Download presentation
Presentation is loading. Please wait.

1
Interventions for Clients with Hematologic Problems
WHITE BLOOD CELL DISORDERS

2
White blood cells (WBCs), or leukocytes, provide protection from invading non-self cells and cancer cells in several ways. These protective functions depend on maintaining normal numbers and ratios of many specific mature, circulating leukocytes. When any one type of WBC is present in either abnormally high or abnormally low amounts, hematopoietic function and immune function may be altered to some degree, placing clients at risk for specific complications

3
Differentiating characteristics of the four types of leukemia

4
LEUKEMIA Etiology ionizing radiation chemicals and drugs
marrow hypoplasia (slow functioning with less than the normal production rate of blood cells) environmental interactions genetic factors viral factors immunologic factors the interaction of these factors
 environmental interactions. genetic factors. viral factors. immunologic factors. the interaction of these factors.")
7
LEUKEMIA

8
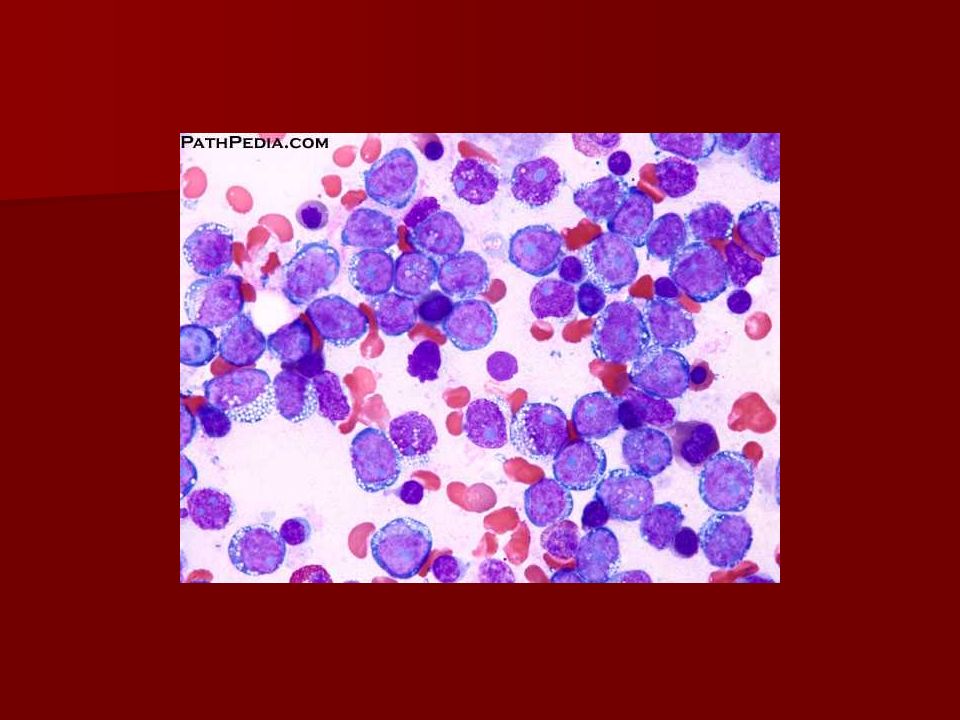
LEUKEMIA Laboratory assessment
decreased hemoglobin and hematocrit levels decreased platelet count altered white blood cell (WBC) count. The WBC count may be low, normal, or elevated but usually is quite elevated; counts of 20,000 to 100,000 are common. The client with a higher WBC count on diagnosis has a poorer prognosis The definitive test for leukemia includes various examinations of cells obtained from bone marrow aspiration and biopsy. The bone marrow is full of leukemic blast phase cells (immature cells that are dividing).
 count. The WBC count may be low, normal, or elevated but usually is quite elevated; counts of 20,000 to 100,000 are common. The client with a higher WBC count on diagnosis has a poorer prognosis. The definitive test for leukemia includes various examinations of cells obtained from bone marrow aspiration and biopsy. The bone marrow is full of leukemic blast phase cells (immature cells that are dividing).")
13
LEUKEMIA DRUG THERAPY FOR LEUKEMIA. Drug therapy for clients with AML is divided into three distinctive phases: induction, consolidation, and maintenance. Induction therapy. Induction therapy is intensive and consists of combination chemotherapy initiated at the time of diagnosis. This therapy is aimed at achieving a rapid, complete remission of all manifestations of disease. A typical course of aggressive chemotherapy includes IV administration of cytosine arabinoside for 7 days with concomitant administration of daunorubicin for the first 3 days. A major side effect of these agents is severe bone marrow suppression. As a result, the client becomes even more vulnerable to infection than before the treatment started. Prolonged hospitalizations are common while the client is immunosuppressed. Recovery of bone marrow function requires at least 2 to 3 weeks, during which time the client must be protected from life-threatening infections. Other adverse reactions include nausea, vomiting, diarrhea, alopecia (hair loss), stomatitis (mouth sores), kidney toxicity, liver toxicity, and cardiac toxicity.
, stomatitis (mouth sores), kidney toxicity, liver toxicity, and cardiac toxicity.")
14
LEUKEMIA Consolidation therapy. Consolidation therapy usually consists of another course of either the same agents used for induction at a different dosage or a different combination of chemotherapeutic agents. This treatment occurs early in remission, and its intent is to cure. At some institutions, consolidation therapy is a single course of chemotherapy; at others, it involves regularly scheduled, repeated courses of chemotherapy for 1 to 2 years. Maintenance therapy. Maintenance therapy may be prescribed for months to years after successful induction and consolidation therapies. It is commonly indicated for clients with acute lymphocytic leukemia (ALL). The purpose is to maintain the remission achieved through induction and consolidation. Maintenance agents are milder and are often given orally for 2 to 5 years.
. The purpose is to maintain the remission achieved through induction and consolidation. Maintenance agents are milder and are often given orally for 2 to 5 years.")
17
LEUKEMIA DRUG THERAPY FOR INFECTION. Drug therapy is the primary defense against infections that develop in clients undergoing therapy for AML. Agents used depend on the sensitivity of the specific organism causing the infection, as well as the extent of the infection, and are categorized by specificity as antibacterial, antiviral, or antifungal.

