Download presentation
Presentation is loading. Please wait.

1
Internal Medicine Board Review Cardiology
Mike McMullan, M.D., FACC July 17, 2014

2
Internal Medicine Examination
Cardiology is the largest section of the review Why is this? Cardiology is the largest section of the boards 40% more than the next closest topic 14% of exam, pulmonary is next at 10% Cardiovascular disease affects more people than any other disease process Almost half of your family, friends, neighbors, and patients will eventually die from heart disease

3
Cardiology Topic Breakdown

4
Cardiology Topic Breakdown

5
My Assignment To cover these areas In order to answer
Physical examination Valvular disease Congenital heart disease Pericardial disease Endocarditis/SBE prophylaxis In order to answer 0 questions 2-5 questions 0-1 questions 1-4 questions _____________ 3-11 questions But “the truth of the matter” is that physical examination will encompass all 32 questions!

6
Breaking It Down – My Method
Focused board oriented pearls of frequently-tested disease processes (This is NOT a comprehensive discussion of each topic!) Broken down by general topics Highlight common scenarios within each topic Symptoms Physical findings Diagnostic tests Management Common word associations
 Broken down by general topics. Highlight common scenarios within each topic. Symptoms. Physical findings. Diagnostic tests. Management. Common word associations.")
7
Breaking It Down Physical examination
Knowing the basics will help you figure out questions Will often ask for the diagnostic test (echo) rather than the diagnosis (aortic stenosis) Be aware of normal findings that require no further w/u – e.g. innocent flow murmurs, venous hum Recognize cardiac clues to systemic diseases – e.g. rapid atrial fibrillation with a scratchy murmur hyperthyroidism Means–Lerman scratch
 rather than the diagnosis (aortic stenosis) Be aware of normal findings that require no further w/u – e.g. innocent flow murmurs, venous hum. Recognize cardiac clues to systemic diseases – e.g. rapid atrial fibrillation with a scratchy murmur. hyperthyroidism. Means–Lerman scratch.")
8
The Basics

9
Where does S1 occur? a b c d e f S1

10
Where does S2 occur? S2 a b c d e f

11
Where does S4 occur? a b c d e f S4

12
The Basics 4 heart sounds S1 – closure of mitral/tricuspid valves
S2 – closure of aortic/pulmonic valves S3 – rapid ventricular filling with rapid flow deceleration May be normal in pts < 40 y/o Often seen in CMP and ventricular failure S4 – atrial contraction against a stiff ventricle HTN HCM Aortic stenosis

13
Which of these sounds is lost in a patient with atrial fibrillation?

14
The Basics 3 additional heart sounds Click (occur with valve closure)
Usually MVP Rarely tricuspid click in Ebstein’s anomaly Opening snap (occur with valve opening) Usually right after S2 - mitral stenosis Can occur at beginning of systole – congenital aortic stenosis – and is more often called ejection sound Rub (occur with cardiac motion) Up to 3 components Atrial systole Ventricular systole Ventricular diastole 2 of 3 components are in diastole
 Usually right after S2 - mitral stenosis. Can occur at beginning of systole – congenital aortic stenosis – and is more often called ejection sound. Rub (occur with cardiac motion) Up to 3 components. Atrial systole. Ventricular systole. Ventricular diastole. 2 of 3 components are in diastole.")
15
The Basics 3 types of mumurs Systolic Diastolic Continuous
Systolic ejection=mid-systolic=crescendo-decrescendo Pansystolic=holosystolic Late systolic – associated with click = MVP! Diastolic Early high-pitched decrescendo Aortic or pulmonic regurgitation Low pitched rumble throughout diastole Mitral or tricuspid stenosis Continuous Patent ductus arteriosus AP window Shunt or fistula

16
Basic Murmurs S1 S2 S1 S2 ES OS S4 S1 S3

17
Venous Waveforms in a Nutshell

18
Venous Waveforms in a Nutshell
Ventricular systole Ventricular systole

19
Large “v” Waves

20
What’s the diagnosis? Aortic stenosis Aortic regurgitation
Mitral regurgitation Tricuspid regurgitation

21
What’s the diagnosis? Aortic stenosis Aortic regurgitation
Mitral regurgitation Tricuspid regurgitation

22
What’s the diagnosis? Mitral regurgitation Mitral stenosis
Aortic regurgitation Aortic stenosis 40 30 mmHg LV 20 x y LA 10

