Download presentation
Presentation is loading. Please wait.

2
Slide No. 9: (2 Marks) A 15 years female complaining of delayed menarche: Findings (A) Inspection of abdomen (B) Inspection of vulva Most Probable Diagnosis: Imperforate Hymen Most Probable Diagnosis: Imperforate Hymen Treatment: Hymenectomy or Hymontomy Treatment: Hymenectomy or Hymontomy
 A 15 years female complaining of delayed menarche: Findings (A) Inspection of abdomen (B) Inspection of vulva Most Probable Diagnosis: Imperforate Hymen Most Probable Diagnosis: Imperforate Hymen Treatment: Hymenectomy or Hymontomy Treatment: Hymenectomy or Hymontomy.")
3
Slide No. 5: (2 Marks) Before surgery During surgery What is your diagnosis? Imperforate Hymen The most serious complication of this operation: Infection A 16-years girl with delayed menarche

5
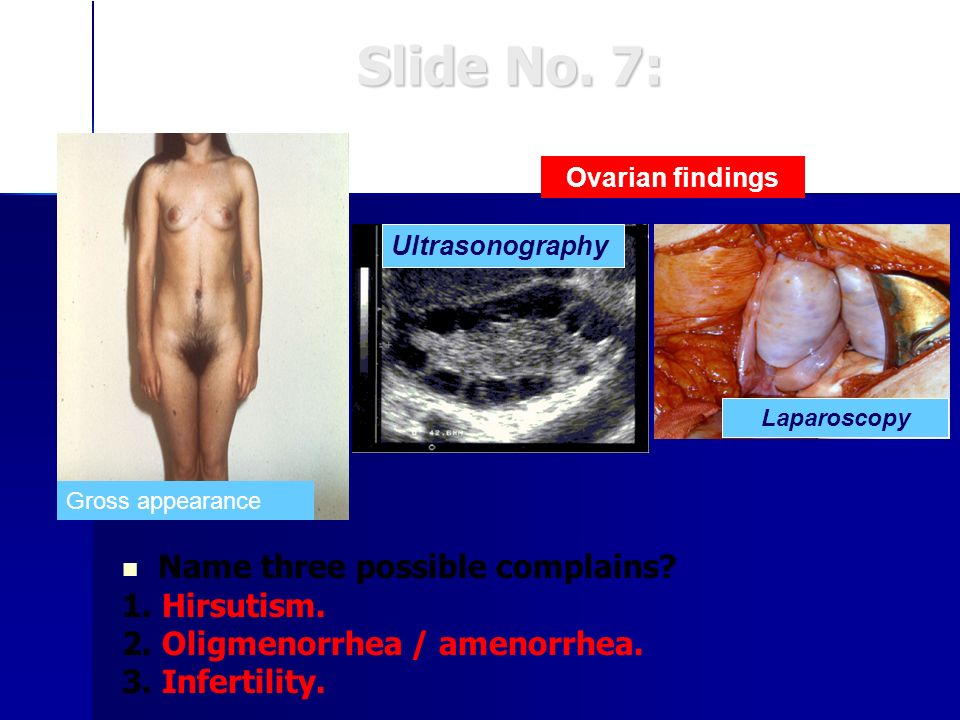
Slide No. 7: Name three possible complains? 1. Hirsutism. 2. Oligmenorrhea / amenorrhea. 3. Infertility. Laparoscopy Ultrasonography Ovarian findings Gross appearance

