Download presentation
Presentation is loading. Please wait.

2
Objective Comparison of direct real-time endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration (TBNA), PET, CT for detection of mediastinal and hilar lymph node metastasis in patients with lung cancer considered for surgical resection
-guided transbronchial needle aspiration (TBNA), PET, CT for detection of mediastinal and hilar lymph node metastasis in patients with lung cancer considered for surgical resection")
3
Methods Design: Prospective study ( December 2003 to March 2005 ) Patients: 102 /280 potentially operable patients with proven ( 96) or radiologically suspected ( 6) lung cancer Interventions: CT, PET, and EBUS-TBNA Surgical histology :The “gold standard” to confirm lymph node metastasis ( expect N3 or extensive N2 disease proven by EBUS-TBNA
 Patients: 102 /280 potentially operable patients with proven ( 96) or radiologically suspected ( 6) lung cancer Interventions: CT, PET, and EBUS-TBNA Surgical histology :The gold standard to confirm lymph node metastasis ( expect N3 or extensive N2 disease proven by EBUS-TBNA")
4
Methods CT MDCT ; 5mm Resectability; Evaluation of LN or distant metastases Radiologist ( blinded ) Positive node: Positive node: short axis 1 cmFDG-PET/CT 300 MBq Positive: SUV > 2.5
 Positive node: Positive node: short axis 1 cmFDG-PET/CT 300 MBq Positive: SUV > 2.5")
5
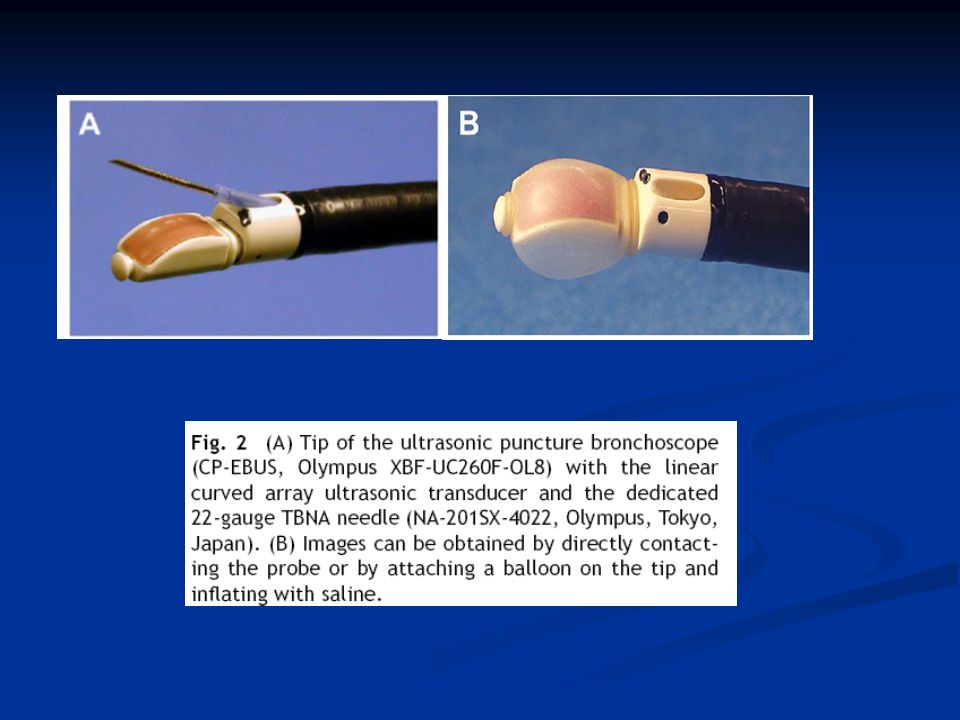
Methods EBUS-TBNA Linear scanning transducer (7.5 MHz) Connection with ultrasound scanner ( Doppler – flower imaging) Performed by the same operator under sedation #1,2,4,7 & #10,11 Short diameter >5mm sampling ( 22-qauge) N3->N2->N1 Result : positive, negative, inconclusive
 Connection with ultrasound scanner ( Doppler – flower imaging) Performed by the same operator under sedation #1,2,4,7 & #10,11 Short diameter >5mm sampling ( 22-qauge) N3->N2->N1 Result : positive, negative, inconclusive")
8
Methods Operable Stage I, II or minimal Stage IIIA (single-station N2 ) Inoperable Extrathoracic spread disease Extensive N2 ( bulky disease, multiple N2 ) N3 disease
 Inoperable Extrathoracic spread disease Extensive N2 ( bulky disease, multiple N2 ) N3 disease")
9
Results

10
Results

12
Discussion FDG-CT More sensitive, less specificity( 61%vs 79% ; 85% vs 90%) More sensitive, less specificity( 61%vs 79% ; 85% vs 90%) Specificity is lower than previously reported Specificity is lower than previously reported Mediastinal nodes, distal metastasis, inflammatory reaction Mediastinal nodes, distal metastasis, inflammatory reaction False positive tissue conformation False positive tissue conformation 23 false positive correctly diagnosis by EBUS-TBNA 23 false positive correctly diagnosis by EBUS-TBNA False positive : related to size of node and volume of macrophage False positive : related to size of node and volume of macrophage 16/23 : CT(+); PET(+) 16/23 : CT(+); PET(+)
 More sensitive, less specificity( 61%vs 79% ; 85% vs 90%) Specificity is lower than previously reported Specificity is lower than previously reported Mediastinal nodes, distal metastasis, inflammatory reaction Mediastinal nodes, distal metastasis, inflammatory reaction False positive tissue conformation False positive tissue conformation 23 false positive correctly diagnosis by EBUS-TBNA 23 false positive correctly diagnosis by EBUS-TBNA False positive : related to size of node and volume of macrophage False positive : related to size of node and volume of macrophage 16/23 : CT(+); PET(+) 16/23 : CT(+); PET(+)")
13
Discussion EBUS-TBNA High sensitive & specific High sensitive & specific A single procedure for staging A single procedure for staging 40/147 mediastinal nodes <5 mm 40/147 mediastinal nodes <5 mm Avoid mediastinoscopy and VATS Avoid mediastinoscopy and VATS False positive: contamination in TBNA process False positive: contamination in TBNA process internal sheath : avoid contamination internal sheath : avoid contamination Limitation : no compare other procedures ( TBNA, EUS-FNA) Limitation : no compare other procedures ( TBNA, EUS-FNA) : # 5,6,8,9 : # 5,6,8,9
 Limitation : no compare other procedures ( TBNA, EUS-FNA) : # 5,6,8,9 : # 5,6,8,9")
14
Discussion TBNA is a fairly “ blind ” procedure TBNA guided by CT fluoroscopy EUS-FNA US-guided needle aspiration

16
Conclusion EBUS-TBNA has a high sensitivity & pecificity compared to CT or PET for mediastinal staging in patients with potentially resectable lung cancer Tissue confirmation obtained by EBUS-TBNA is especially important for accurate staging.

Similar presentations




>")









 Fredric Hoffer, MD Suddhasatta Acharyya,>")


 in Colorectal Cancer Dr Chan Wai Keung Department of Surgery Ruttonjee and Tang Shiu Kin Hospitals.>")