23
What’s the diagnosis? Aortic stenosis HCM with obstruction MVP
Brockenbrough sign Aortic stenosis HCM with obstruction MVP Aortic regurgitation Pulsus bisferiens

25
Normal Findings Innocent murmurs Venous hums
Grade 1-2 (mid)systolic ejection murmurs NEVER Grade 3 or more Pansystolic Diastolic Continuous Other abnormal sounds – e.g. fixed split S2 Venous hums High flow states – e.g. anemia Goes away when lays down
systolic ejection murmurs. NEVER. Grade 3 or more. Pansystolic. Diastolic. Continuous. Other abnormal sounds – e.g. fixed split S2. Venous hums. High flow states – e.g. anemia. Goes away when lays down.")
26
Breaking It Down Pericardial disease (1-4 questions) Cardiac tamponade
Constrictive pericarditis Acute pericarditis

27
Cardiac Tamponade Scenarios – trauma and breast cancer are the two biggies on boards, also lupus and renal failure, occasionally viral pericarditis (rarely aortic dissection) Diagnosis – Beck’s triad (hypotension and elevated neck veins with quiet precordium), pulsus paradoxus, electrical alternans Tests - Swan hemodynamics with equalization of all diastolic pressures and slow y descent, echo Mgt – pericardiocentesis
 Diagnosis – Beck’s triad (hypotension and elevated neck veins with quiet precordium), pulsus paradoxus, electrical alternans. Tests - Swan hemodynamics with equalization of all diastolic pressures and slow y descent, echo. Mgt – pericardiocentesis.")
29
RA Pressure in Tamponade

31
Constrictive Pericarditis
Scenarios – post-radiation for lymphoma, CTD, TB Diagnosis – dyspnea, elevated JVP, Kussmaul’s sign, edema, pericardial knock Tests – echo, CT or MRI, cath with prominent x and y descents, equalization of diastolic pressures with square root sign Mgt – pericardial stripping

32
Constrictive Pericarditis
Kussmaul’s sign

34
125 LA Equalization of Diastolic Pressures 25 50 75 100 RA RV LV Constrictive Pericarditis X Y Y>X Square-root sign RVEDP > 1/3 RVSP

35
Acute Pericarditis Scenarios – usually post-viral syndrome
Diagnosis – pleuritic chest pain, feels better sitting up and leaning forward, pericardial friction rub Tests – EKG with diffuse ST elevation, elevated ESR, CRP and/or biomarkers Mgt – NSAIDs Ibuprofen mg TID or ASA mg TID or Indomethacin 50 mg TID for 7-10 days Colchicine 0.5 – 0.6 mg BID Refractory – prednisone plus colchicine

38
Breaking It Down Congenital heart disease (0-1 questions)
ASD – recognize the EKG VSD – almost always no treatment necessary in adults PDA – continuous murmur Coarctation of aorta – secondary HTN, differential BP’s If cyanotic pt (unlikely), probably Tetralogy of Fallot Pregnancy – tolerated in all patients except pulmonary HTN and cardiomyopathies
, probably Tetralogy of Fallot. Pregnancy – tolerated in all patients except pulmonary HTN and cardiomyopathies.")
39
Atrial Septal Defect 4 types but only need to know ostium secundum for boards Scenario – young adult with murmur or palpitations Diagnosis – fixed split S2, 2/6 SEM at LUSB Tests – EKG with incomplete RBBB and RAD, echo, cath with shunt run Mgt – closure (percutaneously or surgically) for shunt > 1.5:1 No SBE prophylaxis recommended – low risk
 for shunt > 1.5:1. No SBE prophylaxis recommended – low risk.")
40
Atrial Septal Defect

41
ASD EKG

42
ASD TEE

43
ASD Occluder

44
VSD Scenario – asymptomatic young adult referred for murmur
Diagnosis – loud grade 5/6 pansystolic murmur at LSB Test – echo Mgt – closure not typically needed for adults, no longer need SBE prophylaxis by guidelines

45
Ventricular Septal Defect

46
Ventricular Septal Defect

47
Ventricular Septal Defect

48
PDA Scenario – teen or young adult referred for murmur
Diagnosis – usually asymptomatic, continuous murmur LSB Tests – echo Mgt – closure if murmur noted or left ventricular enlargement or pulmonary HTN, small ones without murmur do not need to be closed, no longer need SBE prophylaxis

