Download presentation
Presentation is loading. Please wait.

1
ESTIMATING THE IMPACT OF MATERNAL, NEONATAL AND CHILD SURVIVAL INTERVENTIONS Ingrid Friberg, PhD

2
The Lives Saved Tool - LiST The Lives Saved Tool A multi-cause model of mortality Predict changes in Under 5 and neonatal mortality rates and deaths Maternal mortality ratios and deaths Stillbirth rates and deaths Causes of death Using Country specific health status Changes in child and maternal health intervention coverage levels i.e. ORS, facility delivery, etc. Effect sizes of interventions based on the best available evidence

3
LiST 3 Beginnings: Grew out of the “Bellagio” modeling exercise and the Lancet Child Survival Series (2003). Added in neonatal, nutrition, and updated information Goals: Promote evidence-based decision making Aid in planning expansion of maternal, neonatal and child health interventions Objectives: Estimate lives saved when introducing or scaling up key interventions

4
Demographic estimates and projections UN Pop/Spectrum Number of Child, Maternal and Fetal deaths Deaths by Cause WHO/UNICEF Country estimates Deaths averted - By cause - By intervention General Framework Intervention Coverage Current Target/Goal/Endline *Change is critical* Health Status Stunted, wasted Malaria prevalence Vit A deficiency Zinc deficiency Stunting, Wasting, Breastfeeding Effectiveness Estimates Intervention Impact C1 C2 C3 C4 … Int1 Int2 Int3

5
Which interventions were included? Proximate factors Not distal Work through health programs Not included: income, education and crowding, etc. Water and sanitation are the exceptions Feasible in a low income country 68 priority countries with highest MNCH mortality Cause-specific evidence of effect Research studies or systematic reviews Delphi method if research is impossible (i.e. CEmOC) Updated frequently IJE April 2010, BMC Public Health April 2011
 Updated frequently IJE April 2010, BMC Public Health April")
6
Intervention Types Maternal, fetal, neonatal, child Periconceptional, antenatal, birth, immediate postnatal, child Preventive, curative Nutritional, vaccination, water/sanitation, treatment Risk factors: Cause-of-death specific Immediate, time-lagged External (family planning, AIDS), internal (all others)
, internal (all others)")
7
Periconceptional Interventions Pregnancy Interventions (Family planning) Folic acid supplementation or fortification Safe abortion services Post abortion case management Ectopic pregnancy case management Tetanus toxoid vaccination IPTp – malaria prevention in pregnancy Syphilis detection and treatment Calcium supplementation Multiple micronutrient supplementation Balanced energy supplementation Diabetes case management Maternal malaria case management MgSO4 – management of pre-eclampsia Fetal growth restriction and management (PMTCT)
 Folic acid supplementation or fortification Safe abortion services Post abortion case management Ectopic pregnancy case management Tetanus toxoid vaccination IPTp – malaria prevention in pregnancy Syphilis detection and treatment Calcium supplementation Multiple micronutrient supplementation Balanced energy supplementation Diabetes case management Maternal malaria case management MgSO4 – management of pre-eclampsia Fetal growth restriction and management (PMTCT)")
8
Childbirth Care Interventions Clean birth practices Immediate assessment and stimulation of the neonate Labor and delivery management SBA at home or facility, BEmONC and CEmONC Neonatal resuscitation At home or facility Antenatal corticosteroids for preterm labor Antibiotics for pPRoM MgSO4 – for eclampsia AMTSL – active management of the third stage of labor Induction of labor for pregnancies 41+ weeks

9
Preventive Interventions Thermal care Clean postnatal practices Breastfeeding Promotion Behavior Complementary feeding Education only Education and supplementation Vitamin A for prevention Zinc for prevention Insecticide treated materials Improved water source Water connection in the home Improved sanitation latrine, toilet Hand washing with soap Hygienic disposal of children’s stools BCG vaccine Polio vaccine Pentavalent vaccine DPT, Hib, HepB Pneumococcal vaccine Rotavirus vaccine Measles vaccine

