Download presentation
Presentation is loading. Please wait.

1
What is the optimal method of fetal surveillance in a SGA infant ? What is the frequency of fetal surveillance in a SGA infant ? What is/are the optimal test/s to time delivery ?

2
Biophysical tests, including amniotic fluid volume, cardiotocography (CTG) and biophysical scoring are poor at diagnosing a small or growth restricted fetus. A systematic review of the accuracy of umbilical artery Doppler in a high–risk population to diagnose a SGA neonate has shown moderate.

3
Umbilical artery Doppler Cardiotocography (CTG) Amniotic fluid volume Biophysical profile Middle cerebral artery Ductus venusus (DV) & Umbilical vein Doppler
 Amniotic fluid volume Biophysical profile Middle cerebral artery Ductus venusus (DV) & Umbilical vein Doppler")
4
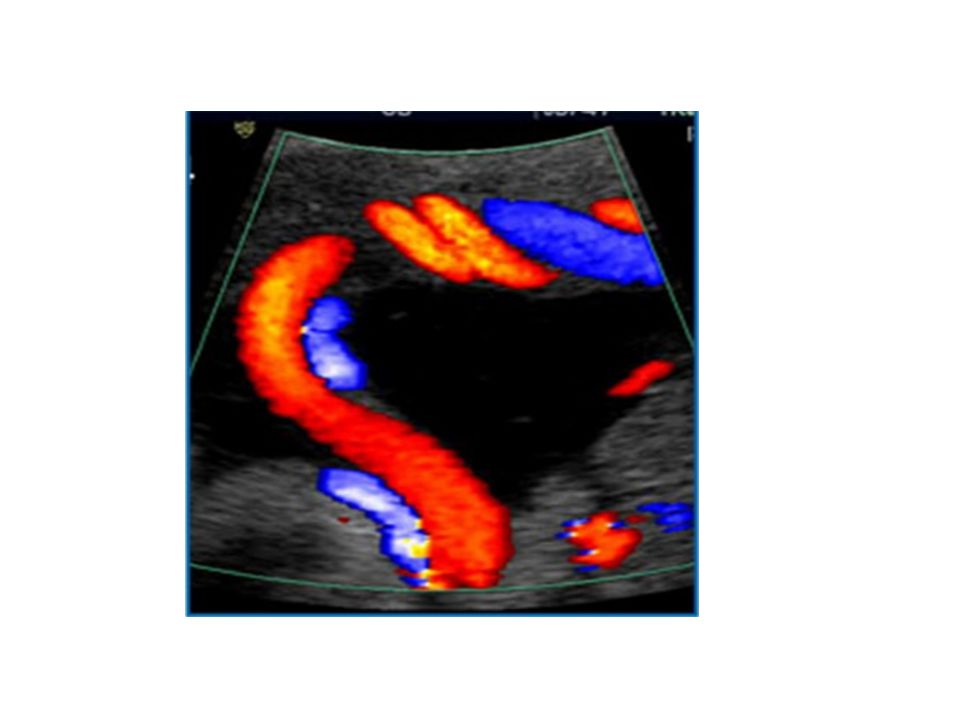
Umbilical artery Doppler In high-risk population, the use of umbilical artery Doppler has been shown to reduce prenatal morbidity & mortality

5
Umbilical artery Doppler Umbilical artery Doppler should be performed in all fetuses with an estimated fetal weight or an abdominal circumference < 10 th percentile (I- A)
")
6
Umbilical artery Doppler Umbilical artery Doppler should be the primary surveillance tool in the SGA fetus.