49
Patent Ductus Arteriosus

50
Patent Ductus Arteriosus

51
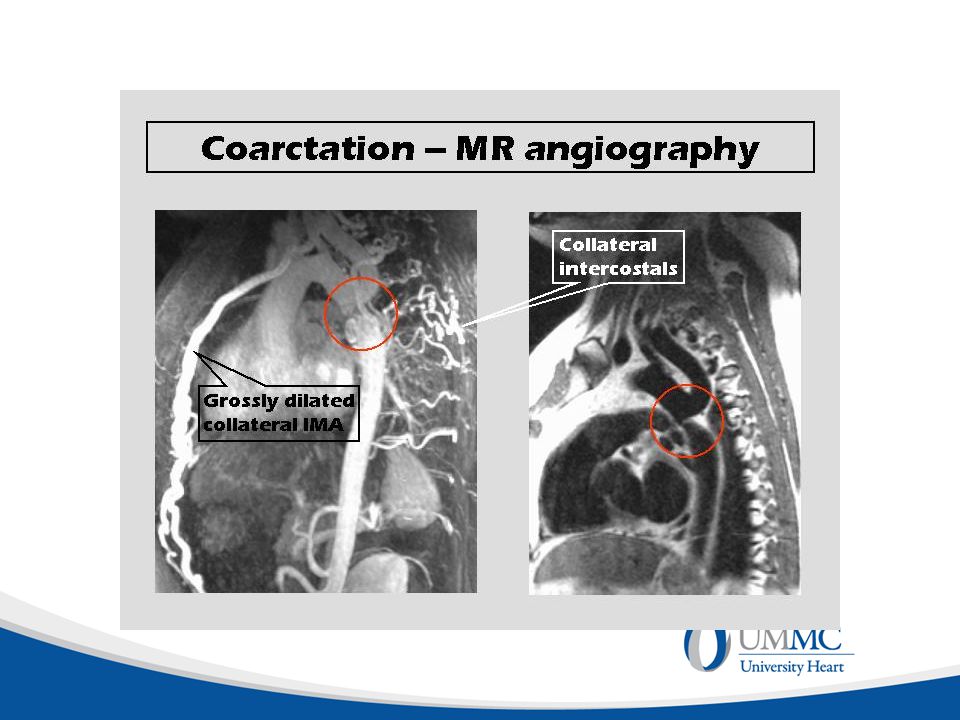
Coarctation of Aorta Great IM board question since it is a secondary cause of HTN Scenario – young adult with HTN, association with Turner’s syndrome Diagnosis – BP in arms vs legs, radiofemoral pulse delay, 2/6 SEM LSB, may have aortic ejection click with bicuspid aortic valve Tests – CXR with figure 3 sign and rib notching, echo, CT angio or MRA Mgt – surgical repair, less commonly stent

52
Coarctation of Aorta

53
Coarctation CXR

55
Cyanotic Lesions Not likely for an IM board
Tetralogy most common – young person with cyanosis and squatting Eisenmenger’s (secondary pulm HTN with conversion to right-to-left shunt) most commonly occurs with VSD Ebstein’s may present as cyanosis in adult, usually with palpitations due to right-sided accessory pathway, marked RAE on EKG and echo
 most commonly occurs with VSD. Ebstein’s may present as cyanosis in adult, usually with palpitations due to right-sided accessory pathway, marked RAE on EKG and echo.")
56
Tetralogy of Fallot

57
Pregnancy and Heart Disease
Lots of pregnant women on the boards – not many with heart disease Cardiac lesions affecting pregnancy Pulmonary HTN Cyanotic lesions (uncorrected) Stenotic valve lesions CMP Recommend vaginal delivery with facilitated second stage Peripartum CMP may occur last 3 months of pregnancy or first 6 months after delivery Marfan’s and coarctation are at higher risk for aortic rupture during surgery
 Stenotic valve lesions. CMP. Recommend vaginal delivery with facilitated second stage. Peripartum CMP may occur last 3 months of pregnancy or first 6 months after delivery. Marfan’s and coarctation are at higher risk for aortic rupture during surgery.")
58
Pregnancy and Heart Disease
High risk Eisenmenger’s syndrome Severe pulmonary HTN Severe aortic stenosis/LVOT obstruction Coarctation of the aorta with obstruction Marfan’s syndrome with aortic root > 43 mm Symptomatic systemic ventricular dysfunction with EF < 40% Need referral to high risk OB center with cardiology collaboration Lower risk lesions can typically have normal pregnancy and delivery CARPREG score Poor functional status (NYHA >2) or cyanosis Systemic ventricular dysfunction Left heart obstruction History of heart failure, stroke, or arrhythmia
 or cyanosis. Systemic ventricular dysfunction. Left heart obstruction. History of heart failure, stroke, or arrhythmia.")
59
Risk of CHD in Offspring of Parents with CHD
Typically 3-12% Can be up to 50% (Marfan’s syndrome) Fetal ultrasonography weeks
 Fetal ultrasonography weeks.")
60
Breaking It Down Valvular heart disease (2-5 questions)
Aortic stenosis – elderly vs younger Aortic regurgitation – Marfan’s or endocarditis MVP – maneuvers, SBE prophylaxis HCM – sudden death in an athlete, maneuvers Mitral stenosis – rheumatic heart disease Tricuspid stenosis with carcinoid patient Tricuspid regurgitation in a patient with right heart failure

