Download presentation
Presentation is loading. Please wait.

1
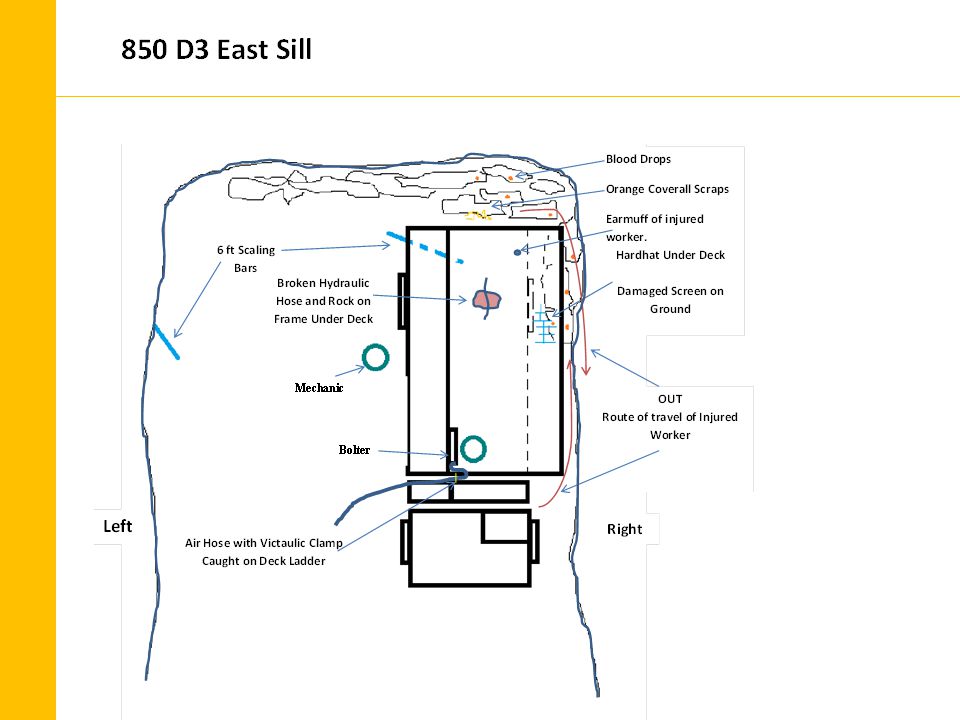
L OST T IME I NJURY R EVIEW AND D ISCUSSION 15 July, 2014: At approx. 11:45 hrs the crew was just finishing up in the TM 850 D3 East Sill and preparing to screen the face. The crew utilized a scissor lift to install the ground support on this particular day and everything was progressing fine. During the process the Front Line Supervisor and the Safety Coordinator visited the heading and ground support was being installed above and beyond the required standard. Due to talc conditions in the heading, the crew opted to extend the screen further down the right wall than was required by the print and rebar was being used to pin the screen on the walls as opposed to split sets.

2
L OST T IME I NJURY C ONT. Before they could install the screen on the face, a hydraulic hose broke underneath the deck near the rear axle and they were unable to continue. A mechanic was called to the site and climbed under the unit to further assess the situation. He discovered that there were several rocks on top of the rear axle and tried to remove them by hand, but they were too big and awkward. The deck was fully lowered at the time and attempts to raise it were unsuccessful because the deck got hung up on the rear corner of the back wall and could not be fully raised.

3
L OST T IME I NJURY C ONT. The deck was then side shifted to the right and when raised, the railing caught the wall near the shoulder of the drift at the back corner. The bolter attempted to side shift the platform to the left in order to clear the wall, but the Victaulic clamp on the bull hose was catching the ladder, preventing the deck from being side shifted to the left. The intention at this time was to raise the deck high enough to install the safety pins for the platform. The unit was then shut down because of continual oil loss through the broken hose. The mechanic then tried to remove the rocks using a scaling bar from the left side of the deck, the injured worker asked for a scaling bar from the bolter on the deck and proceeded down the right wall towards the face.

4
L OST T IME I NJURY C ONT. The bolter saw the face start to fail and hollered a warning, the mechanic immediately retreated away from the face and heard the injured worker yell. Loose had fell from the face struck the worker on the head and shoulder and pushed him into the back of the deck. The bolter proceeded around the right side of the deck and he got as far as the rear wheel where he could see the injured worker crawling out along the right side of the wall. The bolter and mechanic loaded the injured worker in a Toyota and brought him to surface where he was transported to hospital for treatment.