10
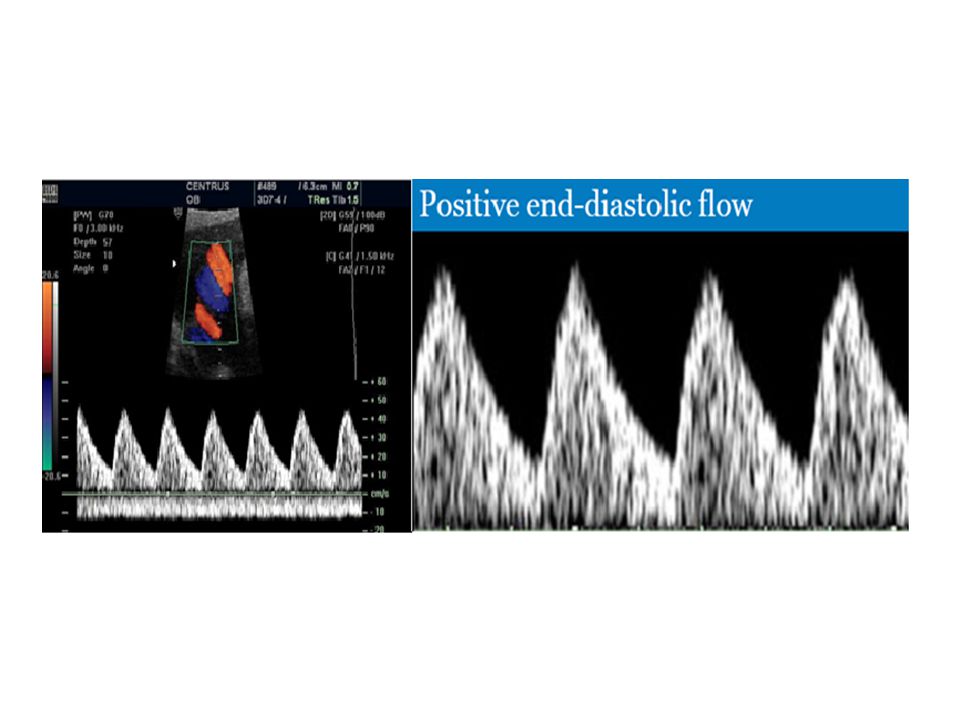
Frequency of Normal Umbilical artery Doppler flow indices in SGA fetus: Defined by customized fetal weight standards 81 % of SGA fetuses have a normal umbilical artery Doppler

11
Management of Normal Umbilical artery Doppler flow indices in SGA fetus: Outpatient management is safe in this group When umbilical artery Doppler flow indices are normal it is reasonable to repeat surveillance every 14 days. More frequent Doppler surveillance may be appropriate in a severely SGA infant.

12
However Compare to AGA, SGA fetuses with a normal umbilical artery Doppler are still at increased risk of neonatal morbidity & adverse neurodevelopmental outcome

13
Which Umbilical artery Doppler waveform index ? The large systematic review of test accuracy couldn't comment on which waveform index to use. Although PI has been widely adopted in the UK, an analysis using receiver operator curves found that IR had the best discriminatory ability to predict a range of adverse perinatal out come

14
Routine umbilical artery Doppler In a low risk or unselected population, systematic review found no conclusive evidence that routine umbilical artery Doppler benefits mother or baby. As, such, umbilical artery Doppler is not recommended for screening an unselected population.

15
Cardiotocography (CTG) CTG should not be used as the only form of surveillance in SGA fetuses. Interpretation of the CTG should be based on short term fetal heart rate variation from computerized analysis (A)
.")
16
The most useful CTG predictor: FHR variation is the most useful predictor of fetal wellbeing in SGA fetuses. A short term variation 3 ms (within 24 h of delivery ) has been associated with a higher rate of metabolic acidemia & early neonatal death
 has been associated with a higher rate of metabolic acidemia & early neonatal death.")
17
Comparison of cCTG with traditional CTG showed a reduction in perinatal mortality with cCTG but no significant difference in perinatal mortality excluding congenital anomalies

