Download presentation
Presentation is loading. Please wait.

2
DIZZINESS History Dizziness Vertigo INNER EAR Single episode Multiple episodes Disequilibrium Presyncope Other Spinning History of 1 st episode Predisposing factors Associated symptoms How long? Single or recurrent

3
able: Summary of typical clinical features of common causes of vertigo OnsetDurationPrecipita nts Associati ons Vestibula r neuroniti s (neuritis) SuddenConstant for many hours or even a day Viral illness (occasion ally) Nausea and vomiting BPPVIntermitt ent Episodes up to 60 seconds Head moveme nts None Ménière' s disease Intermitt ent Unpredic table, episodes may last hours -Deafness Tinnitus Aural fullness Recurren t vestibulo pathy Intermitt ent Episodes lasting minutes to hours -- able: Summary of typical clinical features of common causes of vertigo OnsetDurationPrecipitantsAssociations Vestibular neuronitis (neuritis) SuddenConstant for many hours or even a day Viral illness (occasionally) Nausea and vomiting BPPVIntermittentEpisodes up to 60 seconds Head movements None Ménière's disease IntermittentUnpredictable, episodes may last hours -Deafness Tinnitus Aural fullness Recurrent vestibulopathy IntermittentEpisodes lasting minutes to hours --
 SuddenConstant for many hours or even a day Viral illness (occasion ally) Nausea and vomiting BPPVIntermitt ent Episodes up to 60 seconds Head moveme nts None Ménière s disease Intermitt ent Unpredic table, episodes may last hours -Deafness Tinnitus Aural fullness Recurren t vestibulo pathy Intermitt ent Episodes lasting minutes to hours -- able: Summary of typical clinical features of common causes of vertigo OnsetDurationPrecipitantsAssociations Vestibular neuronitis (neuritis) SuddenConstant for many hours or even a day Viral illness (occasionally) Nausea and vomiting BPPVIntermittentEpisodes up to 60 seconds Head movements None Ménière s disease IntermittentUnpredictable, episodes may last hours -Deafness Tinnitus Aural fullness Recurrent vestibulopathy IntermittentEpisodes lasting minutes to hours --")
4
Homework Chondrodermatitis nodularis chronica helicis Hallpike test Epley’s manouver

5
The Nose

6
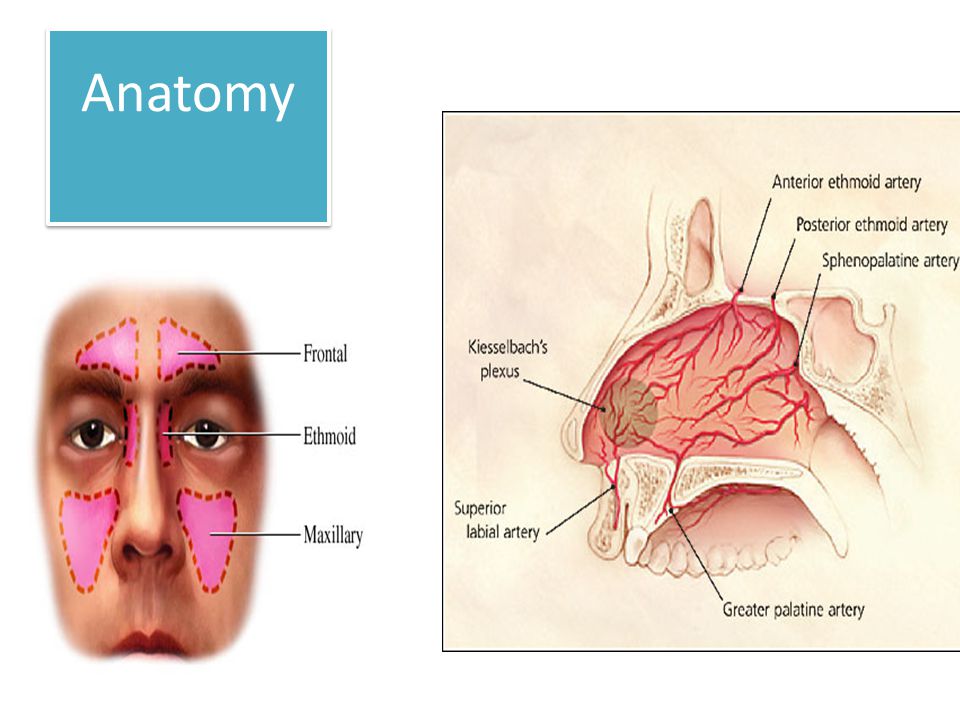
Anatomy

8
# nasal bones

10
Epistaxis

12
Septal perforation

13
Trauma,iatrogenig,Wegner’s,sarcoidosis,TB,Syphilis, COCAINE,NEOPLASTIC. Asynptomatic, wistling,blockage,epistaxis FBC,ESR,CANCA,ACE level?VDRL.Biopsy Saline nasal douches,surgical