5
I NJURIES 17 stitches to close wound in the back of his head 16 stitches to close puncture wounds on his neck and shoulder 12 broken ribs, front and back Left punctured lung and right collapsed lung requiring drain tubes 2 broken vertebrae in lower back (Transverse Processes which are the small tabs on the vertebrae) 10 days in hospital, 6 in ICU Still not fully recovered and is on modified duties but making steady progress to a full recovery and returning to full duties. *Shared with Permission

6
L OST T IME I NJURY I NVESTIGATION Underlying Causes: Failure to secure and make safe, Improper position for the task, poor judgment, preoccupation or frustration, failure to warn, improper attempt to save time, ground conditions. Remedial Action: The accident was reviewed with all U/G crews at both sites stressing the importance of not exposing yourself to unsupported ground. The heading was shut down pending an investigation. The MOL attended the scene on July 18th. It was reinforced with the crews that working safely, takes precedence over production.

8
R ECOMMENDATIONS 1. Crews are to notify their Supervisor when equipment break downs occur. In areas where adequate ground control has not been completed or other hazards exist, the equipment shall be moved to a safe location. Where the equipment cannot readily be moved, the Supervisor will provide written instructions on the Zero Harm Safety Card. A SOP will be developed to provide guidelines and will require Supervisory notification by the crew. 2. A mechanic servicing equipment in the field is to ensure that a production supervisor has been contacted and additional written instructions have been given (indicated on the Zero Harm Safety Cards) for work on equipment in areas where adequate ground control has not been completed or other hazards exist. If additional written instructions have not been given he is to ensure that the production supervisor has been contacted. This will also be included in the SOP referred to in the previous recommendation.
 for work on equipment in areas where adequate ground control has not been completed or other hazards exist. If additional written instructions have not been given he is to ensure that the production supervisor has been contacted. This will also be included in the SOP referred to in the previous recommendation..")
9
R ECOMMENDATIONS 3. The accident is to be included in the U0028 Scissor Lift training module. Precautions to be taken when repairs and maintenance on equipment in hazardous locations will be reviewed with all new trainees. 4. This accident presented at the Porcupine Northeastern Ontario Mines Safety Group meeting in October, 2014. 5. The Maintenance group will examine the scissor decks to determine what can be done to re-route or protect the hydraulic hoses under the deck from being broken. Re-routing, guarding and sourcing a better quality hose are some of the options.

10
R ECOMMENDATIONS 6. The policy with respect to unsupported ground is being reviewed with each crew and this accident will be reviewed in more detail at the August Safety meetings. At the meetings the crews will be asked what they would have done in the same situation, what lessons were learned and what they will do to prevent a recurrence. 7. The McLean bolter was being utilized in this heading prior to the date of the accident. The McLean was down, so the crew opted to use the x- lift. Review with crews the non-routine hazardous task process (in the event it has to be applied) or additional written instructions from their supervisors on the Zero Harm Safety Cards when conditions in the workplace change (management of change). The deck was fine to use, but when the hose broke, the process "fell apart."
 or additional written instructions from their supervisors on the Zero Harm Safety Cards when conditions in the workplace change (management of change). The deck was fine to use, but when the hose broke, the process fell apart. .")
11
H OW T O P REVENT A R ECURRENCE Review with crews the importance of hazard recognition with respect to face and wall conditions in large development headings. When the things change in the work area (equipment failures, damage etc.) the focus must remained on the hazards and not be focused solely on the task at hand. Review policy with respect to unsupported ground: At no time is a worker to work or go under unsupported ground, caution must also be taken with an unsupported face or wall. The mining culture of “get the job done” by accepting undo risks must be curtailed, employees must never place themselves in a position of risk for the sake of production. The effects of an injury is far reaching, there is pain and suffering of the injured worker, but friends, family and co-workers also feel the pain and effects.
 the focus must remained on the hazards and not be focused solely on the task at hand. Review policy with respect to unsupported ground: At no time is a worker to work or go under unsupported ground, caution must also be taken with an unsupported face or wall. The mining culture of get the job done by accepting undo risks must be curtailed, employees must never place themselves in a position of risk for the sake of production. The effects of an injury is far reaching, there is pain and suffering of the injured worker, but friends, family and co-workers also feel the pain and effects..")
12
Discussion: In a similar situation what would you do, what lessons were learned and what will we do to prevent a recurrence. Discuss as a group.

Similar presentations