Download presentation
Presentation is loading. Please wait.

1
Acquired Aplastic Anaemia – Trends in treatment and Bone Marrow Transplantation Vikas Gupta, MD Blood and Marrow Transplant Program Princess Margaret Hospital University of Toronto Toronto vikas.gupta@uhn.on.ca

2
Objectives Management at Presentation Treatment strategies: Immunosuppressive therapy (IST) or Bone Marrow Transplant (BMT)
 or Bone Marrow Transplant (BMT)")
3
Aplastic anaemia bone marrow aspirate

4
Normal Severe aplastic anaemia

5
Aplastic anaemia

6
Etiologic classification Direct toxicity Iatrogenic causes Radiation Chemotherapy Benzene Intermediate metabolites of some drugs Immune-mediated causes Idiopathic Hepatitis associated disease Pregnancy Intermediate metabolites of some drugs Associated with autoimmune disorders

7
Management at Presentation Review of morphology Define disease severity (Camitta 1976; Bacigalupo 1988) Supportive care Management plan: BMT or IST
 Supportive care Management plan: BMT or IST")
8
Assessment of Disease Severity Severe AA (Camitta et al, 1976) BM cellularity <25% or 25-50% with <30% residual haemopoietic cells Two of the three of the following: Neutrophils <0.5 x 10 9 /l Platelets <20 x 10 9 /l Reticulocytes <20 x 10 9 /l Very-severe AA (Bacigalupo et al, 1988) Same as for SAA but neutrophils <0.2 x 10 9 /l Non-severe AA
 BM cellularity <25% or 25-50% with <30% residual haemopoietic cells Two of the three of the following: Neutrophils <0.5 x 10 9 /l Platelets <20 x 10 9 /l Reticulocytes <20 x 10 9 /l Very-severe AA (Bacigalupo et al, 1988) Same as for SAA but neutrophils <0.2 x 10 9 /l Non-severe AA")
9
Management at presentation Review of morphology Define disease severity (Camitta 1976; Bacigalupo 1988) Supportive care Treatment options: BMT or IST
 Supportive care Treatment options: BMT or IST")
10
HLA identical sibling BMT Initial treatment of choice if : severe or very severe aplastic anaemia HLA identical sibling age <40 yr Controversy over upper age limit

11
WP AA Registry: Survival for aplastic anaemia HLA identical sibling donors (1994 – 2003) SAA WP March 2004
 SAA WP March 2004")
12
Indications for immunosuppressive therapy (IST) Severe or very severe AA >40y of age Non-severe AA and transfusion dependent Severe or very severe AA <40 y with no compatible sibling donor
 Severe or very severe AA >40y of age Non-severe AA and transfusion dependent Severe or very severe AA <40 y with no compatible sibling donor")
14
What is the Optimum IST?

15
EBMT randomized study CSA vs. ATG + CSA (Marsh et al, Blood 1999)
")
16
ATG + CsA ATG P = 0.6 German randomised study Frickhofen et al, Blood, 2003

17
P = 0.04 ATG + CsA ATG German randomised study, Frickhofen et al, Blood, 2003

18
Is there a role for combining long term G-CSF with ATG and CSA?

19
Randomised study of ATG, CSA ± G-CSF, Gluckman 2002

20
G-CSF and risk of malignancy Japanese studies show increased risk Alarming high risk 45% in children Small European randomized study did not show increased risk EBMT observational study Incidence of AML/MDS With G-CSF10.9% Without G-CSF5.8% (Socie et al, Blood, 2006, available on line) Current randomized study by EBMT will probably provide a final answer in the future
 Current randomized study by EBMT will probably provide a final answer in the future")
21
Immunosuppressive therapy (IST) ATG + CSA is current standard of care of IST and is an effective treatment but 65-70% respond Delayed response One third of responders relapse secondary complications occur Risk of clonal disorders such as MDS/AML,PNH Cytogenetic evolution Solid tumors Time favours BMT over IST
 ATG + CSA is current standard of care of IST and is an effective treatment but 65-70% respond Delayed response One third of responders relapse secondary complications occur Risk of clonal disorders such as MDS/AML,PNH Cytogenetic evolution Solid tumors Time favours BMT over IST")
22
IST vs. BMT – Q-TwiST Study Viollier et al, Ann Haematol, 2005 Re-produced by permission of Andre Tichelli, Basel, Switzerland

23
Refractory/Relapse after first course of IST Treatment Options BMT – Related or unrelated donor Repeated course of ATG

24
Response to second course of ATG (Di Bona et al, BJH, 1999)
")
25
Response to third course of ATG (Gupta et al, BJH, 2005)
")
26
HLA identical sibling BMT - current issues 1. Graft versus host disease 2. Graft rejection How can results be improved further ?