10
Curative Interventions Maternal sepsis case management Kangaroo mother care Case management of serious neonatal illnesses Oral antibiotics Injectable antibiotics Full supportive care: oxygen, IV fluids, IV antibiotics ORS for diarrhea Antibiotics for dysentery Zinc for treatment of diarrhea Oral antibiotics for management of pneumonia Vitamin A for measles treatment Therapeutic feeding Antimalarials (Cotrimoxazole for HIV+ children) (ART for children)
 (ART for children)")
11
What’s NOT in the model? Education Motivation Gender issues Economic status Emergencies (i.e. famine, flooding) Delivery mechanism Only as relates to total population coverage Quality of care Effectiveness values, adjustments Assumption: Several of these factors are DISTAL factors which MAY work through COVERAGE changes…thus MAY already be in the model
 Delivery mechanism Only as relates to total population coverage Quality of care Effectiveness values, adjustments Assumption: Several of these factors are DISTAL factors which MAY work through COVERAGE changes…thus MAY already be in the model.")
12
Other things not in LiST De-worming (yet) IPTi (yet) Breastfeeding initiation within 1 hour (yet) Birth spacing benefit Treatment of water in the home Iron (or iron-folate) supplementation Indoor air pollution …
 IPTi (yet) Breastfeeding initiation within 1 hour (yet) Birth spacing benefit Treatment of water in the home Iron (or iron-folate) supplementation Indoor air pollution …")
13
What LiST is, What LiST isn’t! Multi-cause mortality model Mathematic model Models coverage impacts Potential impact assessment National or sub-national prioritization tool Discussion points Evidence-based Truth Probabilistic model Natural history model Detailed costing or planning tool Bottlenecks, budgeting Exhaustive Is Isn’t

14
DATA AND MODELING

15
Data Needs Country-Specific Population data and trends Default: UN Population Division 1950-2050 (DemProj) User entered (district) data Cause of death structure Default: WHO/UNICEF/CHERG (2008) User entered data Intervention coverage Population based data Default: DHS/MICS/JMP/WHO-UNICEF (closest to 2008) User entered data Global Intervention Effectiveness data User entered data
 User entered (district) data Cause of death structure Default: WHO/UNICEF/CHERG (2008) User entered data Intervention coverage Population based data Default: DHS/MICS/JMP/WHO-UNICEF (closest to 2008) User entered data Global Intervention Effectiveness data User entered data")
16
Stunting Zinc Diarrhea incidence IUGR Appropriate Complementary Feeding Complementary feeding education and/or supplementation Previous Stunting

17
Malaria Mortality Disease Specific Treatments Disease Specific Preventions Risk factors ITN/IRS Antimalarials Stunting Wasting

18
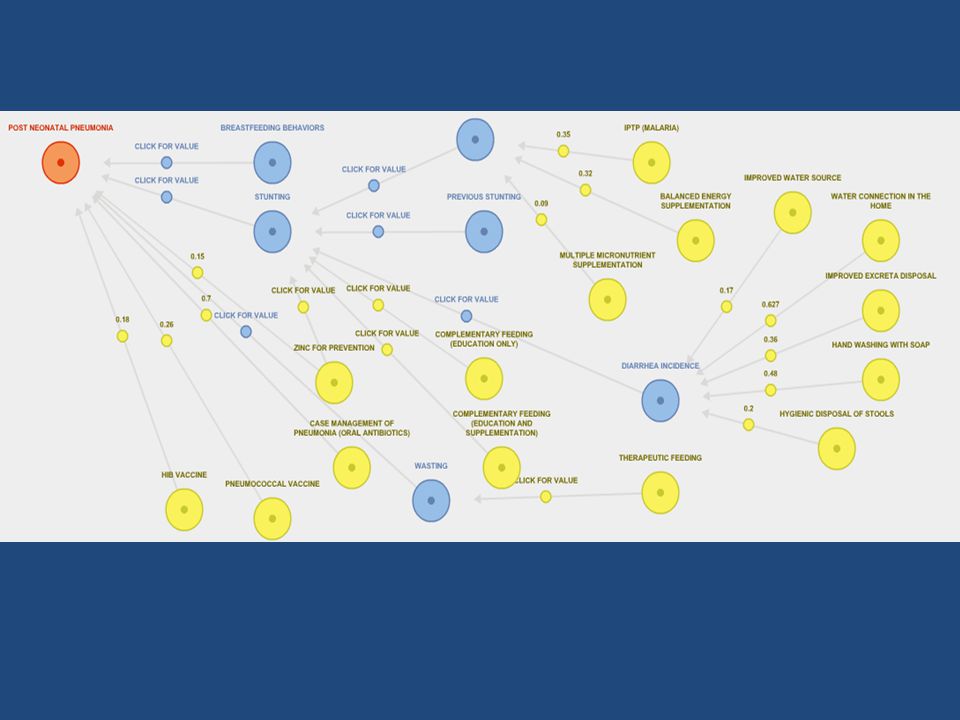
Pneumonia Mortality Hib vaccine Breast Feeding Promotion Pneumococcal vaccine Oral antibiotics for pneumonia Zinc for prevention Diarrhea incidence Improved H 2 O source within 30 minutes Hand washing with soap Water connection in the home Improved sanitation Hygienic disposal of children’s stools Stunting IUGR Pregnant women protected via IPT or sleeping under an ITN Balanced energy supplementation Multiple micronutrient supplementation Breast Feeding Wasting Therapeutic feeding Complementary feeding education/supplementation

