Download presentation
Presentation is loading. Please wait.

1
Uti in children

2
Introduction Pediatric UTIs often signal an underlying genitourinary tract abnormality Can lead to renal scarring with resultant hypertension and renal failure Difficult to diagnose because symptoms are non-specific in this age group and testing is often invasive

3
Pediatric UTIs: Epidemiology
Prevalence Girls—6.5-8% Boys—2-3% Uncircumcised boys have a 5-20 X increase in UTIs vs circumcised boys Occurs in about 7% of children <2 who present with fever without a source

4
Epidemiology (continued)
Incidence of vesicoureteral reflux (VUR) is 1% in children < 2 yoa. 50% of kids <1 yoa with UTI have VUR Early renal scarring is nearly twice as common in this age group. Incidence of scarring increases with each subsequent UTI Scarring occurs in 5-38% of febrile UTI’s.
 is 1% in children < 2 yoa. 50% of kids <1 yoa with UTI have VUR. Early renal scarring is nearly twice as common in this age group. Incidence of scarring increases with each subsequent UTI. Scarring occurs in 5-38% of febrile UTI’s.")
5
Figure 1 Prevalence of VUR by age
Figure 1 Prevalence of VUR by age. Plotted are the prevalences reported in 54 studies of urinary tract infections in children (references in Technical Report). Pediatrics 1999; 103:
. Pediatrics 1999; 103:")
6
Figure 2 Relationship between renal scarring and number of urinary tract infections.16
Pediatrics 1999; 103:

7
UTI: Classiffication Classification: Upper tract infection
Acute pyelonephritis- fever, bacteriuria, systemic symptoms Lower tract infection Urethritis Cystitis Voiding symptoms, little or no fever, no systemic symptoms

8
Clinical Presentation
Age and gender dependent 0 - 2 months: Fever 2 mo.– 2 y/o: Fever (>38 C) Irritability Vomiting and Diarrhea Decrease appetite Between 1-2 y/o = crying on urination, foul smelling odor Females of all ages are more predisposed to UTI due to short urethra.Male urethra as an infant is also short. What is the rationale for why a febrile UTI is pyelo until proven otherwise?The kidney is a complex organ as opposed to the bladder as a hollow viscus. Inflammation of the parenchyma of the kidney is responsible for fever.
 Irritability. Vomiting and Diarrhea. Decrease appetite. Between 1-2 y/o = crying on urination, foul smelling odor. Females of all ages are more predisposed to UTI due to short urethra.Male urethra as an infant is also short. What is the rationale for why a febrile UTI is pyelo until proven otherwise The kidney is a complex organ as opposed to the bladder as a hollow viscus. Inflammation of the parenchyma of the kidney is responsible for fever.")
9
Clinical Presentation
2 y/o – 6 y/o: Systemic symptoms Fever Flank or back pain Urgency, urinary incontinence, dysuria Suprapubic or abdominal pain Foul smelling odor > 6 y/o and adolescents: Same as above

10
Urethritis In female infants In adolescent girls and boys
Part of a diaper dermatitis In adolescent girls and boys Presenting sign of STD In pre-school and school age girls Part of “non-specific” vulvovaginitis Generally environmental Bubble bath Nylon panties (also biker shorts, leotards, bathing suits) Poor hygiene (not wiping, wiping back to front) Overzealous hygiene Use of baby powder, perfumes
 Poor hygiene (not wiping, wiping back to front) Overzealous hygiene. Use of baby powder, perfumes.")
11
Symptoms of urethritis
Dysuria Reluctance to void Perineal discomfort, erythema May be associated with vaginal irritation and erythema in girls In older boys, urethral discharge In adolescent girls associated with PID symptoms Symptoms are difficult to elicit in younger children secondary to lack of vocabulary

12
Cystitis Afebrile usually Frequency Enuresis Dysuria
Reluctance to void

13
Pyelonephritis Usually associated with fever and systemic signs 2° renal parenchymal inflammation Older children Flank pain or abdominal pain Younger children Fever, irritability, vomiting, poor feeding

14
Pyelonephritis - Significance
EACH infection results in scar formation and reduced renal function After diabetes mellitus and collagen vascular disease, undetected renal disease and untreated childhood UTI may be responsible for: A large of portion of ESRD in adults A huge need for dialysis and transplantation It has been the assumption that renal scars are the RESULT of infection; could it also be that kidneys which are scarred or dysfunctional are at higher risk for infection? Is it an association or causality?

15
Pyelonephritis - Significance
Untreated childhood UTI responsible for: Hypertension Impaired kidney function Complications of pregnancy

16
Causes and course of UTI

17
Risk Factors Age <1 year Female gender Uncircumcised males
Constipation Voiding dysfunction Improper wiping Genitourinary abnormalities Vesicoureteral reflux Obstruction Colonization with virulent E. Coli

18
Signs and Symptoms – Children 2 months to 2 years
Fever—usually unexplained Vomiting and/or diarrhea Abdominal Pain Failure to thrive Malodorous urine Crying on urination

19
Signs and Symptoms – Children >2
Fever Vomiting and/or diarrhea Abdominal pain Malodorous urine Frequency and/or urgency Dysuria New incontinence

20
Summary Urinary tract infections are a common cause of fever without a source in children <2 and can lead to renal scarring, HTN or ESRD. Rapid treatment is essential. Symptoms are non-specific and thus a high level of suspicion is required Urine culture is required for diagnosis, and should be obtained by catheterization or SPA when child is ill or infection is suspected Treatment requires a 7-14d course of antibiotics Prophylactic abx are required after initial treatment All Children <2 require 2 imaging studies after initial UTI