19
LEUKEMIA INFECTION PROTECTION SKIN CARE RESPIRATORY CARE
BONE MARROW TRANSPLANTATION

21
LEUKEMIA Sources of stem cells. BMT originated with the use of allogeneic bone marrow transplantation (transplantation of identical bone marrow from a sibling) and has advanced to the use of human leukocyte antigen (HLA)-matched stem cells from the umbilical cords of unrelated donors. Transplants can be classified based on the source of stem cells. In autologous transplants, the clients receive their own stem cells, which were collected before therapy. Syngeneic transplants are rare and involve the client's own identical twin as the donor of stem cells. In allogeneic transplants, a closely HLA-matched sibling or an unrelated donor provides the stem cells. Stem cells for transplantation may be obtained by one of the following methods: bone marrow harvest, peripheral stem cell pheresis, or umbilical cord blood stem cell Transplantation procedures have five phases: stem cell procurement, conditioning regimen, transplantation, engraftment, and posttransplantation recovery
 and has advanced to the use of human leukocyte antigen (HLA)-matched stem cells from the umbilical cords of unrelated donors. Transplants can be classified based on the source of stem cells. In autologous transplants, the clients receive their own stem cells, which were collected before therapy. Syngeneic transplants are rare and involve the client s own identical twin as the donor of stem cells. In allogeneic transplants, a closely HLA-matched sibling or an unrelated donor provides the stem cells. Stem cells for transplantation may be obtained by one of the following methods: bone marrow harvest, peripheral stem cell pheresis, or umbilical cord blood stem cell. Transplantation procedures have five phases: stem cell procurement, conditioning regimen, transplantation, engraftment, and posttransplantation recovery.")
24
Timing and steps of allogenic bone marrow transplantation

25
LEUKEMIA HEALTH TEACHING
The client and the family need to be educated about the importance of continuing therapy and appropriate medical follow-up, despite the unpleasant side effects of therapy. Many clients go home with a central venous catheter in place and require instructions about its care and maintenance. These guidelines may be altered depending on the home setting, assistance available, and agency policy

27
LEUKEMIA Protecting the client from infection after discharge from the hospital is just as important as it was during hospitalization. The nurse urges the client to use proper hygiene and to avoid crowds or others with infections. Neither the client nor any household member should receive live virus immunization (poliomyelitis, measles, or rubella) for 2 years after transplantation. The client should continue mouth care regimens at home. The nurse emphasizes that the client should immediately notify the physician if he or she experiences fever or any other sign of infection.
 for 2 years after transplantation. The client should continue mouth care regimens at home. The nurse emphasizes that the client should immediately notify the physician if he or she experiences fever or any other sign of infection.")
29
LEUKEMIA Because platelet recovery is usually slower than recovery of white blood cells (WBCs), many clients return home still at risk for bleeding. Thrombocytopenia may be present for 6 months following transplantation. The nurse reinforces the safety and bleeding precautions initiated in the hospital, emphasizing that the client must follow these precautions until the platelet count is above 50,000. The client and family are instructed to assess for petechiae, avoid trauma and sharp objects, apply pressure to wounds for 10 minutes, and report any unusual symptoms, including blood in the stool or urine, or headache that does not respond to acetaminophen.

