Download presentation
Presentation is loading. Please wait.

1
Fahad Alosaimi MD psychiatry and psychosomatic medicine consultant Assistant professor KSU, Riyadh

2
Ahd is a 7 year old boy, was brought by his mother to pediatrician for assessment of his behavior. His teacher noticed that he has problem in staying in his seat & playing in the class a lot. He needs a lot of prompt and direction to follow his teacher. He always answers before the question is completed. At home, his mother complains that he is always hyperactive, forgetful, and his room looks miserable.

3
Analyze the symptoms & signs, both presented and expected in this case including mood, thoughts, cognition, perception and physical aspects. Discuss possible etiological reasons Discuss differential diagnosis Discuss management of attention deficit & hyperactivity disorder.

4
Assessment of the developmental stage is very important to reach the diagnosis. Children are less able to express themselves in words. The child’s existence and emotional development depends on the family or care givers. Evidence of disturbance is based more on observation of behavior made by parents, teachers and others. Psychological problems in a child may be a manifestation of disturbance in other members of the family. Use of psychotropic medications is less common in comparison to adult psychiatry

5
Referral history: medical, school, social, legal Family interview Parent interview Patient interview: verbal, art, play Standardized instruments and psychological tests Physical exam and laboratory studies Informing interview So, assessment interview may last up to 2 hours

6
Biopsychosocial - all elements important Multimodal - individual, family, social, educational, somatic Collaborative Family School others

7
Intellectual developmental disorder (Mental Retardation) Learning disorders Motor skills disorders Communication disorders Pervasive developmental disorders Attention deficit & disruptive disorders Feeding and eating disorders Tic disorders Elimination disorders Other disorders of infancy, childhood & adolescence.
 Learning disorders Motor skills disorders Communication disorders Pervasive developmental disorders Attention deficit & disruptive disorders Feeding and eating disorders Tic disorders Elimination disorders Other disorders of infancy, childhood & adolescence.")
8
Inattention Hyperactivity Impulsivity

9
These criteria are present before age 12 These criteria are present in 2 or more setting Interfere with social, academic or occupational functioning

10
A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2): 1. Inattention: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate). b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading). c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction). d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked). e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines). f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers). g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones). h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts). i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
 of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate). b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading). c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction). d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked). e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines). f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers). g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones). h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts). i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments)..")
11
2. Hyperactivity and impulsivity: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fidgets with or taps hands or feet or squirms in seat. b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place). c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.) d. Often unable to play or engage in leisure activities quietly. e. Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with). f. Often talks excessively. g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation). h. Often has difficulty waiting his or her turn (e.g., while waiting in line). i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing). B. Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years. C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities). D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning. E. The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal).
 of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fidgets with or taps hands or feet or squirms in seat. b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place). c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.) d. Often unable to play or engage in leisure activities quietly. e. Is often on the go, acting as if driven by a motor (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with). f. Often talks excessively. g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation). h. Often has difficulty waiting his or her turn (e.g., while waiting in line). i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing). B. Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years. C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities). D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning. E. The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal)..")
13
CNS Pathophysiology Neurotransmitter dysfunction Dopamine: D4 receptor, dopamine transporter gene mutation implicated norepinephrine, others? These positron emission tomography (PET) scans show that patients with ADHD had lower levels of dopamine transporters in the nucleus accumbens, a part of the brain's reward center, than control subjects.
 scans show that patients with ADHD had lower levels of dopamine transporters in the nucleus accumbens, a part of the brain s reward center, than control subjects..")
14
ODD : oppositional defiant disorder

15
Depressive disorders Bipolar disorders Drug abuse Learning disabilities Language disorders Visual and hearing deficits Anxiety disorders, including OCD and PTSD Environmental stressors Hyperthyroidism Other endocrinopathies Toxic encephalopathy (including drugs, such as theophylline and phenobarbital) CNS trauma, neoplasm, etc.
 CNS trauma, neoplasm, etc.")
16
1. Establish diagnosis 2. Psycho-education to family 3. Psycho-education to school teacher 4. Behavior modification 5. Drug treatment: Stimulants (first line): Methylphenidate, amphetamine/dextroamphetamine Atomoxetine
: Methylphenidate, amphetamine/dextroamphetamine Atomoxetine.")
17
In family history, His 7 year old sister never speaks a sentence except one word. She does not maintain eye contact with them and never relate to them. She seems not listening if they call her name. When she sits, she always moves back and forth. She likes to play with one toy only and gets irritated if lost or moved from her. Moreover, her mother reported that she had delayed milestone. She is not able to be dry day time till now. When her needs are not met, she screams and cries till she get what she wants. She cannot serve herself in feeding and needs assistant in dressing.

