Download presentation
Presentation is loading. Please wait.

1
Geraldine O’Dowd Consultant Pathologist NHS Lanarkshire 18 th November 2014 Colorectal Cancer Pathology: Impact of new guidelines for the laboratory

2
Introduction Colorectal cancer is common in Scotland Important part of workload in most laboratories New developments: New RCPath. guidelines Colorectal screening ICC and molecular testing

3
Plan Focus on new RCPath. guideline 2014 Gross dissection Venous invasion Cases without obvious cancer Colorectal screening impact ICC and molecular testing developments

4
RCPath. Minimum Dataset

5
Background Changes in pathology reporting requirements and in clinical expectations occur with time Major impact for lab and consultant workload The report…..

6
Pathology Reports

7
IN THE PAST: Minimalist reporting Block of tumour, block of lymph nodes, maybe margins (max. around 5 blocks) Very brief report…..
 Very brief report…...")
14
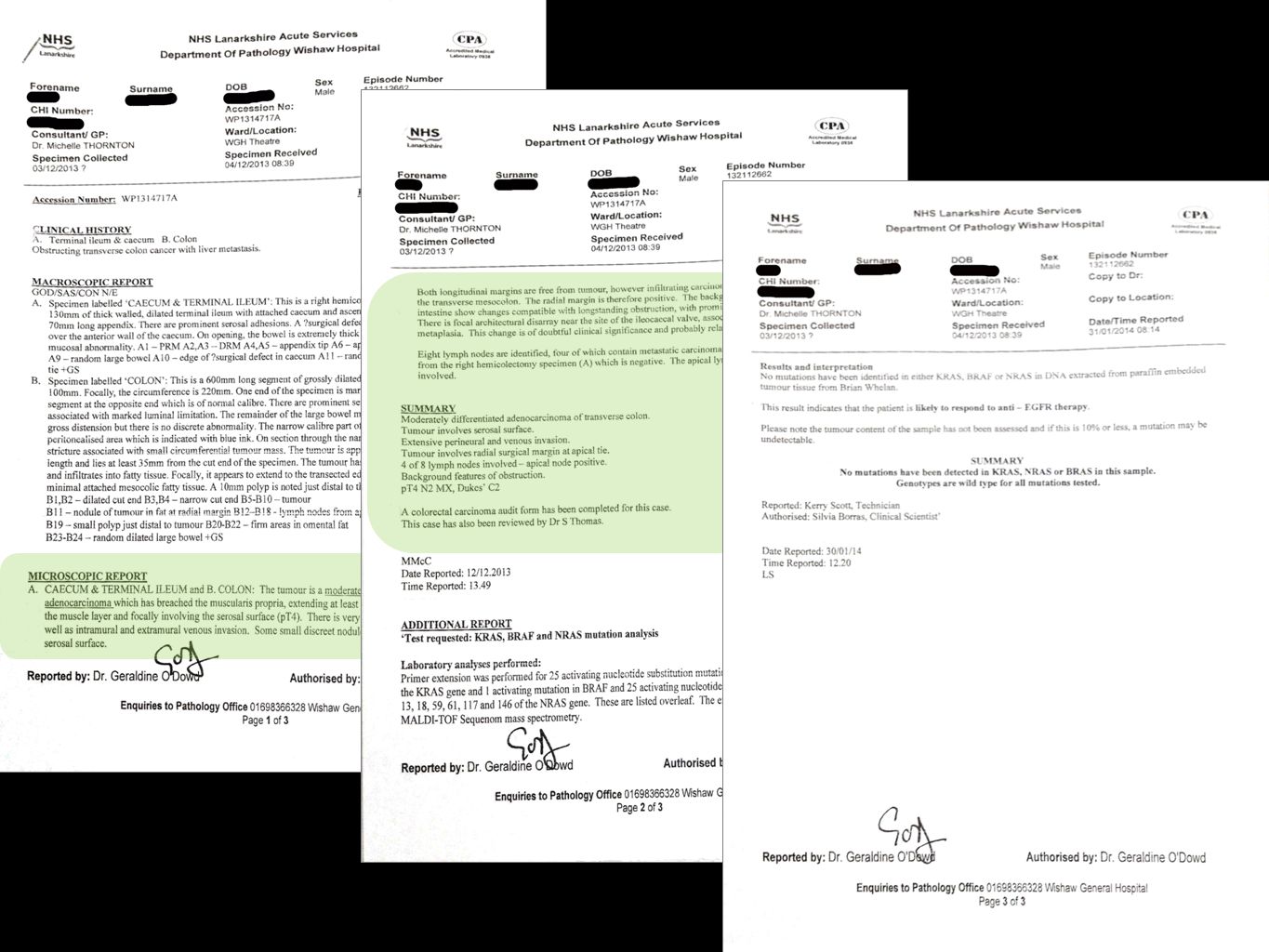
NOW: Requires use of ‘minimum’ dataset More tumour blocks All lymph nodes Complex margin assessment Use of ICC and routine special stains Many blocks (often more than 40) Additional molecular testing
 Additional molecular testing")
19
Dissection

