Download presentation
Presentation is loading. Please wait.

1
Making a Difference: The Lean Culture and Results at Denver Public Health Judith Shlay, MD, MSPH Heather Weir, MPH, RD

2
Questions for the group Who uses Lean currently? Who has been using Lean for > 2 years? Who is considering using Lean? Who would like to know what Lean is? Who has ever heard of an A3?

3
Objectives Background of Denver Health and Denver Public Health Reason for Action Where we’ve been Recent progress in 2013 Structure of QI at DPH QI Projects

4
Denver Health Overview Large, urban, integrated, public safety-net institution which includes: – 911 medical response system – 525 bed acute care hospital with a Level 1 Trauma Center – Denver Public Health department – 8 family health centers – 15 school-based clinics – 100 bed non-medical detoxification facility – call center (includes a regional poison center, drug and nurse advice line) – correctional care and a center for the medical response to terrorism, mass casualties and epidemics Approximately 65% of patients <185% federal poverty level >70% members of ethnic minorities Substantial amount of uncompensated care
 – correctional care and a center for the medical response to terrorism, mass casualties and epidemics Approximately 65% of patients <185% federal poverty level >70% members of ethnic minorities Substantial amount of uncompensated care")
5
Denver Cares Correctional Care Denver Health Medical Center 911911 Family Health Centers Regional Poison Center & Nurseline Denver Health Medical Plan School- based Health Centers Rocky Mtn Center for Medical Response to Terrorism Public Health Rky Mtn Regional Trauma Ctr HIT Denver Cares Public Health Employed Physicians Legend: Bright Green – Pt Revenue Blue – City Orange – DHMP Lavender – Grants Dark Red - RMPDC

6
Right People Right Environment Right Communication and Culture Right Process Right Reward Getting It Right… Perfecting The Patient Experience

7
Principles of Lean The customer defines value Deliver value to the customer on demand and without waste Standardize to solve and improve Transformational learning requires a deep personal experience Mutual respect and shared responsibility enable higher performance

8
What is a Lean Management System? Lean is a systematic approach of continuous improvement, based on the Toyota Production System (TPS) of LEAN principles and LEAN tools, used for the identification and elimination of waste Lean Thinking is the operation of a business from the patient/customer’s definition of value…not from the organization’s or its assets Lean Management System is the mechanism to develop, sustain, and improve processes over time
 of LEAN principles and LEAN tools, used for the identification and elimination of waste Lean Thinking is the operation of a business from the patient/customer’s definition of value…not from the organization’s or its assets Lean Management System is the mechanism to develop, sustain, and improve processes over time.")
9
Current Denver Health Lean Management System Focus Lean Management System – Strategic Alignment – Standard Work – Visual Management – Continuous Improvement (Lean Tools) Root Cause Problem Solving (A3 deployment) – Leadership Standard Work
 Root Cause Problem Solving (A3 deployment) – Leadership Standard Work")
11
Strategic Planning

12
Strategic Planning Process Organize (Aug-Sept) Assess (Sept-Oct) Facilitated Planning Session (Oct) Develop Action Plans (Nov-Dec) Implement (starting Jan 2014)
 Assess (Sept-Oct) Facilitated Planning Session (Oct) Develop Action Plans (Nov-Dec) Implement (starting Jan 2014)")
13
DPH Overview Provides public health services for the City and County of Denver – Direct disease control services (e.g., tuberculosis, HIV, STD clinics and immunizations) – Epidemiology and informatics – Preparedness – Vital records/vital statistics – Denver Prevention Training Center – STD/HIV/TB prevention activities – Immunization outreach – Health promotion division Tobacco control Maternal child and youth health Healthy eating and active living prevention activities Injury prevention
 – Epidemiology and informatics – Preparedness – Vital records/vital statistics – Denver Prevention Training Center – STD/HIV/TB prevention activities – Immunization outreach – Health promotion division Tobacco control Maternal child and youth health Healthy eating and active living prevention activities Injury prevention")
14
The Core Functions and Essential Services Monitor Health Diagnose and Investigate Inform, Empower, Educate Inform, Empower, Educate Mobilize Community Partnerships Mobilize Community Partnerships Develop Policies Enforce Laws Link To / Provide Care Link To / Provide Care Assessment Develop and Apply PH Science Assure Competent Workforce Evaluate Policy Development Assurance Epidemiology Improve Health Quality CORE FUNCTIONS:

15
Core Functions of Public Health Implications for Quality Assessment Policy Development Assurance Priority Areas WORK WELL-DONE WORTHY Improve Health Protect Health Emergency- Prepared

16
Elements of Public Health Quality WorthyWorkWell-Done Prioritization Evidence Reviews Performance Measures Important Health Issues High-Value Interventions Accountable Performance Continuous Quality Improvement

17
History of QI at DPH 2011 Customer Satisfaction QI focus of Program Director/Mgr meeting 2012 February – Results Based Accountability (RBA) training at retreat June- 2As+R QI project in STD Clinic (NNPHI Grant) 2012 November- ASI Grant to hire QI Coordinator
 training at retreat June- 2As+R QI project in STD Clinic (NNPHI Grant) 2012 November- ASI Grant to hire QI Coordinator")
18
2013 Progress 2013 January – QI Coordinator starts February- Quality Committee (QC) and Performance Management Team start meeting; onFocus software 1 st used with DPH plan March – QI Assessment Survey 2013 June – QI Plan finalized August – QC completed 1 st dept wide QI project (customer satisfaction) September – Started the ‘Oppy Award’; onFocus expanded to Birth and Death Records (1 st pilot) 2013 October – onFocus pilot with the Infectious Disease Clinic (2 st pilot); Scorecard development/improvement November – 80% of programs have started a QI project (YTD: 4 completed/11 in progress); planning for 2014
 and Performance Management Team start meeting; onFocus software 1 st used with DPH plan March – QI Assessment Survey 2013 June – QI Plan finalized August – QC completed 1 st dept wide QI project (customer satisfaction) September – Started the ‘Oppy Award’; onFocus expanded to Birth and Death Records (1 st pilot) 2013 October – onFocus pilot with the Infectious Disease Clinic (2 st pilot); Scorecard development/improvement November – 80% of programs have started a QI project (YTD: 4 completed/11 in progress); planning for 2014")
19
Lean Work at Denver Public Health The nuts and bolts