31
MALIGNANT LYMPHOMA Malignant lymphomas occur as a result of abnormal overgrowth of one type of leukocyte (lymphocytes); they differ from the leukemias in the degree of maturation of the affected cells and the location of cell production. Lymphomas are malignancies characterized by a proliferation of committed lymphocytes rather than stem cell precursors (as in leukemia). This proliferation occurs not in bone marrow but in other lymphoid tissues scattered throughout the body, especially the lymph nodes and spleen. Lymphomas are actually solid tumors rather than cellular suspensions within the blood and bone marrow, and they fall into two major categories among adults: Hodgkin's lymphoma and non-Hodgkin's lymphoma
; they differ from the leukemias in the degree of maturation of the affected cells and the location of cell production. Lymphomas are malignancies characterized by a proliferation of committed lymphocytes rather than stem cell precursors (as in leukemia). This proliferation occurs not in bone marrow but in other lymphoid tissues scattered throughout the body, especially the lymph nodes and spleen. Lymphomas are actually solid tumors rather than cellular suspensions within the blood and bone marrow, and they fall into two major categories among adults: Hodgkin s lymphoma and non-Hodgkin s lymphoma.")
33
Hodgkin's Lymphoma Hodgkin's lymphoma is a cancer that can affect any age group, although incidence peaks first in people in their mid-to-late 20s and then in people older than 50 years of age. Men and women are affected equally in the first group, but the disease is more prevalent in men in the older group. Factors implicated as possible causes of Hodgkin's lymphoma include viral infections and previous exposure to alkylating chemical agents. This cancer usually originates in a single lymph node or a single chain of nodes. The lymphoid tissues within the node undergo malignant transformation, usually initiating some inflammatory processes. These nodes contain a specific transformed cell type, the Reed-Sternberg cell, a marker for Hodgkin's lymphoma. The disease first metastasizes (spreads) to other nearby lymphoid structures and eventually invades nonlymphoid tissues
 to other nearby lymphoid structures and eventually invades nonlymphoid tissues.")
34
Hodgkin's Lymphoma Assessment
Assessment most often reveals a greatly enlarged but painless lymph node or nodes, usually the earliest manifestation of Hodgkin's lymphoma. The client also often experiences fever, malaise, and night sweats. More specific clinical manifestations depend on the site (or sites) of malignancy and the extent of disease. Diagnosis and grade are established when biopsy of a node or mass reveals Reed-Sternberg cells. The client then undergoes extensive staging procedures to determine the exact extent of disease. Staging must be detailed and accurate because the treatment regimen is determined by the extent of disease. Staging procedures for Hodgkin's lymphoma include biopsies of distant lymph nodes, computed tomography (CT) of the thorax and abdomen, staging laparotomy, a complete blood count (CBC), liver function studies, and bilateral bone marrow biopsies
 of malignancy and the extent of disease. Diagnosis and grade are established when biopsy of a node or mass reveals Reed-Sternberg cells. The client then undergoes extensive staging procedures to determine the exact extent of disease. Staging must be detailed and accurate because the treatment regimen is determined by the extent of disease. Staging procedures for Hodgkin s lymphoma include biopsies of distant lymph nodes, computed tomography (CT) of the thorax and abdomen, staging laparotomy, a complete blood count (CBC), liver function studies, and bilateral bone marrow biopsies.")
36
Manifestations and staging criteria for Hodgkin's lymphoma

37
Hodgkin's Lymphoma Interventions
Hodgkin's lymphoma is now one of the most curable types of cancer. Generally, for stage I and stage II disease without mediastinal node involvement, the treatment of choice is extensive external radiation of involved lymph node regions. With more extensive disease, radiation coupled with an aggressive multiagent chemotherapy regimen is most effective in achieving a cure

38
Non-Hodgkin's Lymphoma
Non-Hodgkin's lymphoma is the classification for all cancers originating from lymphoid tissues that are not diagnosed as Hodgkin's lymphoma. There are more than 12 subtypes of non-Hodgkin's lymphoma, including low-grade, intermediate, and high-grade lymphomas. The low-grade lymphomas usually arise from B-cell lymphocytes and progress slowly. Although clients with low-grade lymphomas have longer survival rates, the diseases are less responsive to treatment and, consequently, cures are rare. At the other end of the spectrum are the high-grade lymphomas, which are aggressive tumors of usually mixed cellularity with rapid doubling times. High-grade lymphomas are more responsive to chemotherapy, and the chances for a longterm cure are greater. Most non-Hodgkin's lymphomas arise from lymph nodes, but they can originate in virtually any tissue or organ. A low-grade lymphoma also can convert to a higher-grade lymphoma. Definitive causes are unknown, but viral infection, exposure to ionizing radiation, autoimmune disorders, and exposure to toxic chemicals have all been implicated

40
Non-Hodgkin's Lymphoma
Because lymphomas may arise from lymphoid cells in any tissue and because the malignancy can spread to any organ, assessment reveals no specific clinical manifestations other than lymphadenopathy common to all types of lymphoma. Diagnosis is made from the histologic features apparent on biopsy of any suspicious node or mass. Classification of the specific lymphoma subtype is based on a complex grading of surface markers, cytogenetic features, cell size, and expression of viral antigens. Staging is similar to that for Hodgkin's lymphoma. Treatment consists of radiation therapy and multiagent chemotherapy. Nursing care needs are similar to those for clients with Hodgkin's lymphoma, with additional organ-specific problems taken into account if the disease is widely disseminated

Similar presentations















1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")



 CHEMOTHERAPY Adult Medical-Surgical Nursing.>")







>")


:>")