20
Specimen dissection Hemicolectomies, anterior resections and abdominoperineal resections Colorectal trimming is time consuming macroscopic assessment and handling is critical identification of anterior peritoneal reflection assessment of mesorectal plane quality marking of non peritonealised ( ‘ circumferential ’ ) margin
 margin")
22
From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July 2014.

23
.

24
Specimen dissection Specimen photography- time consuming Ink to mark non-peritonealised circumferential margin Open specimen and clean but, where possible, avoid opening through tumour Good fixation (College recommends at least 48h) Careful cutting into thin transverse slices (around 3 to 6mm), arranged to preserve anatomical orientation
 Careful cutting into thin transverse slices (around 3 to 6mm), arranged to preserve anatomical orientation")
25
PROXIMAL DISTAL POSTERIOR ANTERIOR R L LEVEL OF APR 1 2 3 4 5 6 7 8 9 10

26
PROXIMAL DISTAL POSTERIOR ANTERIOR R L LEVEL OF APR 1 2 3 4 5 6 7 8 9 10 6 7

27
From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July 2014.

31
Specimen dissection Selection of blocks for histological examination standard versus ‘ macro ’ blocks relationship to peritoneum (determines pT3 or pT4) relationship to layers of bowel wall (good sampling to avoid understaging) proximity to margins venous or perineural invasion role of special staining to improve detection discontinuous deposits of tumour in mesorectum
 relationship to layers of bowel wall (good sampling to avoid understaging) proximity to margins venous or perineural invasion role of special staining to improve detection discontinuous deposits of tumour in mesorectum")
32
From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July 2014.

34
Specimen dissection Lymph node examination apical node (nearest to surgical vascular tie) sequential sections through mesorectal fat to retrieve ALL lymph nodes if nodes are bisected in this process, care is required to avoid over staging (many pathologists process one node per block to avoid problems)
 sequential sections through mesorectal fat to retrieve ALL lymph nodes if nodes are bisected in this process, care is required to avoid over staging (many pathologists process one node per block to avoid problems)")
35
Histological reporting Tumour type, differentiation and stage Other pathological changes, e.g. polyps, IBD, diverticular disease, etc. Lymph node status Presence or absence of venous and perineural invasion extramural versus intramural veins elastic staining to aid recognition