20
Performance Management Framework

21
Quality Committee Lean Events - RIEs, 6S Lean Black Belts QI projects PDSAs QI Plan QI training Quarterly Reports BI Tool/Dashboards Visual Management Boards Website – internal/external onFocus Scorecards Results Accountability Population Indicators Program Performance Measures Customer Satisfaction Surveys Strategic Planning – metrics/achievement indicators QI Assessment (all-staff) Performance Management Self- Assessment Public Health Accreditation Board (PHAB) standards Healthy People 2020 National and State benchmarks Program goals and targets to set expectations Performance Standards Performance Measurement Quality Improvement Reporting of Progress Leadership & Culture DPH – Performance Management System
 Performance Management Self- Assessment Public Health Accreditation Board (PHAB) standards Healthy People 2020 National and State benchmarks Program goals and targets to set expectations Performance Standards Performance Measurement Quality Improvement Reporting of Progress Leadership & Culture DPH – Performance Management System")
22
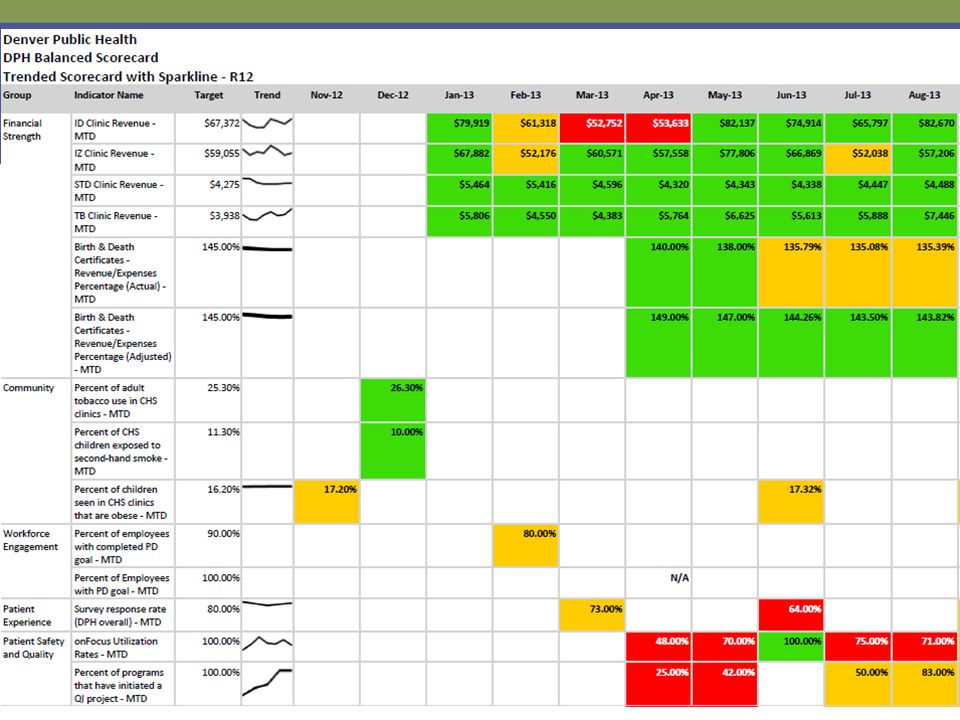
onFocus (Performance Management Software) On Focus spreadsheet
 On Focus spreadsheet")
24
Identify what you want to improve or are concerned about Is there data available? Are there standards to compare your data to? Start an A3 Use the Word or PPt template* Develop a concise Reason for Action and why change is needed (Complete step 1 of the A3) Decide on a Project Leader and get buy- in/sponsorship from management Complete steps 2-3 of the A3 2. Initial State 3. Target State Project team activity Assemble the project team May be a larger group (involve those who do and are affected by the work) List the QI Project on the DPH QI Project Tracking list* Complete steps 4-9 of the A3 4. Gap Analysis 5. Solution Approach 6. Rapid Experiments (use the PDSA form*) 7. Completion Plans 8. Confirmed State 9. Insight Update project information on the DPH QI Project Tracking list* Denver Public Health – Process for Quality Improvement Projects *All forms, resources, and the QI Project Tracking list are available on the Pulse/Intranet (DPH subsite) - DPH Performance Management siteDPH Performance Management site (QI Project folder) Ask for help! Contact Heather Weir, QI Coordinator (x23582) and your Quality Committee representative when starting a QI project
 Decide on a Project Leader and get buy- in/sponsorship from management Complete steps 2-3 of the A3 2. Initial State 3. Target State Project team activity Assemble the project team May be a larger group (involve those who do and are affected by the work) List the QI Project on the DPH QI Project Tracking list* Complete steps 4-9 of the A3 4. Gap Analysis 5. Solution Approach 6. Rapid Experiments (use the PDSA form*) 7. Completion Plans 8. Confirmed State 9. Insight Update project information on the DPH QI Project Tracking list* Denver Public Health – Process for Quality Improvement Projects *All forms, resources, and the QI Project Tracking list are available on the Pulse/Intranet (DPH subsite) - DPH Performance Management siteDPH Performance Management site (QI Project folder) Ask for help. Contact Heather Weir, QI Coordinator (x23582) and your Quality Committee representative when starting a QI project.")
25
Why are we doing this? What is the burning platform? What is the chief complaint? What are the attributes of the Initial State (qualitative and quantitative)? Use visuals. What are the attributes of the Target State (qualitative and quantitative)? Use visuals. Have metrics that are defined and achievable. What holds us back from the Target State? What are the root causes of these road blocks? What is the hypothesis to address the root cause (If/Then statements)? Does solution approach link well with root causes? Expect the Solution Approach to not be perfect – test them! Are Rapid Experiments achieving desired results? Action Plan – who, what, when Check that Completion Plan is on track at follow-up meetings Are Confirmed State metrics in place and do they validate the target state? Do insights show key lessons learned and identify future opportunities?
. Use visuals. What are the attributes of the Target State (qualitative and quantitative). Use visuals. Have metrics that are defined and achievable. What holds us back from the Target State. What are the root causes of these road blocks. What is the hypothesis to address the root cause (If/Then statements). Does solution approach link well with root causes. Expect the Solution Approach to not be perfect – test them. Are Rapid Experiments achieving desired results. Action Plan – who, what, when Check that Completion Plan is on track at follow-up meetings Are Confirmed State metrics in place and do they validate the target state. Do insights show key lessons learned and identify future opportunities .")
26
QI Projects