15
Rhinitis 2 out of 3 for >1 hour every day for >2 weeks. -Nasal congestion -rhinorrhoea (Ant. Or Post.) -sneezing - itching (nasal cavity),facial pain,anosmia *RAST *steroides (beclomethazone,fluticasone,mometasone) *Antihistaminics *Oral steroides *Montelukast *saline douches *surgical NB Rhinits and sinusits usually coexist and are concurrent in most individuals; thus, the correct terminology is now rhinosinusits.
 -sneezing - itching (nasal cavity),facial pain,anosmia *RAST *steroides (beclomethazone,fluticasone,mometasone) *Antihistaminics *Oral steroides *Montelukast *saline douches *surgical NB Rhinits and sinusits usually coexist and are concurrent in most individuals; thus, the correct terminology is now rhinosinusits..")
16
Sinusitis Acute:<4 weeks 1-Broad spectrum antibiotics 2-Betnesol nasal drops(2 drops BD) 3-Steam inhalation 4-Xylometazoline 0.5% 2 drops tds Chronic >12 weeks RAST,ESR,CANCA,ACE,CT scan Sinuses Medical treatment for 3 months mild :fluticasone 2 puffs OD Severe (polyps) :Betamethasone 2 drops for 6 weeks followed by steroides spray Oral antihistaminics (if allergic) Oral steroids (very severe) Oral antibiotics (clarythromycin) Surgical: FESS Referral: failure of treatment red flags patient willing to have surgery.
 3-Steam inhalation 4-Xylometazoline 0.5% 2 drops tds Chronic >12 weeks RAST,ESR,CANCA,ACE,CT scan Sinuses Medical treatment for 3 months mild :fluticasone 2 puffs OD Severe (polyps) :Betamethasone 2 drops for 6 weeks followed by steroides spray Oral antihistaminics (if allergic) Oral steroids (very severe) Oral antibiotics (clarythromycin) Surgical: FESS Referral: failure of treatment red flags patient willing to have surgery.")
17
Periorbital cellulitis

18
Nasal polyps What are they? Paediatric polyps? ?Unilateral polyps?( neoplastic until proven otherwise) Associated with Asthma (particularly late-onset asthma) Aspirin sensitivity.......... Samter's triad infective sinusitis cystic fibrosis Kartagener's syndrome Churg-Strauss syndrome all patients with suspected nasal polyps should be referred to ENT for a full examination topical corticosteroids shrink polyp size in around 80% of patients Around in 1% of adults in the UK have nasal polyps. They are around 2-4 times more common in men and are not commonly seen in children or the elderly.
 Associated with Asthma (particularly late-onset asthma) Aspirin sensitivity Samter s triad infective sinusitis cystic fibrosis Kartagener s syndrome Churg-Strauss syndrome all patients with suspected nasal polyps should be referred to ENT for a full examination topical corticosteroids shrink polyp size in around 80% of patients Around in 1% of adults in the UK have nasal polyps. They are around 2-4 times more common in men and are not commonly seen in children or the elderly..")
21
Red flags Unilateral blockage Unilateral discharge Blood stained discharge Eye signs /symptoms Facial swelling (smokers, elderly)
")
22
SNORING Causes Epworth sore...?sleep apnoea(is it witnessed) Day time somnolesence Treatment Wight loss Surgical UVPPP CPAP DLVA Patient’s responsibility to inform DVLA when OSA suspected/investigated. Doctors responsibility to inform DVLA if untreated OSA pt is witnessed driving