8
SLIDE 1

9
SLIDE 2

10
SLIDE 9 UTERU S

11
Local Examination During surgery Ultrasonography Abdominal Examination

13
Imperforate hymen

14
15% of 1ry amenorrhea 15% of 1ry amenorrhea Normal breasts and Sexual Hair development & Normal looking external female genitalia Normal breasts and Sexual Hair development & Normal looking external female genitalia Normal female range testosterone level Normal female range testosterone level Absent uterus and upper vagina & Normal ovaries Absent uterus and upper vagina & Normal ovaries Karyotype 46-XX Karyotype 46-XX 30% renal,10% skeletal and middle ear anomalies 30% renal,10% skeletal and middle ear anomalies Treatment : STERILE ? Vaginal creation(Dilatation VS Vagino- plasty) Treatment : STERILE ? Vaginal creation(Dilatation VS Vagino- plasty)
 Treatment : STERILE . Vaginal creation(Dilatation VS Vagino- plasty).")
15
X-linked recessive gene. X-linked recessive gene. Absent cytosol receptors Absent cytosol receptors Normal breasts but no sexual hair Normal breasts but no sexual hair Normal looking female external genitalia Normal looking female external genitalia Absent uterus and upper vagina Absent uterus and upper vagina Karyotype 46, XY Karyotype 46, XY Male range testosterone level Male range testosterone level Treatment : gonadectomy after puberty + HRT Treatment : gonadectomy after puberty + HRT ? Vaginal creation (dilatation VS Vaginoplasty ) ? Vaginal creation (dilatation VS Vaginoplasty )
 . Vaginal creation (dilatation VS Vaginoplasty ).")
18
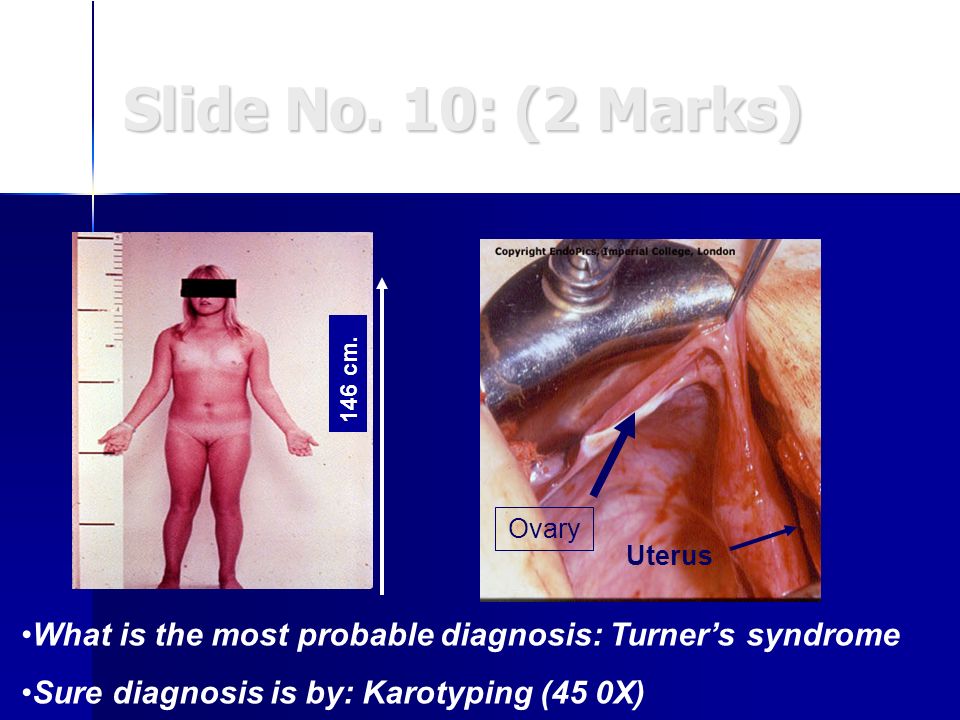
Slide No. 10: (2 Marks) A 18-years girl with primary amenorrhea Ovary Uterus 146 cm. What is the most probable diagnosis: Turners syndrome Sure diagnosis is by: Karotyping (45 0X)
.")
19
Mosaic (46-XX / 45-XO)(Classic 45-XO) Turners syndrome
(Classic 45-XO) Turners syndrome")
20
Ovarian dysgenesis