27
WP AA Registry - HLA identical sibling donors - SAA WP March 2004

28
WP AA Registry HLA identical sibling donors (1994 – 2003) in patients surviving at least 100 days SAA WP March 2004
 in patients surviving at least 100 days SAA WP March 2004")
29
Is GVHD necessary for AA? Unlike BMT for malignancies, GVL is probably not necessary in AA With current protocols, 30-35% develop chronic GVHD Adverse impact of GVHD on Well-being Quality of life Fertility

30
Impact of GVHD on Fertility in AA (Deeg et al, Blood, 1997) Chances of becoming pregnant / fathered a child in long term BMT survivors of AA GenderWith GVHDNo GVHD Female26%61% Male29%62%
 Chances of becoming pregnant / fathered a child in long term BMT survivors of AA GenderWith GVHDNo GVHD Female26%61% Male29%62%")
31
An ideal protocol for BMT for AA Durable Engraftment Minimal Regimen-related toxicity Minimal risk of acute and chronic GVHD Preserves Fertility Applicable to a wider group of patients especially relatively older patients and those with co-morbidities

32
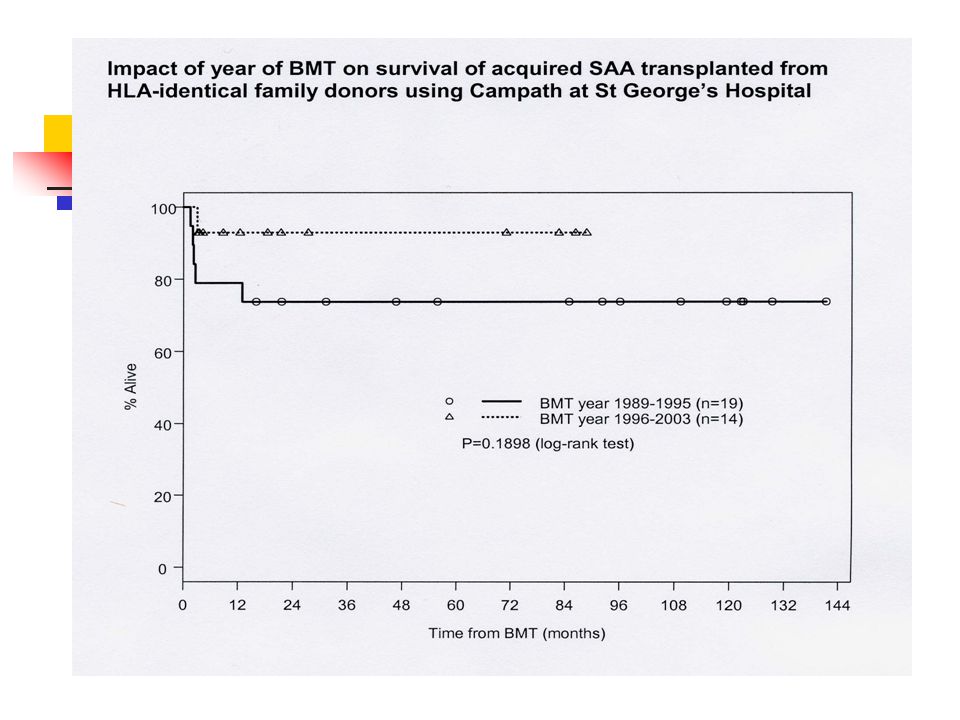
Favorable effect on acute and chronic GVHD with cyclophosphamide and in vivo Anti-CD52 Monoclonal antibodies for marrow transplantation from HLA-identical sibling donors for acquired aplastic anaemia V. Gupta, S.Ball, Q-L Yi, D. Sage, S. McCann, M Lawler, M. Ortin, G Hale, H Waldmann, EC Gordon- Smith, J. Marsh (Biology of Blood and Marrow Transplant, 2004: 867-876)
.")
35
GVHD Acute (11%) Chronic (3%)
 Chronic (3%)")
36
Alemtuzumab for prevention of GVHD in AA The impact on acute and chronic GVHD was favorable However, graft rejection was 24% Important Lesson Graft rejection was higher in patients who received campath both prior and after stem cell infusion (36%) compared to those who received campath only prior to stem cell infusion (16%)
 compared to those who received campath only prior to stem cell infusion (16%)")
37
Alemtuzumab for prevention of GVHD in AA Therefore, timing and dose of anti- CD52 MoAb is important At PMH, second generation protocols for Campath antibodies were designed and initiated in October 2004 Day –810 mg Day –720 mg Day –630 mg