61
Aortic Stenosis Scenarios – young to middle aged adult with bicuspid valve, older adult (> 70 y/o) with tricuspid valve Diagnosis Symptoms are chest pain, syncope, CHF PE shows 3-4/6 SEM at RUSB radiating to carotids, pulsus parvus et tardus (weak and delayed upstrokes) Tests – echo, cath only as pre-op for CAD Mgt – surgery, balloon valvuloplasty is only palliative and short-lived, TAVR new option – only for inoperable or extreme high risk at present – probably too early for boards right now
 Tests – echo, cath only as pre-op for CAD. Mgt – surgery, balloon valvuloplasty is only palliative and short-lived, TAVR new option – only for inoperable or extreme high risk at present – probably too early for boards right now.")
62
Aortic Regurgitation Scenario – Marfan’s syndrome, endocarditis
Diagnosis – shortness of breath, early high-pitched decrescendo diastolic murmur at left or right upper sternal border, wide pulse pressure, brisk pulses Test – echo Mgt – afterload reduction with ACE inhibitor or nifedipine, valve replacement for EF < 55% or LVESD > 55mm

63
MVP Favorite board question
Scenario – young woman with palpitations, chest pain Diagnosis – mid-systolic click with late systolic murmur, increases with Valsalva Test – echo Mgt – beta blocker for symptoms, SBE prophylaxis no longer recommended!, valve repair only for severe regurgitation +/- atrial fibrillation or pulmonary HTN

64
MVP

65
Hypertrophic Cardiomyopathy
Favorite board question Scenario – young athlete with syncope or aborted sudden death, SOB, diastolic heart failure Diagnosis – SEM at RUSB which increases with Valsalva, brisk carotid upstrokes, S4, pulsus bisferiens Test – EKG with LVH and T wave inversion, echo Mgt – beta blockers and calcium channel blockers, surgical or percutaneous myectomy, ICD placement if high risk for sudden death, no competitive athletics except golf and bowling, screening of first- and second-degree relatives

66
HCM

68
HCM EKG

69
Differentiating Aortic Stenosis from Hypertrophic Cardiomyopathy
Same Both may present with syncope Both have a harsh SEM radiating to the carotids Different HCM usually younger than AS Carotid upstrokes are brisk with HCM, diminished with AS Murmur gets louder with Valsalva with HCM, softer with Valsalva with AS

70
Mitral Stenosis Yet another favorite board question
Scenario – woman with history of rheumatic heart disease Diagnosis – DOE, palpitations, PND, diastolic rumble with loud S1 and opening snap just after S2, small PMI, palpable P2, rales Tests – echo, TEE to grade valve Mgt – slow heart rate to improve diastolic filling time – beta blockers, SBE prophylaxis no longer required, balloon valvuloplasty is the first line procedure for these pts (as opposed to AS)
")
71
Tricuspid Stenosis Not a likely question
Same murmur as mitral stenosis but at left sternal border rather than apex Present with right heart failure rather than DOE and rales Seen in association with carcinoid and with prior use of Fen-Phen

