Download presentation
Presentation is loading. Please wait.

1
Medical School of Oncology Highlights on NSCLC Management STAGING STRATEGIES Maria Grazia Ghi Divisione di Oncologia-Venezia Roma, 29 ottobre 2010

2
Il nuovo sistema di stadiazione TNM definisce il nodulo polmonare in altro lobo ipsi-laterale come: 1.T3 2.T4 3.M1 1 / 30 Cross-tab label

3
Qual è la metodica di stadiazione in uso nel vostro Centro per la stadiazione del mediastino con sospetto N2? 1.TAC + PET 2.Imaging (TAC +/- PET) + TBNA 3.Imaging (TAC +/- PET) + EBUS/EUS 4.Imaging (TAC +/- PET) + mediastinoscopia 1 / 30 Cross-tab label
 + TBNA 3.Imaging (TAC +/- PET) + EBUS/EUS 4.Imaging (TAC +/- PET) + mediastinoscopia 1 / 30 Cross-tab label.")
4
TNM STAGING SISTEM 6 TH EDITION - Different stages of disease based on anatomic extention and survival data - Monoinstitutional database (USA) - 5,319 patients from historical cases (pre- 1975) - Adopted from 1997 to December 2009 - No internal or external validation
 - 5,319 patients from historical cases (pre- 1975) - Adopted from 1997 to December No internal or external validation")
5
TNM STAGING SISTEM 7 TH EDITION - Different stages of disease based on anatomic extention and survival data - International database from 4 continents (North America, EU, Asia, Australia) - More than 67.000 patients of cases treated 1990-2000 - Adopted from January 2010 - Internal and external validation with recognized statistical methods
 - More than patients of cases treated Adopted from January Internal and external validation with recognized statistical methods")
6
THE NEW STAGING SISTEM The importance of staging - Prognostic information - Therapeutic decision : surgery +/- induction therapy chemoradiation chemotherapy

7
c TNM stage : MST & 5y OS

8
THE NEW STAGING SISTEM Changes for T definition

9
THE NEW STAGING SISTEM Changes for T definition - To subclassify T1 and T2 according to tumor size - To identify a new T3 definition according to tumor size - To reclassify additional node in the same lobe and in different ipsilateral lobe - To reclassify malignant pleural effusion

10
THE NEW STAGING SISTEM Changes for T definition according to dimensional criteria

11
THE NEW STAGING SISTEM Changes for T definition (T1-3) according to dimensional criteria OS for clinical T stage N0
 according to dimensional criteria OS for clinical T stage N0")
12
THE NEW STAGING SISTEM Changes for T definition (T1-3) according to dimensional criteria
 according to dimensional criteria")
13
THE NEW STAGING SISTEM Changes for T definition according to other parameters Reclassify T4 tumours due to additional tumour nodeles in the primary lobe as T3 Reclassify M1 tumours due to additional tumour nodeles in other ipsilateral lobe as T4 Reclassify T4 tumours due to malignant pleural effusion as M1, create M1a category

14
THE NEW STAGING SISTEM Changes for T definition (T3-4) according to other parameters OS for clinical T stage N0 - multiple nodes in the same lobe is stage II - multiple nodes in different lobe on the same side is stage III
 according to other parameters OS for clinical T stage N0 - multiple nodes in the same lobe is stage II - multiple nodes in different lobe on the same side is stage III")
15
THE NEW STAGING SISTEM Changes for T definition (T3-4) according to other parameters
 according to other parameters")
16
THE NEW STAGING SISTEM Methods for T stage definition - modern spiral contrast CT scan (mediastinal or lung windows) Good quality multi-slice CT is the minimum standard
 Good quality multi-slice CT is the minimum standard")
17
THE NEW STAGING SISTEM Difficulties for T stage definition - visceral pleural invasion (T2) - mediastinal pleural invasion (T3) - parietal pericardial invasion (T3) - hilar fat invasion (T2) - mediastinal fat invasion (T4) - ground glass opacities
 - mediastinal pleural invasion (T3) - parietal pericardial invasion (T3) - hilar fat invasion (T2) - mediastinal fat invasion (T4) - ground glass opacities")
18
THE NEW STAGING SISTEM Changes for M definition

