Download presentation
Presentation is loading. Please wait.

1
Reporting and Management of Early stage Colorectal Cancer Frank Carey Dundee

2
First Principles Screening is about reducing disease- specific mortality The best surrogate marker of success is detection of a high proportion of cancers at early stage

3
Stage Distribution of Symptomatic Colorectal Cancer A8% D25% B33% C34%

4
Stage Distribution of Screen -Detected Cancers True A 26% 48% C26% Polyp Cancers 22% D1% B25%

5
Early stage colorectal cancer Dukes A (T1, T2) Cancer confined to submucosa (T1) We are concerned mainly with the latter
 Cancer confined to submucosa (T1) We are concerned mainly with the latter")
6
Pathology Reporting Early stage cancer in formal surgical resections Cancer in local resections (polypectomy and others) Together these make up 50% of screen- detected cancers Add Dukes’B (T3/T4) and we have 75%
 Together these make up 50% of screen- detected cancers Add Dukes’B (T3/T4) and we have 75%")
7
Early Cancer in Surgical Resections RCPath dataset does not allow for subdivision of T1 tumours apart from in terms of tumour differentiation One effect of screening is that we may detect biologically more aggressive lesions at an early stage There may be a need to look more carefully at these tumours

8
screen

9
Non-core data items Nature of advancing margin Tumour infiltrating lymphocytes Tumour budding Intramural venous invasion (Petersen et al Gut 2002; 51:65) Immunohistochemical and/or molecular data
 Immunohistochemical and/or molecular data")
10
Submucosal venous invasion Loses prognostic significance when all stages are analysed Valid in Dukes’ B Indicator of bad prognosis in locally resected cancer Need for study in screened population, especially in Dukes’ A resections

11
“Jass” parameters Margin characteristics Lymphoid reaction/tumour infiltrating lymphocytes

12
Early colorectal cancer Identification: –Endoscopic Pedunculated Flat Depressed –Pathological

13
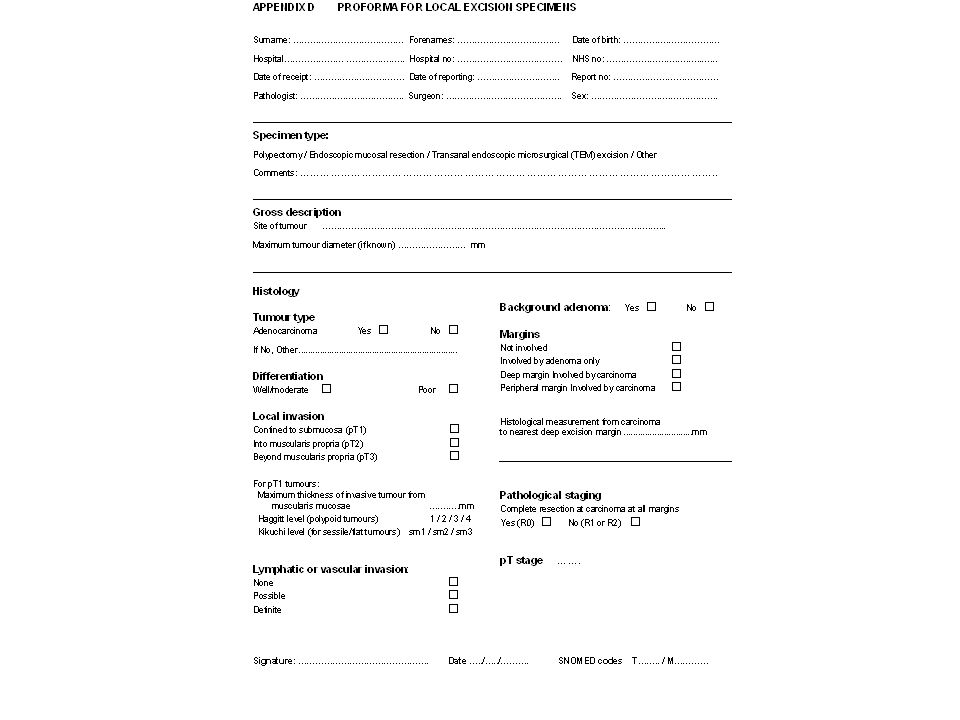
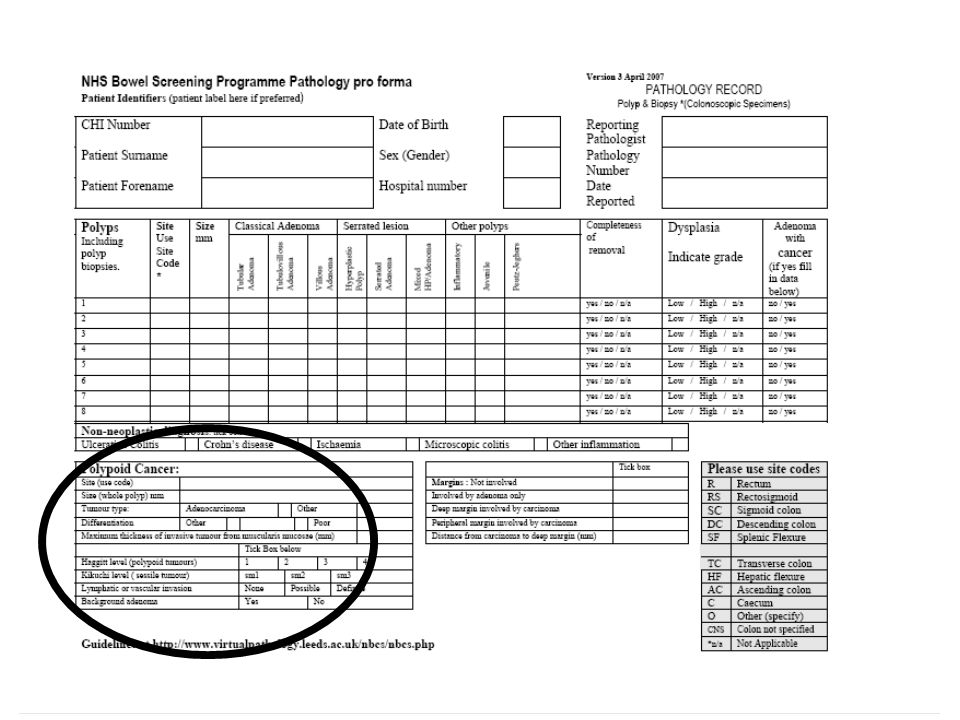
Presentation to pathology Polypectomy for presumed adenoma –Pedunculated –Sessile Specialised resections for larger sessile lesions –Endoscopic mucosal resection (EMR) –Transanal endoscopic microsurgical resection (TEMS)
 –Transanal endoscopic microsurgical resection (TEMS)")
14
Macroscopic handling Measurement All should be handled as potential cancer (all tissue submitted, preservation of the stalk etc.)
")
15
EMR/TEMS should be received pinned on cork –Fixed “face down” –Margins inked