72
Tricuspid Regurgitation
Not a likely test question, but may see a case of pulm HTN with TR and also PR Scenario – young woman with severe SOB, hypoxia, and right heart failure – edema, ascites, elevated JVP, large v wave, pulsatile liver Diagnosis – echo, right heart cath, CTA – must rule out other etiologies – CTD, congenital heart disease, recurrent PE Mgt – pulm HTN has poor prognosis if no reversible cause, O2, calcium blockers, Coumadin, prostacyclin analogs (epoprostenol), endothelin receptor antagonists (bosentan), phosphodiesterase-5 inhibitors (sildenafil), lung transplantation
, endothelin receptor antagonists (bosentan), phosphodiesterase-5 inhibitors (sildenafil), lung transplantation.")
73
Endocarditis Guidelines – Updated 2008
No Class I indications for endocarditis prophylaxis Class IIA recommendations Antibiotic prophylaxis is reasonable for dental procedures for patients with – Prosthetic cardiac valve or material used in valve repair Previous endocarditis Congenital heart disease Unrepaired cyanotic disease, including palliative shunts/conduits Completely repaired CHD for the first six months after correction Repaired CHD with residual defects at site of prosthesis Cardiac transplant with valvular heart disease No prophylaxis for GI or GU procedures

74
SBE Prophylaxis Know prophylaxis regimen
Amoxicillin 2.0 g orally 1 hour before procedure Know what to use in a PCN allergic patient! Clindamycin 600 mg orally 1 hour before procedure Keflex 2.0 g orally 1 hour before procedure Zithromax 500 mg orally 1 hour before procedure

75
Endocarditis Scenario – think about it in a pt with multisystem involvement, fever, chills, skin lesions, recent dental work or surgery, murmur – also with an IV drug user with multiple lung lesions Diagnosis – clinical picture, fever, regurgitant murmur, splenomegaly, Janeway lesions, Osler’s nodes, Roth’s spots, anemia, leukocytosis, elevated ESR and CRP, glomerulonephritis Tests – blood cultures are mainstay of diagnosis, echo/TEE Mgt – IV antibiotics Empiric therapy – Vancomycin after 2-3 sets of blood cultures drawn Guide further therapy based on organism/sensitivities PCN G or Rocephin for 4 weeks PCN G + Gentamicin for 2 weeks Common organism – Viridans group streptococci Unusual organism associations Strep gallolyticus (formerly Strep bovis) Associated with colon cancer Needs colonscopy
 Associated with colon cancer. Needs colonscopy.")
80
The Bottom Line Recognize word associations Irregularly irregular
Mid-systolic click Pulsus paradoxus Pulsus alternans Electrical alternans Pulsus parvus et tardus Kussmaul’s sign Large v waves Prominent x and y descents Fixed splitting of S2 Paradoxical splitting of S2 Wide physiologic splitting of S2

81
The Bottom Line Recognize word associations Pericardial knock
Pericardial rub Continuous murmur Pansystolic murmur Early high pitched diastolic murmur Low pitched diastolic rumble Elevated neck veins with clear lung fields Elevated neck veins with hypotension and quiet precordium Murmur increases with Valsalva

82
80 year old woman presents with syncope, on exam has weak carotid upstrokes, a normal S1 with a diminished S2, and a grade III/VI systolic ejection murmur at the RUSB radiating to the carotids. Bicuspid aortic valve stenosis Tricuspid aortic valve stenosis Hypertrophic cardiomyopathy VSD

83
40 year old man with Marfan’s syndrome, a blood pressure of 150/50, brisk pulses throughout, and an early high-pitched diastolic murmur heard best at the RUSB Hypertrophic cardiomyopathy Mitral stenosis Aortic regurgitation Pulmonic regurgitation

84
30 year old woman who presents with palpitations, on exam has a normal S1 and S2, a midsystolic click, and a late systolic murmur that occurs earlier (becomes longer and/or louder) with Valsalva maneuver VSD Hypertrophic cardiomyopathy Mitral regurgitation Mitral valve prolapse

85
Bicuspid aortic stenosis Tricuspid aortic stenosis
20 year old basketball player referred for episode of syncope, noted to have brisk carotid upstrokes, a normal S1 and S2 with an S4 gallop, and a grade II/VI systolic ejection murmur at the LSB which becomes louder with Valsalva maneuver Bicuspid aortic stenosis Tricuspid aortic stenosis Hypertrophic cardiomyopathy Mitral valve prolapse

86
Maneuvers Valsalva and standing decrease ALL murmurs except –
Hypertrophic cardiomyopathy Mitral valve prolapse Therefore – Valsalva and standing increase the murmur of HCM and MVP Squatting reduces the murmur of HCM and MVP