20
How are the models built? Preventions Treatments Risk factors Multiple interventions? Two Preventions (or Risk Factors): Proportional impact by coverage/effect size Calculated on residual deaths No double counting Preventions and Treatments: Enter prevention(s), then treatment(s) Deaths not already averted
: Proportional impact by coverage/effect size Calculated on residual deaths No double counting Preventions and Treatments: Enter prevention(s), then treatment(s) Deaths not already averted.")
21
Some Limitations Data availability If no baseline, can’t evaluate impact accurately Data quality Sensible scale up targets Feasible, acceptable, funds available Interventions included in software Some evaluated for one outcome, not others Maternal No country specific cause of death yet; regional causes No risk factors yet Not yet vetted intervention impacts through CHERG and other groups

22
LIST “VALIDATION” USES

23
Neonatal Package Modeling

24
ACSD Results

25
Modeling Mortality Rates and Equity

26
ITN studies

27
How can LiST be used? Planning, Evaluation, Research, Advocacy Strategic planning Which interventions are necessary to reduce mortality? (maternal, neonatal, under-5) Will the targets reduce mortality as much as needed? Evaluation and intermediate-term follow-up What is the impact of observed coverage changes? Evaluation of historic trends (i.e. multiple DHS/MICS surveys) Predict lives saved (past and future) How many lives could be saved with full scale-up of proven interventions in priority countries? How many deaths remain left after vaccination scale ups?
 Will the targets reduce mortality as much as needed. Evaluation and intermediate-term follow-up What is the impact of observed coverage changes. Evaluation of historic trends (i.e. multiple DHS/MICS surveys) Predict lives saved (past and future) How many lives could be saved with full scale-up of proven interventions in priority countries. How many deaths remain left after vaccination scale ups .")
28
How has LiST been used? Globally Global Action Plan for Pneumonia ‘Impatient Optimist’ speech by Bill Gates Regionally ASADI, by Saving Newborn Lives Country level Catalytic initiative: to guide planning and priority setting ( Malawi, Ghana, Niger) Ethiopia Sub-nationally CSHGP DFID in Nigeria (PRRINN-MNCH)
 Ethiopia Sub-nationally CSHGP DFID in Nigeria (PRRINN-MNCH).")
29
Who has used LiST? Gates Foundation, GAVI USAID, DFID, CIFF MCHIP Save the Children, Saving Newborn Lives, MSH WHO (GAPP), UNICEF CHAI
, UNICEF CHAI.")
30
How NOT to use LiST As the correct answer It depends on what you put in and what your goals are Also must consider cost, feasibility, accepability To suggest decreasing coverage of any interventions Mortality has declined BECAUSE of those interventions To suggest taking funds away from interventions To suggest that things in LiST are “GOOD” while everything else is “BAD” It is based upon data availability unless otherwise stated To decide HOW to do anything!!! That is for the programmers to decide!

31
What can I get out of LiST? Number of deaths Total, by cause, by age group Mortality rates/ratios (NMR, U5MR, MMR, SBR) Deaths averted, Total, by cause, by intervention, by age group Intermediate outcomes Stunting, wasting, breastfeeding Displays Tables, graphs, pie charts Single country, multiple scenarios within one country Multiple countries, single or multiple scenarios
 Deaths averted, Total, by cause, by intervention, by age group Intermediate outcomes Stunting, wasting, breastfeeding Displays Tables, graphs, pie charts Single country, multiple scenarios within one country Multiple countries, single or multiple scenarios.")
32
Future Directions for LiST Costing tie-ins Both a CHOICE based costing tool and MBB Part of the new One Health Model Yes, we will be adding in uncertainty Improve the maternal model A new tool for multi-country analyses

33
LiST Resources FREE Web Links www.futuresinstitute.org www.healthpolicyinitiative.com/index.cfm?id=software&get =Spectrum www.jhsph.edu/iip/list (join the listserv there) list.cherg.org Software + Manual Languages English, French, Spanish, Portuguese Contact Ingrid Friberg - ifriberg@jhsph.edu
 list.cherg.org Software + Manual Languages English, French, Spanish, Portuguese Contact Ingrid Friberg -")
Similar presentations















: How to create a sub-national projection Ingrid Friberg, PhD.>")
: A few details What you need to know to actually make this program work and work well…>")