19
THE NEW STAGING SISTEM Changes for M definition - To identifie intrathoracic and extrathoracic metastases (M1a vs M1b) - To reclassify additional node in the controlateral lung (M1a) - To reclassify malignant pleural effusion (M1a)
 - To reclassify additional node in the controlateral lung (M1a) - To reclassify malignant pleural effusion (M1a)")
20
THE NEW STAGING SISTEM Changes for M definition OS for clinical M stage

21
THE NEW STAGING SISTEM Changes for M definition No Mx definition!

22
THE NEW STAGING SISTEM Methods for M stage definition - contrast CT scan (chest and abdominal) - brain MRI/CT scan in symptomatic pts - Bone scan if sympthoms - PET or PET/CT scan
 - brain MRI/CT scan in symptomatic pts - Bone scan if sympthoms - PET or PET/CT scan")
23
THE NEW STAGING SISTEM N definition

24
THE NEW STAGING SISTEM the importance of N definition - Diagnosis of NSCLC is often based on nodes analysis - Adequate tissue sampling need for biological and molecular analysis

25
THE NEW STAGING SISTEM The importance of N definition - Mediastinal lymphnode involvement is the most important prognostic factor in M0 pts - Mediastinal lymphnode involvement influences therapeutic strategies - If complete resection is considered, an accurate mediastinal lymphnode evaluation is mandatory

26
THE NEW STAGING SISTEM Changes for N definition - New defined nodal zone and nodal station map - No changes for N definition

27
THE NEW STAGING SISTEM No changes for N definition

28
THE NEW STAGING SISTEM No changes for N definition OS for c N stage any cT,M0 but..... should it be changed?

29
c N2 Stage T2b N2 M0 – IIIa - Different therapeutic approach ? - Different prognosis?

30
Andre F et al, JCO 2000 Surgery could cure a small proportion of N2 patients Distinguishing mN2 from cN2 must be a goal of preoperative Surgery could cure a small proportion of N2 patients Distinguishing mN2 from cN2 must be a goal of preoperative

31
Minimal N2 (mN2): no preoperative evidence of gross N2 at CT scan Clinical N2 (cN2): evidence of N2 disease at CT scan N2 single station (N2 L1) N2 multiple station (N2L2) LN size Grunenwald d et al, JNCI 1997 Ruckdeshel JC, Semin Oncol 1997 Subclassification of N2 disease (not validated)
: no preoperative evidence of gross N2 at CT scan Clinical N2 (cN2): evidence of N2 disease at CT scan N2 single station (N2 L1) N2 multiple station (N2L2) LN size Grunenwald d et al, JNCI 1997 Ruckdeshel JC, Semin Oncol 1997 Subclassification of N2 disease (not validated)")
32
THE NEW STAGING SISTEM No changes for N definition Unanswered questions - Different prognosis based on the n°of node? Probably yes but too small n° of patients 5y OS: single N1: 48% multiple N1: 35% p<0.09 single N2: 34% multiple N2: 20% p<0.001

33
N3 zone N2 zone Nodal zone and nodal station map solving discrepancies between Western and Japanase map

34
N1 zone N2 zone THE NEW STAGING SISTEM Nodal zone and nodal station map

35
METHODS FOR N STAGE DEFINITION - CT scan - PET or PET/CT scan - mediastinoscopy - thoracoscopy - TTNA - TBNA - EBUS TBNA - EUS FNA Not invasive Minimally invasive Invasive

36
Not invasive methods - CT scan - PET scan - PET-CT MEDIASTINAL LN STAGING

37
CT scan - based on node size - sensitivity 57% - specificity 82% - PPV 56% - NPV 83% - Clinical applicability limited for small nodes (20% may contain metastases) - Large nodes may be benign - Insufficient for clinical decision - Usefull for select procedures for sampling of suspected LNs De Leyn et al, E J CT S 2007 METHODS FOR N STAGE DEFINITION
 - Large nodes may be benign - Insufficient for clinical decision - Usefull for select procedures for sampling of suspected LNs De Leyn et al, E J CT S 2007 METHODS FOR N STAGE DEFINITION")
38
PET scan Functional imaging - Sensitivity 74% - Specificity 85% - PPV 79% - NPV 93% - Insufficient anatomic details - Limitation in spacial resolution - Uptake by inflammatory disease De Leyn et al, E J CT S 2007 METHODS FOR N STAGE DEFINITION