18
Analyze the symptoms & signs, both presented and expected in this case including mood, thoughts, cognition, perception and physical aspects. Discuss possible etiological reasons Discuss differential diagnosis Discuss management of Autism spectrum disorder & intellectual disability disorder (mental retardation).
..")
19
Qualitative impairment in social interaction. Qualitative impairments in communication. Restricted repetitive and stereotyped patterns of behavior, interests and activities.

20
A. Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history : 1. Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions. 2. Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures: to a total lack of facial expressions and nonverbal communication. 3. Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers. B. Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history: 1. Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases). 2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
. 2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day)..")
21
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g.,strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests). 4. Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement). C. Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life). D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning. E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co- occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
. 4. Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement). C. Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life). D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning. E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co- occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level..")
24
Establish diagnosis Assess hearing Specific treatment is unknown. Treat inattention Sometimes antipsychotic drugs and antidepressants are used to cope with aggressive behavior and depression. Behavior modification Special education

25
Subaverage intellectual function (IQ<70) Impaired adaptive functioning Childhood onset Subtypes by level Mild: IQ 50 – 70 Moderate: IQ 35 – 50 Severe: IQ 20 – 35 Profound: IQ < 20
 Impaired adaptive functioning Childhood onset Subtypes by level Mild: IQ 50 – 70 Moderate: IQ 35 – 50 Severe: IQ 20 – 35 Profound: IQ < 20")
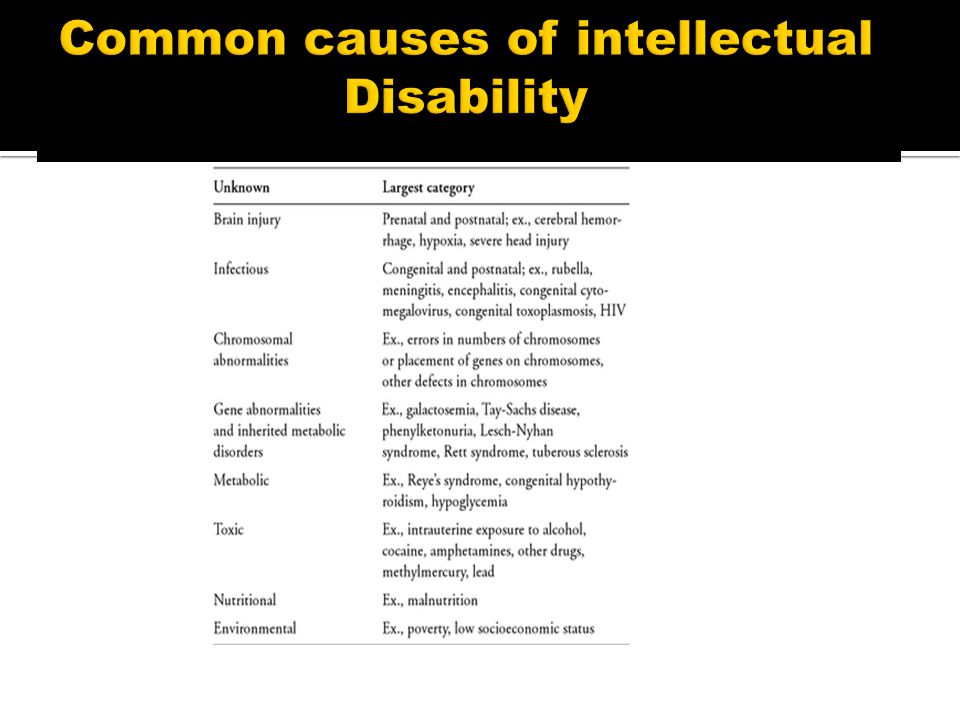
26
A disorder with onset during the developmental period that includes both intellectual and adaptive functioning deficits in conceptual, social, and practical domains. The following three criteria must be met: A. Deficits in intellectual functions, such as reasoning, problem solving, planning, abstract thinking, judgment, academic learning, and learning from experience, confirmed by both clinical assessment and individualized, standardized intelligence testing. B. Deficits in adaptive functioning that result in failure to meet developmental and sociocultural standards for personal independence and social responsibility. Without ongoing support, the adaptive deficits limit functioning in one or more activities of daily life, such as communication, social participation, and independent living, across multiple environments, such as home, school, work, and community. C. Onset of intellectual and adaptive deficits during the developmental period.

28
1. Look for treatable causes 2. Stop further deterioration 3. Special education 4. Behavior modification if needed 5. Drug treatment if needed 6. Help family

29
http://www.safeshare.tv/v/0Az-twgqb_4

Similar presentations










>")

 By: Bianca Jimenez Period:5.>")
. Diagnostic and.>")







 Three.>")