24
Homework CSF rhinorrhoea

25
Throat

26
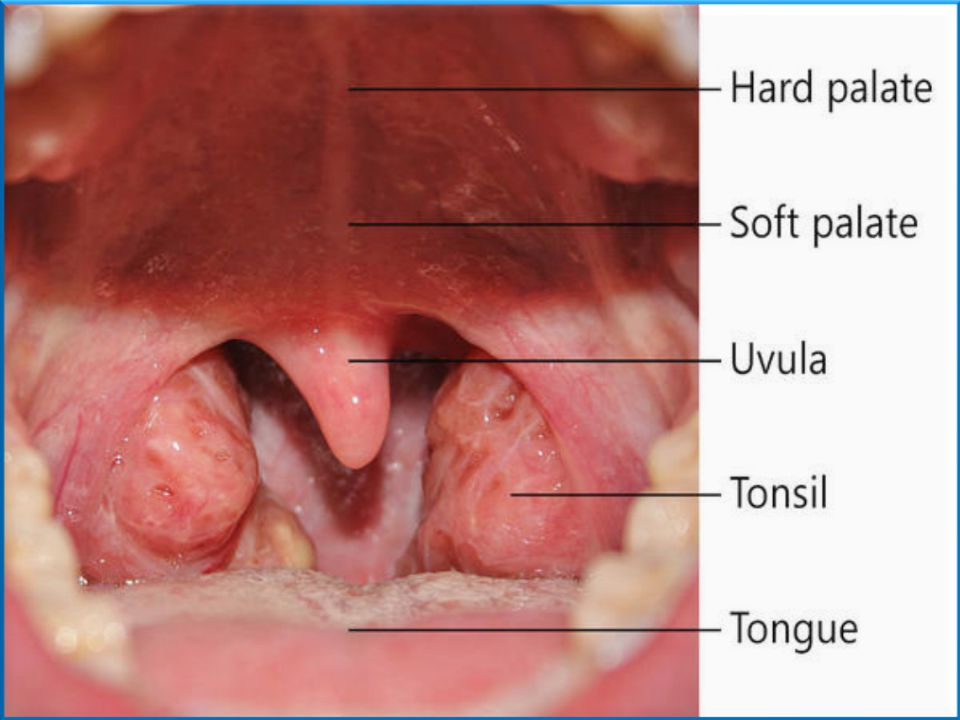
Anatomy

29
Acute tonsillitis

30
NICE indications for antibiotics features of marked systemic upset secondary to the acute sore throat unilateral peritonsillitis a history of rheumatic fever an increased risk from acute infection (such as a child with diabetes mellitus or immunodeficiency) patients with acute sore throat/acute pharyngitis/acute tonsillitis when 3 or more Centor criteria are present WHICH ANTIBIOTICS? Presence of tonsillar exudate Tender anterior cervical lymphadenopathy or lymphadenitis History of fever Absence of cough Presence of tonsillar exudate Tender anterior cervical lymphadenopathy or lymphadenitis History of fever Absence of cough

31
Quinsy

33
Glandular fever

37
Laryngology

38
Hoarseness Causes: URTI (Most common) Trauma(shouting/nodules). Iatrogenic tumour neurological (?) functional(young women) Ask about ? Reflux symptoms, Wight loss, inhalers use, voice misuse, stress,swallowing, breathing Investigations :TFT,weight,indirect laryngoscopoy. Urgent Chest XRAY (IF SYMPTOMS >3 WEEKS) If X-ray shows positive signs..urgent referral to chest physician If X-ray shows negative signs..urgent referral to ENT Early laryngeal tumours confined to vocal cords have 80-90% 5 Y survival.
 functional(young women) Ask about . Reflux symptoms, Wight loss, inhalers use, voice misuse, stress,swallowing, breathing Investigations :TFT,weight,indirect laryngoscopoy. Urgent Chest XRAY (IF SYMPTOMS >3 WEEKS) If X-ray shows positive signs..urgent referral to chest physician If X-ray shows negative signs..urgent referral to ENT Early laryngeal tumours confined to vocal cords have 80-90% 5 Y survival..")
39
2WW Red flags Persistent hoarseness > 3 weeks Pain Dysphagia Haemoptysis Otalgia Neck lump Especially in - smokers - over 40yrs

40
Croup versus epiglottitis FeaturesCROUPEpiglottitis OrganismPara influanze virusH Influanza Age< 2 years2-6 Onsetgradualrapid Previous attackoftenno CoughParkingno DysphagiaNO+++ stridorinspiratoryInsp/expiratory Pyrexia+++ positionLying DownSitting forward droolingNo+++ nodes++++ behaviorstrugglingQuiet voicehoarsemuffled colourpinkgrey

41
Neck lumps Lymphadenopathy Branchial cyst Thyroglossal cyst Salivary glands Refer urgently to ENT

42
Urgent referral Mouth ulcers> 3weeks. Lumps in mouth >3 weeks Ubexplained sore throat>1 month Hoarseness >3 weeks, negative CXR. Unexplained salivary gland swelling>4 weeks Unilateral unexplained ear ache with normal otoscopy Asymmetrical /unilateral deafness Unilateral tinnitus

44
The ear http://www.youtube.com/watch?feature=play er_embedded&v=0kEKoQ33dB0

Similar presentations














 Lawrence Pike.>")

