18
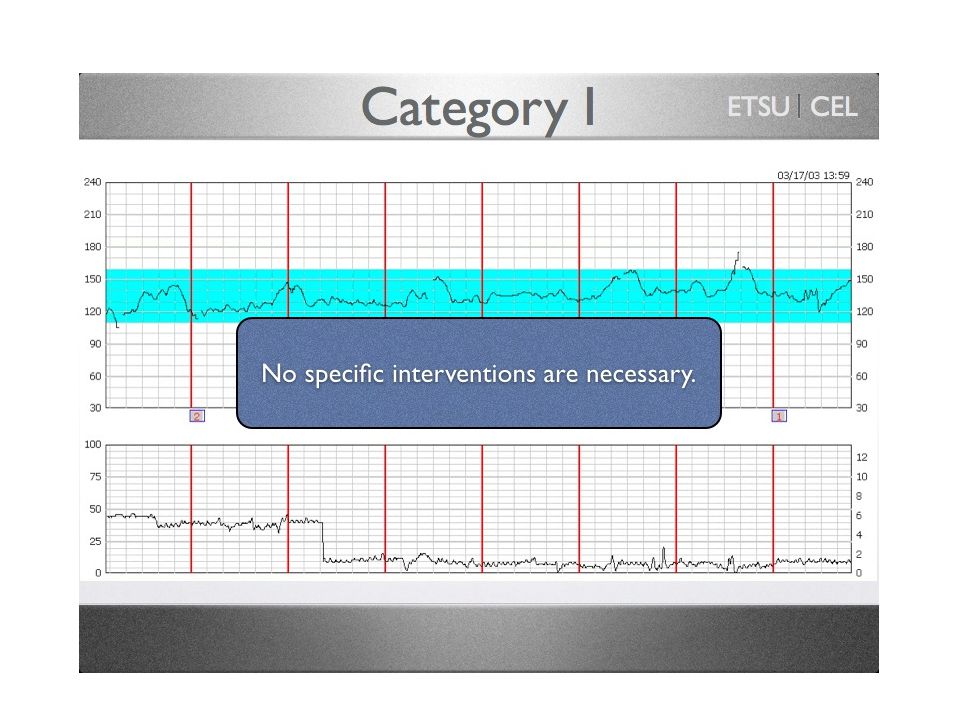
رده 1 نوار ضربان قلب جنین خصوصیات رده 1 عبارتند از : تعداد ضربان قلب پایه در محدوده طبیعی ( از 110 تا 160 ضربان در دقیقه ) تغییر پذیری پایه متوسط ( از 6 تا 25 ضربان در دقیقه ) فقدان افت متغیر و دیر رس وجود یا عدم وجود تسریع ضربان قلب احتمال وجود افت زودرس ضربان قلب این گروه به عنوان " طبیعی " تلقی شده و نشان دهنده این است که جنین در لحظه ثبت نوار ، از نظر وضعیت اسید – باز در وضعیت طبیعی بسر می برد
 تغییر پذیری پایه متوسط ( از 6 تا 25 ضربان در دقیقه ) فقدان افت متغیر و دیر رس وجود یا عدم وجود تسریع ضربان قلب احتمال وجود افت زودرس ضربان قلب این گروه به عنوان طبیعی تلقی شده و نشان دهنده این است که جنین در لحظه ثبت نوار ، از نظر وضعیت اسید – باز در وضعیت طبیعی بسر می برد")
21
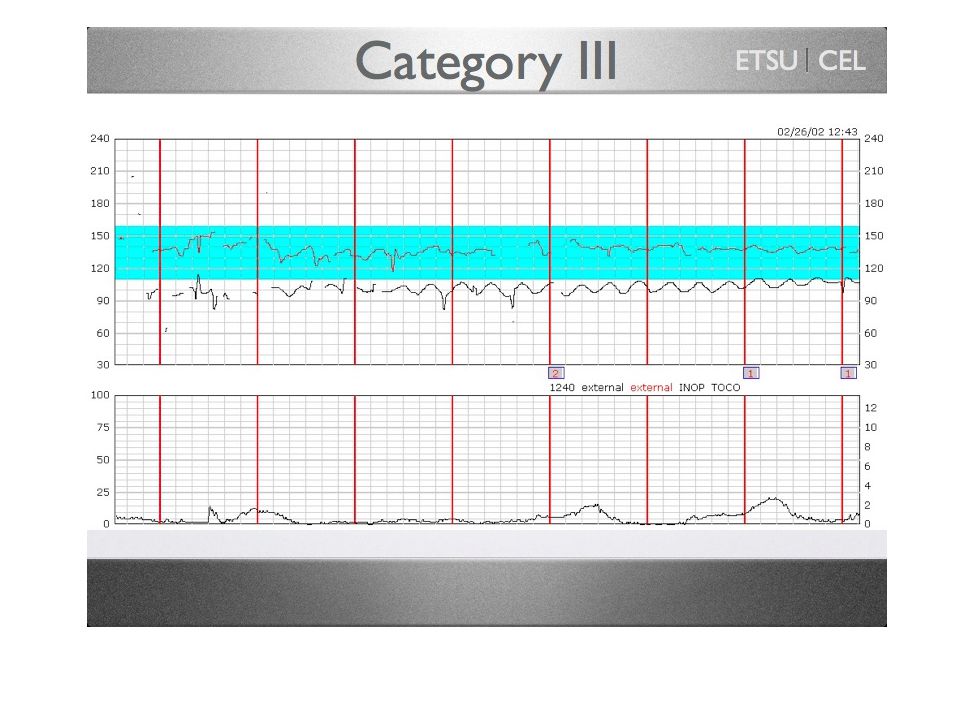
رده 3 نوار CTG خصوصیات این رده عبارتند از فقدان تغییر پذیری پایه ضربان قلب جنین به همراه هر کدام از موارد ذیل : - افت دیررس مکرر ضربان قلب - افت متغیر مکرر ضربان قلب - کندی ضربان قلب جنین ( برادیکاردی ) الگوی سینوزوئیدال این رده با رنگ قرمز ( خطر ) نشان داده شده و به عنوان " غیر طبیعی " تلقی گردیده و نشان دهنده وضعیت غیر طبیعی اسید - باز جنین در موقع ثبت نوار است. در موارد مواجهه با این گروه لازم است که اقدامات فوری و مناسب در جهت بهبودی وضعیت جنین صورت گیرد و در صورتی که حداکثر در عرض 30 دقیقه مشکل برطرف نشد ، زایمان مد نظر قرار گیرد.