38
Traditional GVHD prophylaxis (CSA+MTX) 2000-2004 N=14 Campath based GVHD prophylaxis 2005-2006 N=10 P value Median age of patients (range) 38 (20-59)40 (25-56)NS Stage of disease New Diagnosis Relapsed/Ref. 11(79%) 3(21%) 5(50%) NS Type of donor MSD/MFD AD 12 (86%) 2 (14%) 8(80%) 2(20%) NS AA patients receiving alemtuzumab based protocols at PMH
 3(21%) 5(50%) NS Type of donor MSD/MFD AD 12 (86%) 2 (14%) 8(80%) 2(20%) NS AA patients receiving alemtuzumab based protocols at PMH.")
39
OutcomesTraditional GVHD prophylaxis (CSA+MTX) N=14 Campath based GVHD prophylaxis N=10 P value Graft Failure3(21%)1(10%)NS Had 2 nd BMT2(14%)0NS Acute GVHD (II-IV)9/14(64%)1/9(11%)0.03 Chronic GVHD7/9(78%)00.002 Serious GVHD8/14(66%)00.007
 N=14 Campath based GVHD prophylaxis N=10 P value Graft Failure3(21%)1(10%)NS Had 2 nd BMT2(14%)0NS Acute GVHD (II-IV)9/14(64%)1/9(11%)0.03 Chronic GVHD7/9(78%) Serious GVHD8/14(66%)00.007")
40
AA patients receiving alemtuzumab based protocols at PMH Infectious complications Increased CMV reactivation in the campath patients (p=0.008) Other infections do not appear to be increased
 Other infections do not appear to be increased")
41
What is the current role of unrelated donor BMT ?

42
International BMT Registry (IBMTR)
")
43
Unrelated donor tx for AA (Deeg et al. Blood 2006)
")
44
Low-Dose Cyclophosphamide, Fludarabine and ATG as preparative regimen for aplastic anaemia from alternative donors (Bacigalupo et al, BMT, 2005)
")
45
Treatment strategies for newly diagnosed patient with Severe Aplastic Anaemia (Gupta and Marsh, In Press, 2007) Age of patient 40yr > 40 yr HLA identical sibling YesNo Response at 4 months YesNo Response at 4 months YesNo MUD available No Yes Adequate performance status Adequate performance status Yes NoYes MUD BMT Supportive therapy Options 1. 3 rd ATG if previous response to ATG 2. CRP using novel IST 3. BMT using CRP with UCB HLA id sib BMT ATG (horse)+CSA 2 nd ATG (rabbit/horse) +CSA MUD BMT Supportive therapy Options Maintain on CSA while FBC rising, then very slow taper, often over one/more years 1. 3 rd ATG if previous response to ATG 2. CRP using novel IST 3. BMT using CRP with UCB / haplotransplantation
+CSA 2 nd ATG (rabbit/horse) +CSA MUD BMT Supportive therapy Options Maintain on CSA while FBC rising, then very slow taper, often over one/more years 1. 3 rd ATG if previous response to ATG 2. CRP using novel IST 3. BMT using CRP with UCB / haplotransplantation.")
46
Conclusions Survival has improved in young patients with AA treated with BMT and immunosuppressive therapy (IST) Improvements in supportive care such as new antimicrobials, anti-fungals and better transfusion practices have contributed to better outcome Quality of recovery is different between BMT and IST, need for prospective QOL studies
 Improvements in supportive care such as new antimicrobials, anti-fungals and better transfusion practices have contributed to better outcome Quality of recovery is different between BMT and IST, need for prospective QOL studies")
Similar presentations










 Masood Anwar. Bone marrow failure syndromes can be defined as a group of diseases in which occurs failure on the part of bone marrow to produce.>")