38
Venous Invasion

40
Extramural vein Elastic layer below serosal surface

41
Extramural vein

43
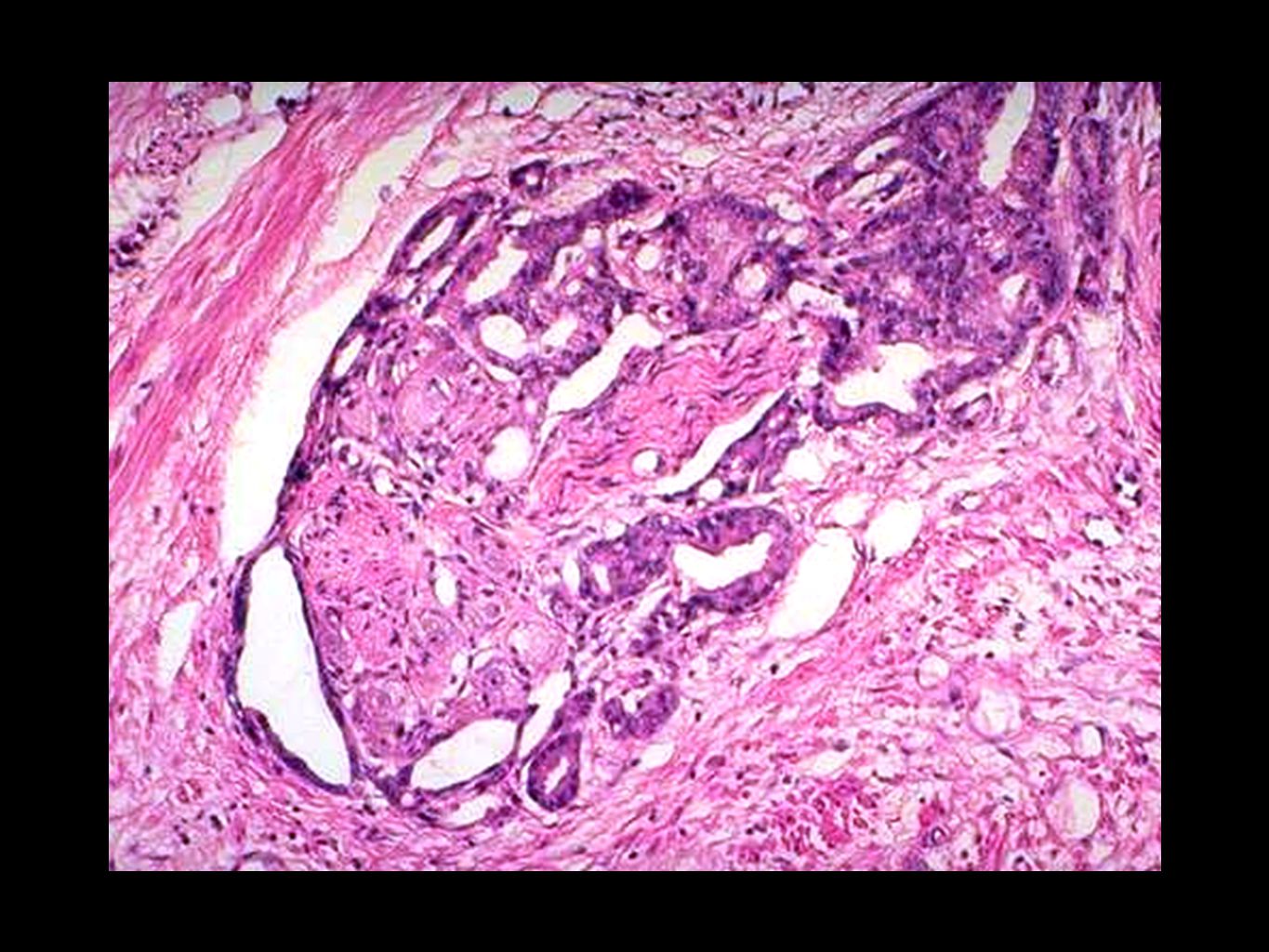
Intramural venous invasion

44
Identifying the Tumour Site

45
Where’s the cancer?!? Problems in 2 main settings: Pre-operative chemoradiotherapy Previous polypectomy with cancer Must identify correct part of bowel to process Need good clinical and radiological information May need many blocks and levels Must identify tumour bed or scar site

46
College guidance “Rectal tumours that have undergone pre-operative therapy may undergo regression such that no definite residual tumour can be recognised. In such cases, at least five blocks from the site of the original mass should be taken in the first instance. If these do not show residual tumour on microscopic examination (after examining sections from three levels) then the whole of the tumour site and/or the scarred area should be blocked for histology. If still no tumour is found, three levels should be cut on all blocks from the tumour site and, if still negative, a pathology complete response can then be recorded.” From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July 2014.
 then the whole of the tumour site and/or the scarred area should be blocked for histology. If still no tumour is found, three levels should be cut on all blocks from the tumour site and, if still negative, a pathology complete response can then be recorded. From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July")
49
Molecular Testing

50
Molecular testing Evidence that some genes predict response to certain forms of chemotherapy, e.g. cetuximab K-RAS BRAF NRAS Testing of formalin-fixed, paraffin embedded tissue At present, usually requested for specific patients May allow curative treatment when irresectable disease Known prognostic value and may affect risk for other family members

51
College guidance “Mismatch repair (MMR) protein immunohistochemistry now has several well-recognised applications in colorectal carcinoma..... We now consider MMR immunohistochemistry a core dataset item for patients under 50 years at time of diagnosis and for patients, in whom an assessment of prognosis is appropriate, with adenocarcinomas classified as poorly differentiated morphologically or tumours showing other morphological features of MMR deficiency. It should also be available upon request by either oncologist or geneticist on individual cases..” From RCPath ‘ Dataset for Colorectal Cancer ’, 3rd edition, July 2014.

52
Consequences for the lab…

53
Consequences More time dissecting: photos, inking, macro blocks, etc. More blocks produced and so more sections to cut and stain Routine use of elastica staining on all tumour blocks More blocks and levels from cases without obvious cancer After Bowel Screening polypectomy After pre-operative chemoradiotherapy More use of ICC and molecular testing

54
Summary New guidelines have important consequences for workload at every level More time trimming More blocks More sections More special stains and ICC More molecular testing Longer reports to produce and to type Those involved in planning must consider likely future service developments

55
Any questions? END!

Similar presentations






























 Sibley Memorial Hospital Washington, DC.>")