21
FSH Serum level Low / normalHigh Hypogonadotropic hypogonadim Gonadal dysgenesis

22
Normal hight Normal hight Normal external and internal genital organs (infantile) Normal external and internal genital organs (infantile) Low FSH and LH Low FSH and LH MRI to R/O intra-cranial pathology. MRI to R/O intra-cranial pathology. 30-40% anosmia (kallmanns syndrome) 30-40% anosmia (kallmanns syndrome) Sometimes constitutional delay Sometimes constitutional delay Treat according to the cause (HRT), potentially fertile. Treat according to the cause (HRT), potentially fertile.
 30-40% anosmia (kallmanns syndrome) Sometimes constitutional delay Sometimes constitutional delay Treat according to the cause (HRT), potentially fertile. Treat according to the cause (HRT), potentially fertile..")
24
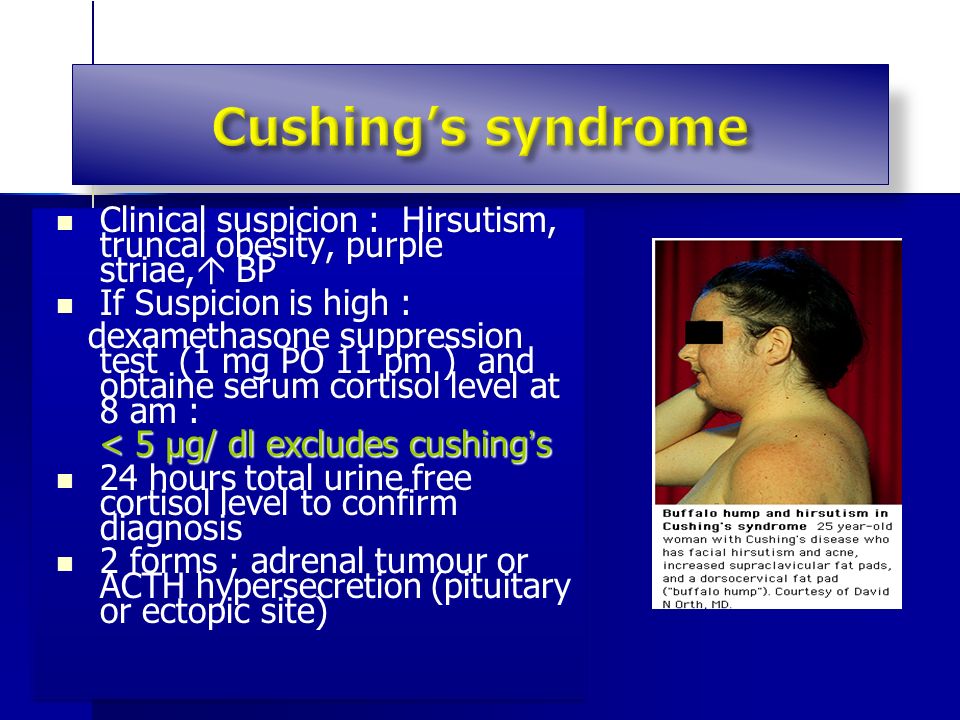
Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP If Suspicion is high : If Suspicion is high : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : < 5 µ g/ dl excludes cushing s < 5 µ g/ dl excludes cushing s 24 hours total urine free cortisol level to confirm diagnosis 24 hours total urine free cortisol level to confirm diagnosis 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP If Suspicion is high : If Suspicion is high : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : < 5 µ g/ dl excludes cushing s < 5 µ g/ dl excludes cushing s 24 hours total urine free cortisol level to confirm diagnosis 24 hours total urine free cortisol level to confirm diagnosis 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site)
 and obtaine serum cortisol level at 8 am : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : < 5 µ g/ dl excludes cushing s < 5 µ g/ dl excludes cushing s 24 hours total urine free cortisol level to confirm diagnosis 24 hours total urine free cortisol level to confirm diagnosis 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP Clinical suspicion : Hirsutism, truncal obesity, purple striae, BP If Suspicion is high : If Suspicion is high : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : dexamethasone suppression test (1 mg PO 11 pm ) and obtaine serum cortisol level at 8 am : < 5 µ g/ dl excludes cushing s < 5 µ g/ dl excludes cushing s 24 hours total urine free cortisol level to confirm diagnosis 24 hours total urine free cortisol level to confirm diagnosis 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site) 2 forms ; adrenal tumour or ACTH hypersecretion (pituitary or ectopic site)")
25
1 o or 2 o Amenorrhea is often first sign 1 o or 2 o Amenorrhea is often first sign A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea Hypothalamic suppression Hypothalamic suppression Abnormal body image, intense fear of weight gain, often strenuous exercise Abnormal body image, intense fear of weight gain, often strenuous exercise Mean age onset 13-14 yrs (range 10-21 yrs) Mean age onset 13-14 yrs (range 10-21 yrs) Low estradiol risk of osteoporosis Low estradiol risk of osteoporosis Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Treatment : body wt. (Psychiatrist referral) Treatment : body wt. (Psychiatrist referral) 1 o or 2 o Amenorrhea is often first sign 1 o or 2 o Amenorrhea is often first sign A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea Hypothalamic suppression Hypothalamic suppression Abnormal body image, intense fear of weight gain, often strenuous exercise Abnormal body image, intense fear of weight gain, often strenuous exercise Mean age onset 13-14 yrs (range 10-21 yrs) Mean age onset 13-14 yrs (range 10-21 yrs) Low estradiol risk of osteoporosis Low estradiol risk of osteoporosis Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Treatment : body wt. (Psychiatrist referral) Treatment : body wt. (Psychiatrist referral)
 can cause menstrual irregularity. Treatment : body wt. (Psychiatrist referral) Treatment : body wt. (Psychiatrist referral) 1 o or 2 o Amenorrhea is often first sign 1 o or 2 o Amenorrhea is often first sign A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea A body mass index (BMI) <17 kg/m ² menstrual irregularity and amenorrhea Hypothalamic suppression Hypothalamic suppression Abnormal body image, intense fear of weight gain, often strenuous exercise Abnormal body image, intense fear of weight gain, often strenuous exercise Mean age onset yrs (range yrs) Mean age onset yrs (range yrs) Low estradiol risk of osteoporosis Low estradiol risk of osteoporosis Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Bulemics less commonly have amenorrhea due to fluctuations in body wt, but any disordered eating pattern (crash diets) can cause menstrual irregularity. Treatment : body wt. (Psychiatrist referral) Treatment : body wt. (Psychiatrist referral).")
26
Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Eating disorders have a higher prevalence in female athletes than non-athletes Eating disorders have a higher prevalence in female athletes than non-athletes Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Eating disorders have a higher prevalence in female athletes than non-athletes Eating disorders have a higher prevalence in female athletes than non-athletes Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels
 Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Eating disorders have a higher prevalence in female athletes than non-athletes Eating disorders have a higher prevalence in female athletes than non-athletes Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Common in women who participate in sports (e.g. competitive athletes, ballet dancers) Eating disorders have a higher prevalence in female athletes than non-athletes Eating disorders have a higher prevalence in female athletes than non-athletes Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels Hypothalamic disorder caused by abnormal gonadotrophin-releasing hormone pulsatility, resulting in impaired gonadotrophin levels, particularly LH, and subsequently low oestrogen levels.")
Similar presentations








 become male or female?>")











>")





 Professor of OB/GYN Qassim,College of Medicine Amenorrhea Salah Roshdy (MD) Professor of OB/GYN Qassim,College of Medicine.>")