87
Mitral stenosis Aortic regurgitation VSD PDA
35 year old woman with increasing dyspnea and fatigue, a history of rheumatic heart disease, a loud S1, a prominent S2 followed by an opening snap, and a diastolic rumble which becomes louder at the end of diastole Mitral stenosis Aortic regurgitation VSD PDA

88
Pulmonary stenosis VSD ASD Aortic stenosis
35 year old woman referred for palpitations and murmur, normal S1 with wide fixed splitting of S2, and a grade II/VI systolic ejection murmur at the LUSB Pulmonary stenosis VSD ASD Aortic stenosis

89
Left bundle branch block Right bundle branch block Aortic stenosis HTN
65 year old man who is asymptomatic, noted to have a normal S1, a second heart sound of normal intensity which splits with expiration and becomes single with inspiration (paradoxical splitting), and no murmur Left bundle branch block Right bundle branch block Aortic stenosis HTN This was on the 1994 IM board exam!
, and no murmur. Left bundle branch block. Right bundle branch block. Aortic stenosis. HTN. This was on the 1994 IM board exam!")
90
Best of luck! Get a good night’s sleep! Trust your initial reaction.
Use clinical judgment. Look for the point of the question. If no clue, guess and move on. Can always come back if time allows.

91
And remember…

92
Bonus questions! me with your answers. Or if you have questions or suggestions.
93
25 year old man who presents to the ER following a stab wound to the left chest, found to have a BP of 80/50, HR 130, a pulsus paradoxus of 20 mm Hg, distended neck veins, and distant heart sounds Constrictive pericarditis Cardiac tamponade Restrictive cardiomyopathy Tension pneumothorax

94
28 year old woman with primary pulmonary hypertension, elevated neck veins with a prominent v wave, a II/VI pansystolic murmur at the LLSB that increases with inspiration, and a pulsatile liver Mitral regurgitation Tricuspid regurgitation VSD ASD

95
45 year old veteran who presents with palpitations and SOB after a week-end of binge drinking, on exam has a radial pulse of 120, an apical pulse of 180, and an irregularly irregular heart rhythm PAC’s Bigeminy Atrial flutter Atrial fibrillation

96
25 year old woman with a history of recent onset hypertension, diminished femoral pulses, and a grade II/VI systolic ejection murmur at the LSB and back Subclavian stenosis Peripheral vascular disease Coarctation of the aorta Renal artery stenosis

97
70 year old man from a nursing home with elevated neck veins that increase with inspiration and prominent x and y descents, normal S1 and S2 with a loud S3 knock, and no murmur Constrictive pericarditis Restrictive cardiomyopathy Cardiac tamponade Tricuspid regurgitation

98
35 year old woman referred for murmur, has a continuous murmur at the 2nd left intercostal space
Tetralogy of Fallot Pulmonary stenosis Patent ductus arteriosus Coarctation of the aorta

99
35 year old woman with a history of a murmur since birth, has a grade IV/VI pansystolic murmur at the left sternal border Tetralogy of Fallot ASD VSD Transposition of the great arteries

100
5 year old boy with a history of cyanosis and digital clubbing, noted to stop and “squat” during play, has an RV lift, a single S2, and a grade III/VI systolic ejection murmur at the LUSB Tetralogy of Fallot VSD Pulmonic stenosis ASD Transposition of the great arteries

101
Venous hum! Lay her back down and it will go away.
You are performing routine physical exams for your local high school athletes. You notice a continuous murmur over the neck in a healthy-appearing 18 y/o girl while she is sitting on the stretcher. What is the most likely diagnosis and how do you confirm it? Venous hum! Lay her back down and it will go away.

102
The next patient has a 2/6 midsystolic murmur at the LUSB with physiologic splitting of S2. What is the most likely diagnosis? Innocent murmur - always < 2/6 murmur - never diastolic - never pansystolic - normal S2

103
Myocardial infarction Pulmonary embolus Pericarditis Pneumothorax
A 30 y/o man presents with chest pain which is less severe when he sits up and leans forward. On exam, he has a scratchy sound in systole and diastole heard throughout his precordium. This is his EKG. Most likely diagnosis is - Myocardial infarction Pulmonary embolus Pericarditis Pneumothorax

104
Bonus questions - answers
B, B, D, C, A, C, C, A Venous hum, innocent murmur C Remember, me for questions!

Similar presentations






















 Chapter 8 Are G. Talking, MD, FACC Instructor Patricia L. Thomas, MBA, RCIS.>")