27
Rapid Improvement Event (RIE) – Vaccine Inventory Management Reason for Action: adhere to federal/state laws improving/creating standard work outgrown current Vaccine Registry (Vaxtrax) inefficient use of resources
 – Vaccine Inventory Management Reason for Action: adhere to federal/state laws improving/creating standard work outgrown current Vaccine Registry (Vaxtrax) inefficient use of resources")
28
Initial State Target State

29
Results

30
The number of private vaccine orders decreased to one time a month Decreased the time for the nurse ordering Used par levels to determine how many vaccines to order

31
Results 100% charts were reviewed 30% errors in September to 10% in April Errors found primarily in not indicating which program they are from (Travel, 317 funded, Tdap cocooning)
")
32
Return on Investment

33
STD Clinic – Ask, Advise, Refer (2As+R) Root cause analysis BarriersPotential Solutions Competing priorities/Tobacco is not STI-related Education Staff timeStreamlined, standardized work process Patient receptivityEducation and training No system to document tobacco use and referrals Create a standard work process Change the EMR Perceived lack of cessation resourcesEducation No incentive for clinic staff buy-inEducation: Cessation saves Monetary incentives for staff Potentially able to bill
 Root cause analysis BarriersPotential Solutions Competing priorities/Tobacco is not STI-related Education Staff timeStreamlined, standardized work process Patient receptivityEducation and training No system to document tobacco use and referrals Create a standard work process Change the EMR Perceived lack of cessation resourcesEducation No incentive for clinic staff buy-inEducation: Cessation saves Monetary incentives for staff Potentially able to bill")
34
STD Clinic – Ask, Advise, Refer (2As+R) The current state and the ideal state
 The current state and the ideal state")
35
STD Clinic – Ask, Advise, Refer (2As+R) Rapid Experiments October 24November 1November 15December 1 Paper Pilot in the Clinic Clarified questions, re-training & provided additional resources Attend clinic huddles weekly to reinforce, encourage Amended the EMR
 Rapid Experiments October 24November 1November 15December 1 Paper Pilot in the Clinic Clarified questions, re-training & provided additional resources Attend clinic huddles weekly to reinforce, encourage Amended the EMR")
36
STD Clinic – Ask, Advise, Refer (2As+R) Results
 Results")
37
Flu Vaccines - in all DPH clinics

38
Shared Drive Clean Up Projects Reason for action: – reduce time in finding files – ensure critical files are accessible/backed up – correct permissions on folders

39
Birth and Death Records – Phone Orders New process Process mapping – staff identified 14 areas of improvement

40
Birth and Death Records – Phone Orders

42
Contact Information Judith Shlay, MD, MSPH 605 Bannock St., MC 2600 Denver, CO 80220 (303) 602-3714 judith.shlay@dhha.org Heather Weir, MPH, RD 605 Bannock St., MC 2600 Denver, CO 80220 (303) 602-3582 heather.weir@dhha.org
 Heather Weir, MPH, RD 605 Bannock St., MC 2600 Denver, CO (303)")
Similar presentations