39
PET-CT scan - Dual purpose:. Node size. Biologic activity - Sensitivity 89% - Specificity 84-94% METHODS FOR N STAGE DEFINITION

41
Invasive surgical methods - mediastinoscopy (cervical) - left side videothoracoscopy (VATS) for tumor of the left upper lobe (station 5 and 6) - anterior mediastinotomy (Chamberlain procedures) – higher morbidity than cervical approach METHODS FOR N STAGE DEFINITION
 - left side videothoracoscopy (VATS) for tumor of the left upper lobe (station 5 and 6) - anterior mediastinotomy (Chamberlain procedures) – higher morbidity than cervical approach METHODS FOR N STAGE DEFINITION")
42
Invasive methods METHODS FOR N STAGE DEFINITION

43
Cervical Mediastinoscopy - General anesthesia - LN station 1,2,4, 7 sub. - Sensitivity 78% - Specificity 100% - False negative 10% - False positive 0% - Morbidity 2% - Mortality 0.08% - Poorly utilized (27%) - some stations are not accessible (5,6,8,9,7 posterior) - No consensus on how many LN station should be examined (at least one omolateral, one controlateral and the subcarinal) METHODS FOR N STAGE DEFINITION Detterbeck et al, Chest 2007
 - some stations are not accessible (5,6,8,9,7 posterior) - No consensus on how many LN station should be examined (at least one omolateral, one controlateral and the subcarinal) METHODS FOR N STAGE DEFINITION Detterbeck et al, Chest")
44
Minimally invasive methods - Transbronchial needle aspiration - TBNA (blind) - Trans thoracic needle aspiration - TTNA (CT or fluoroscopic guided) - EBUS TBNA - EUS FNA METHODS FOR N STAGE DEFINITION
 - Trans thoracic needle aspiration - TTNA (CT or fluoroscopic guided) - EBUS TBNA - EUS FNA METHODS FOR N STAGE DEFINITION")
45
EBUS FNA for mediastinal staging - No general anesthesia - Anterior LN station 2,4, 7, 10, 11 - station 3 (post) - Sensitivity 76-93% - Specificity 100% - False positive 0% - False negative 20% METHODS FOR N STAGE DEFINITION
 - Sensitivity 76-93% - Specificity 100% - False positive 0% - False negative 20% METHODS FOR N STAGE DEFINITION")
46
EBUS metanalysis for mediastinal staging 1299 pts from 11 studies (CT or PET pos. in 8 studies) METHODS FOR N STAGE DEFINITION
 METHODS FOR N STAGE DEFINITION.")
47
EUS FNA for mediastinal staging - No general anesthesia - posterior LN station 2,4, 5(AP w),7 - inferior LN station 8,9 - Sensitivity 84% - Specificity 99.5% - False positive 0.7% - False negative 19% METHODS FOR N STAGE DEFINITION Detterbeck et al, Chest 2007
,7 - inferior LN station 8,9 - Sensitivity 84% - Specificity 99.5% - False positive 0.7% - False negative 19% METHODS FOR N STAGE DEFINITION Detterbeck et al, Chest 2007")
48
EUS metanalysis for mediastinal staging 1201 pts from 18 studies METHODS FOR N STAGE DEFINITION Micames et al, Chest 2007

49
EBUS vs EUS - 160 pts with enlarged CT nodes - all pts received EUS and EBUS nodes staging METHODS FOR N STAGE DEFINITION

50
TBNA vs EUS vs EBUS vs EBUS+EUS Wallace et al, JAMA 2008 138 pts regardless of radiographic LN disease METHODS FOR N STAGE DEFINITION