16
Microscopy Often a difficult problem….. How reproducible is this diagnosis? See Neil Shepherd…

17
Help is at hand!

18
Microscopy Differentiation –Even focal poor differentiation is reported and is an indicator for further surgical therapy

19
Microscopy Tumour budding Detached groups of up to 5 cells at invading front –Not included in reporting recommendations –Need for more research

20
Microscopy Assessment of depth of invasion (if completely excised) –Direct measurement from muscularis mucosae (Ueno et al) Depth >2mm 20% nodal mets (vs. 5%) Width of invasive front >4mm 20% node positive (vs. 4%)
 Width of invasive front >4mm 20% node positive (vs. 4%).")
21
Measuring invasive tumour Accuracy of depth measurement questionable

22
Haggitt levels For polypoid adenomas Often difficult in practice

23
Depth of invasion…. Haggitt system failings –Study included high grade dysplasia (level 0) –1/3 of cases were surgical excisions –Statistical comparison was between level 4 and combined levels 0-3 (no node mets in levels 0-3)
 –1/3 of cases were surgical excisions –Statistical comparison was between level 4 and combined levels 0-3 (no node mets in levels 0-3).")
24
Kikuchi levels Applicable to sessile adenomas sm1sm2 sm3

25
Depth of invasion….. Kikuchi system –Refined sm1a – invading front < ¼ of width of lesion sm1b – invading front ¼ - ½ width of lesion sm1c – invading front > ½ width of lesion –Not currently recommended

26
Microscopy Margins –Involved by cancer –Involved by adenoma Definition of margin positivity –Direct involvement –1mm –2mm –5mm

27
Lymphatic or vascular invasion 3 categories allowed –Not present –Possibly present –Present Problem of retraction artefact –Worse near cauterised margin

30
A real case Polyp was margin clear Problem of ?vascular invasion discussed at MDT Surgery –1 positive node

31
Margin positivity Sigmoid polyp with a lot of diathermy artefact Called carcinoma R1

32
Resection after polypectomy Difficulty of finding polypectomy site Reassuring for endoscopist/surgeon!

33
Future developments Research studies looking at histological parameters in early stage cancers Identification of poor-prognosis groups Interventional trials of therapy Ensuring consistency of pathological reporting

Similar presentations





>")













