsis occurs when untreated to all organs

92
Plague Clinical Features Clinical Features –80% as bubonic form –10% as sepsis –10% as pulmonary –As warfare agent presentation would be bubonic and pulmonary Generally present as gram negative infection with plague specific features

93
Plague Diagnosis Diagnosis –Differential »Cat Scratch »Tularemia »LGV »Chancroid »TB »Streptococccal »Rickettsiae Lab Confirm –Aspiration of Bubo –Wright-Giemsa, Gram Stain

94
Plague Treatment Treatment –Isolation for first 48 hrs of treatment –Streptomycin, ceftriaxone, chloramphenical, –Doxycyclcine all acceptable –If treated early, buboes do not require drainage –Postexposure Prophylaxis: Doxycycline –Immunization: high risk individuals

95
Tularemia History History –Discovered in 1911 in Tulare County, California by McCoy –Edward Francis discovered deer fly transmission –High infectivity after aerosolization Agent –Francisella tularensis –Obligate aerobe, coccobacillus –Two biovars: US isolate highly virulent for rabbits, humans

96
Tularemia Epidemiology Epidemiology –Principle reservoir is the tick in the US –Abdominal Pain, Pharyngitis, from contaminated water in areas where water mammals live (non- US) Pathogenesis –Possibly capsular –Unclear, no toxins –Spreads through skin, mucous membranes, GI –5-10 organisms –Humoral response by MHC II mediated T- cell immunity
 Pathogenesis –Possibly capsular –Unclear, no toxins –Spreads through skin, mucous membranes, GI –5-10 organisms –Humoral response by MHC II mediated T- cell immunity")
97
Tularemia Clinical Features Clinical Features –Incubation 3-6 day –Ulceroglandular 75% »Skin or mucous membranes, nodes >1cm –Typhoidal 25% »Smaller nodes »Non-mucous membranes Multiple Const/Syst complaints –Fever –HA –Chills –Abdominal pain –Fluctuant Lymph nodes (drainage)
")
98
Tularemia Diagnosis Diagnosis –Difficult serology and growth medium procedures –ELISA most reliable Treatment –Streptomycin –Aminoglycosides –Chloramphenicol –Tetracyclines Prophylaxis –Doxycycline

99
Brucellosis History History –Zoonotic infection »Domestic »Wild –Animal Products, contact with infected animals, aerosols –Relapsing Fever, associated with ruminant abortion –US actively developed warfare agent with Brucella Agent –Non-toxic, nonsporulating,aerobic, Gram-neg, coccobacilli –6 species with several biovars –Unusual LPS component of cell membrane

100
Brucellosis Epidemiology Epidemiology –Transmission at abortion, slaughter, and milk –Highly infectious in lab workers who work with the Brucella –Fewer than 200 fatal cases/yr in US Pathogenesis –Enter thru skin, GI, mucous membranes –Phagocytized by WBC but carried to lymph nodes –Placenta may carry 10 10 bacteria/gram

101
Brucellosis Clinical Features Clinical Features –diverse, variability –3d to weeks incubation –Neuropsychiatric along with fever, cough, arthritis –Mild lab abnormalities Diagnosis –Serum agglutination –PCR –IgG

102
Brucellosis Treatment Treatment –Doxycycline –Streptomycin –Aminoglycosides Prophylaxis Prophylaxis –Prevention (no-vaccine) –Doxycycline
 –Doxycycline")
103
Q Fever History History –1937 discovery –Zoonotic –Coxiella Burnetii –50 g of dried powder equal to casualty rate of anthrax or tularemia –Multiple wars with soldiers infected from living in barns, near livestock Agent –Close relative of Legionella, not true rickettsiae –Obligate intracellular pathogen –Spore-like formation –Phase I/II

104
Q Fever Epidemiology Epidemiology –Extremely infectious –Single organism capable of disease –Multiple hosts, arthropod to human –Human infection from livestock same as Brucellosis but also shed in urine –Urine persistence can infect from objects such as straw Pathogenesis –Inhalation of aerosols –Phagocytosis with eventual lysis and release

105
Q Fever Clinical Features Clinical Features –Incubation 10-40 days –Asymptomatic seroconversion –Acute Disease: »Chill,rigors,retroorbital HA »Fever, myalgias –Chronic: endocarditis Diagnosis –Serological »Comp Fixation »Indir Flour Ab »ELISA

106
Q Fever Treatment Treatment –Tetracyclines –Macrolides –Quinolones in chronic disease Prophylaxis Prophylaxis –Vaccine –Doxycycline

107
Smallpox Variola – ds-DNA, Orthopox Virus Variola – ds-DNA, Orthopox Virus –Major: 30% mortality, Asia, Africa –Minor: 1% mortality, Europe, South America Possible to recover Smallpox from preserved cadavers or recombinant with monkeypox Possible to recover Smallpox from preserved cadavers or recombinant with monkeypox

108
Smallpox Pathogenesis and Clinical Features Pathogenesis and Clinical Features –Highly stable and infective for long periods outside of host –Fever, followed by rash 3-6 days later –Rash period is infective, lymphoid dissemination »Head to toe spread –Incubation avg = 12 days –Sx: fever, delerium, backache, cough (aerosol) –Hemorrhagic and Flat-type higher mortality
 –Hemorrhagic and Flat-type higher mortality")
109
Smallpox Diagnosis and Treatment Diagnosis and Treatment –Dx: Guarnieri bodies = viral aggregation –Distinguish subclinical Smallpox from Varicella –Quarantine for 3 days for rash development post exposure –Vaccines »Vaccinia »VIG within 7 days of disease; care if recently vaccinated

110
Viral Encephalitides

112
Zoonotic viruses Zoonotic viruses Aerosolization transmission as well as insect; route of biological warfare agent a source of concern Aerosolization transmission as well as insect; route of biological warfare agent a source of concern Each VE has distinct but similar incubation, symptoms and mortality Each VE has distinct but similar incubation, symptoms and mortality Vaccines key to management of VEE, WEE, EEE Vaccines key to management of VEE, WEE, EEE

113
Viral Hemorrhagic Fevers

115
Toxins

117
pg607

118
Toxins General Discussion and Overview General Discussion and Overview –Mechanism of Toxicity –Diagnosis/Recognition –Treatments/Antidotes

Similar presentations





























 USN Preventive Medicine Resident Johns Hopkins Bloomberg School of Public Health.>")













. Center for Food Security and Public Health Iowa State University - 2004 Overview Organism History Epidemiology Transmission.>")