51
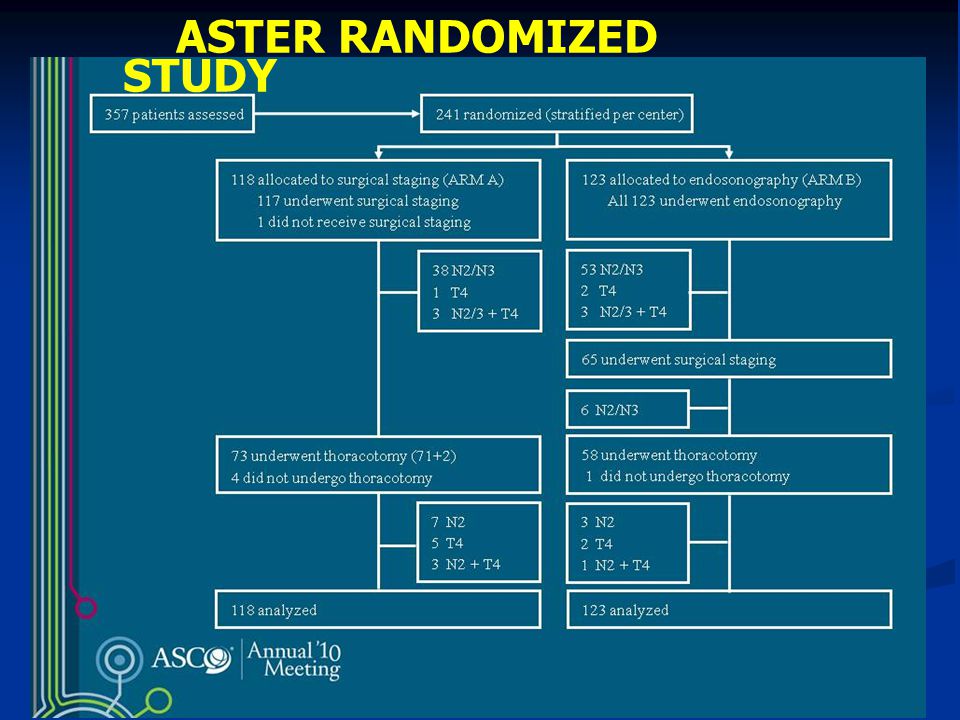
ASTER RANDOMIZED STUDY Endosonography (EBUS + EUS) followed by surgical staging vs surgical staging alone in N2-3 suspect disease Tournoy et al, ASCO 2010
 followed by surgical staging vs surgical staging alone in N2-3 suspect disease Tournoy et al, ASCO 2010")
52
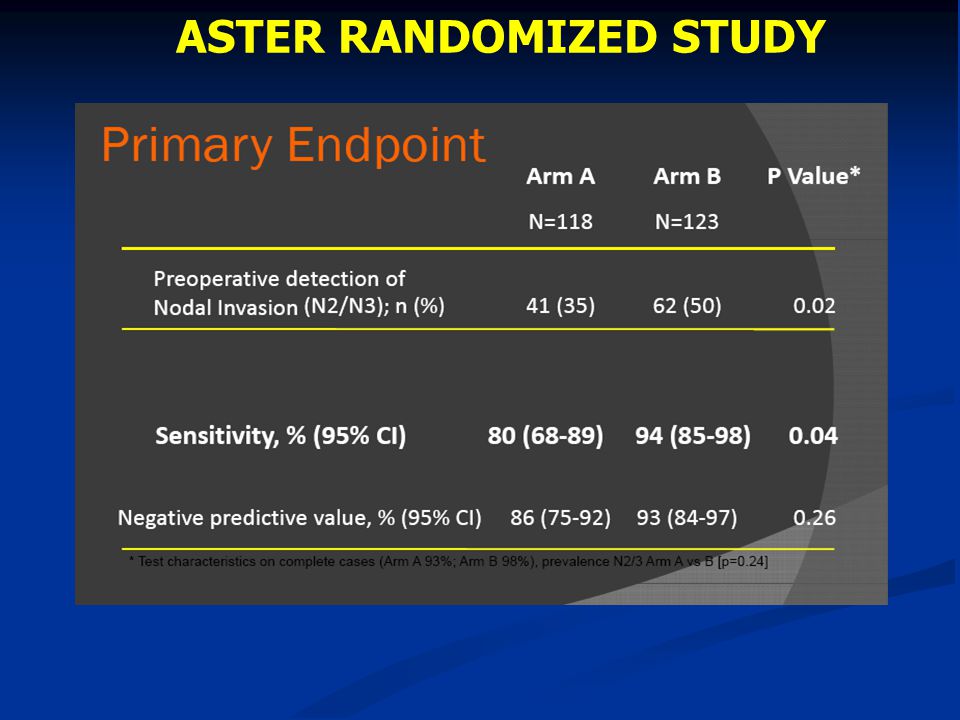
ASTER RANDOMIZED STUDY