24
رده 2 نوار ضربان قلب جنین : این دسته از نوار به عنوان " حد واسط " تلقی می شود زیرا که شامل تمامی الگوهایی است که جز رده 1 یعنی رده " طبیعی " و رده 2 یعنی " غیر طبیعی " قرار نمی گیرند. انجمن زنان و مامایی کانادا این رده را بعنوان " غیر معمول " نام گذاری گرده است. روش استانداردی برای بررسی وضعیت این جنین ها بیان نشده است. بطور کلی وجود تغییر پذیری پایه متوسط ( دامنه معادل 6 تا 25 ضربان در دقیقه ) و تسریع ضربان قلب نشانگر وضعیت طبیعی تعادل اسید - باز جنین بوده و نیازی به زایمان فوری نیست این بیماران باید مرتبا تا زمانی که تبدیل به رده 1 یا 3 شوند، تحت نظر بوده و مکررا بررسی شوند.
 و تسریع ضربان قلب نشانگر وضعیت طبیعی تعادل اسید - باز جنین بوده و نیازی به زایمان فوری نیست این بیماران باید مرتبا تا زمانی که تبدیل به رده 1 یا 3 شوند، تحت نظر بوده و مکررا بررسی شوند..")
27
Amniotic fluid volume Ultrasound assessment of amniotic fluid volume should not to be used as the only form of surveillance in SGA fetus

28
Amniotic fluid volume is usually estimated by the single deepest vertical pocket (SDVP) or amniotic fluid index(AFI), although both correlate poorly with actual amniotic fluid volume
 or amniotic fluid index(AFI), although both correlate poorly with actual amniotic fluid volume")
29
Interpretation of amniotic fluid volume should be based on single deepest vertical pocket (SDVP).
.")
30
The incidence of an AFI ≤ 5 cm in a low risk population is 1.5%. Compared to cases with a normal AFI, the risk of perinatal mortality and morbidity was not increased in cases with isolated oligohydramnios ( RR 0.7, 95% CI 0.2–2.7) nor in those with associated conditions, including SGA fetuses (RR 1.6, 95% CI 0.9–2.6).
 nor in those with associated conditions, including SGA fetuses (RR 1.6, 95% CI 0.9–2.6)..")
31
Oligohydramnios is associated with labour outcome: a systematic review of 18 studies involving 10551 women, found an AFI ≤ 5 cm was associated with an increased risk of caesarean section for fetal distress (RR 2.2, 95% CI 1.5–3.4) and an Apgar score < 7 at 5 minutes (RR 5.2, 95% CI 2.4–11.3) but not acidaemia. limited information is available about the accuracy of oligohydramnios to independently predict perinatal mortality and substantive perinatal morbidity in non– anomalous SGA fetuses monitored with umbilical artery Doppler

32
Biophysical profile Consist of a NST + 4 ultrasound component : fetal movement, fetal muscle tone, amniotic fluid volume, fetal breathing movement. A BPP is an appropriate second line (back-up) testing strategy when the NST component is non-reactive or none – interpretable
 testing strategy when the NST component is non-reactive or none – interpretable.")
33
Biophysical profile (BPP) Biophysical profile should not be used for fetal surveillance in preterm SGA fetuses.
 Biophysical profile should not be used for fetal surveillance in preterm SGA fetuses.")
34
What is the optimal method of fetal surveillance in a SGA infant ? What is the frequency of fetal surveillance in a SGA infant ? What is/are the optimal test/s to time delivery ?

Similar presentations








: Part 3 – Antepartum>")
>")