58
CONCLUSION OF ASTER STUDY IMPLICATION s: - Initial endosonography should be the new standard for mediastinal staging - Starting mediastinal staging with endosonography in resectable NSCLC: 1) improved the detection of LN metastases 2) reduces futile thoracotomies 3) for a similar complication rate as compared to surgical staging alone
 improved the detection of LN metastases 2) reduces futile thoracotomies 3) for a similar complication rate as compared to surgical staging alone")
59
- High false negative value for blind TBNA (around 30%) and CT scan (around 20%); high false positive for PET (around 20%) - Endoscopy ultrasonography improve the accuracy of TBNA (but expertise dependent) - Endoscopy ultrasonography associated with minimal complications - Minimally invasive techniques (high specificity but low NPV) are complementary to mediastinoscopy METHODS FOR N STAGE DEFINITION
 and CT scan (around 20%); high false positive for PET (around 20%) - Endoscopy ultrasonography improve the accuracy of TBNA (but expertise dependent) - Endoscopy ultrasonography associated with minimal complications - Minimally invasive techniques (high specificity but low NPV) are complementary to mediastinoscopy METHODS FOR N STAGE DEFINITION")
60
THE NEW STAGING SISTEM International gudelines for N definition - AIOM - ESMO - ASCO - NCCN - ACCP

61
NORMAL CT MEDIASTINUM N1 or central lesion (independent from PET scan) EUS-NA or EBUS- TBNA NEGATIVE MEDIASTINOSCOPY CT STAGE I-IIIb SUITABLE FOR SURGERY PET SCAN for medastinal staging NEGATIVEPOSITIVE SURGERY MEDIASTINAL LN SAMPLING 2007 (first choice)
 EUS-NA or EBUS- TBNA NEGATIVE MEDIASTINOSCOPY CT STAGE I-IIIb SUITABLE FOR SURGERY PET SCAN for medastinal staging NEGATIVEPOSITIVE SURGERY MEDIASTINAL LN SAMPLING 2007 (first choice)")
62
CT N2-3 M0 (independent from PET scan) Tissue confIrmation EUS-NA or EBUS- TBNA (first choice) POSITIVE NEGATIVE MEDIASTINOSCOPY MULTIMODALITY TREATMENT POS NEG SURGERY 2007
 Tissue confIrmation EUS-NA or EBUS- TBNA (first choice) POSITIVE NEGATIVE MEDIASTINOSCOPY MULTIMODALITY TREATMENT POS NEG SURGERY 2007")
63
THE NEW STAGING SISTEM Limiting of TNM staging - No hystologic type differences - No clinical status differences - Limited/No biological information

64
CONCLUSIONS 1 -Staging is a multidisciplinary process involving imaging, medical and surgery techniques - Accurate pretreatment staging is crucial for an adequate treatment plan - Changes in the new TNM edition mainly involved T size stratification, multiple nodes and pleural effusion

65
CONCLUSIONS 2 - Mediastinoscopy is the first choice in patients with suspected N1 and for central tumor with normal radiographic mediastinum - In patients with suspected N2-3 disease tissue confirmation with ultrasound biopsy is indicated (first choice). Mediastinoscopy is of second choice after negative ultrasound biopsy - Combined EUS/EBUS could replace mediastinoscopy in the future

66
Il nuovo sistema di stadiazione TNM definisce il nodulo polmonare in altro lobo ipsi-laterale come: 1.T3 2.T4 3.M1 1 / 30 Cross-tab label

67
Qual è la metodica di stadiazione suggerita come prima scelta per la stadiazione del mediastino con sospetto N2? 1.TAC + PET + TBNA 2.TAC + PET + EBUS/EUS 3.TAC + PET + mediastinoscopia 1 / 30 Cross-tab label

Similar presentations















-guided transbronchial needle aspiration (TBNA), PET, CT for detection of mediastinal.>")