21
References Committee on Quality Improvement, Subcommittee on Urinary Tract Infection. The diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics 1999; 103: Layton, KL. Diagnosis and Management of Pediatric Urinary Tract Infections. Clinics in Family Practice 2003; 5: 2 Chon DH, Frank CL, Shortliffe LM. Pediatric Urinary Tract Infections. Pediatric Clinics of North America 2001; 48: Linderd KA, Shortliffe LM. Evaluation and management of pediatric urinary tract infections. Urologic Clinics of North America 1999; 26: McCollough M, Sharieff G. Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed.2002; Acute Urinary Tract Infections Clinical Effective Committee. Evidence based clinical practice guideline for patients 6 years of age or less with a first time acute urinary tract infection. Cincinnati (OH): Children’s Hospital Medical Center 1999; 1-14
: Children’s Hospital Medical Center 1999;")
22
Patient groups Options Time horizon NHS perspective
long-term antibiotic treatment for preventing recurrent urinary tract infections (UTI) in children Patient groups Infants of 1 year Girls and boys Recurrent UTI (no abnormalities) Mild VUR (grade I and II) Options Long-term low dose antibiotics (Cochrane review) (Trimethoprim, Nitrofurantoin, Cotrimoxazole) Intermittent treatment of UTIs Time horizon 3 years of long-term antibiotics and follow-up to end stage renal disease NHS perspective
 in children. Patient groups. Infants of 1 year. Girls and boys. Recurrent UTI (no abnormalities) Mild VUR (grade I and II) Options. Long-term low dose antibiotics (Cochrane review) (Trimethoprim, Nitrofurantoin, Cotrimoxazole) Intermittent treatment of UTIs. Time horizon. 3 years of long-term antibiotics and follow-up to end stage renal disease. NHS perspective.")
23
Model Structure for UTI

24
The evidence Effectiveness Existing reviews (variable quality)
Meta analysis, Multiple parameter synthesis Probabilistic trial based model Natural history Epidemiological studies Pooled trial baselines Registry studies Clinical judgement Quality of life Published studies Survey Costs Published unit costs and dosage (BNF, PSSRU, CIPFA)
")
25
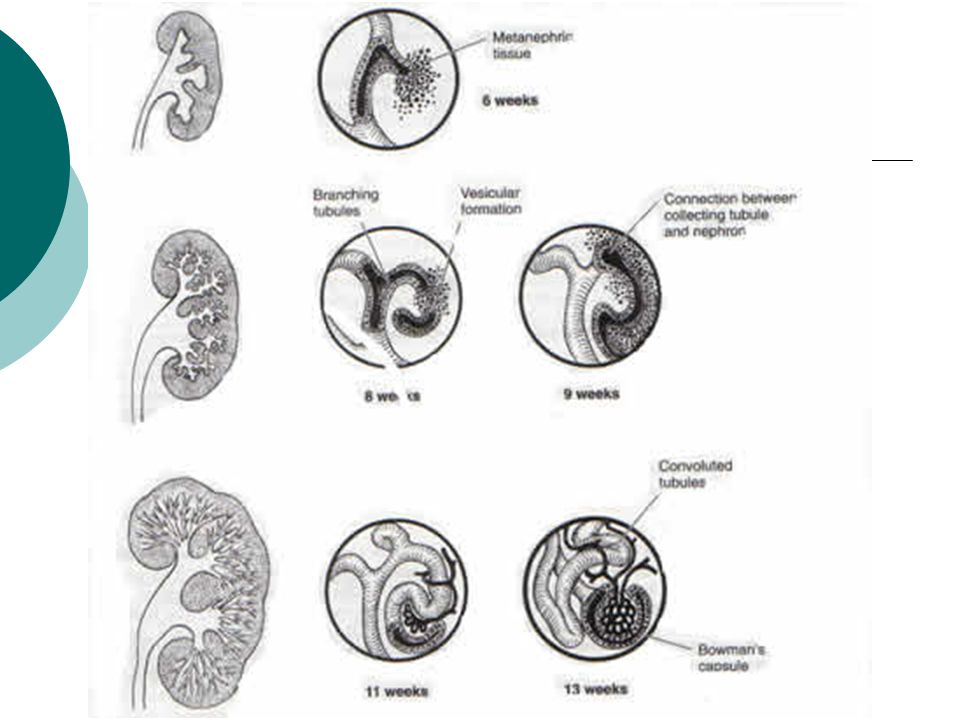
Antenatal Period The most common cause is physiologic dilation.
Metanephric urine production begins at 8 weeks, even before ureteral canalization is complete. Transient obstruction with hydronephrosis occurs.

26
Embryology

29
Pathophysiology: Anatomic and functional processes interrupts the flow of urine. There is a rise in ureteral pressure causing stretching and dilation; if pressures continue to rise, leads to decline in renal blood flow and GFR. When significant obstruction is persistent, it affects nephrogenic tissue and results in varying degrees of cystic dysplasia and renal impairment.

30
Grading of Severity of Hydronephrosis

31
Most Common Causes in Neonates:
Ureteropelvic Junction Obstruction Ureterovesical Junction Obstruction Posterior Urethral Valves Eagle-Barrett Syndrome (a.k.a. Prune Belly Syndrome) Vesicoureteral Reflux Ureterocele
 Vesicoureteral Reflux. Ureterocele.")
32
Treatment for UPJ: Pyeloplasty

33
Diagnosis

34
Urine Collection Clean Catch acceptable for toilet trained children (wearing underwear or pull-ups) Ensure cleansing with antiseptic towelette Catheterized specimen in diapered children Suprapubic bladder tap in <6 month old child is guaranteed sterile Frequently, the nursing staff will need to give explicit instructions to parent or patient or actually assist in urine collection

35
Leukocyte Esterase Has to accumulate in urine
Insufficient accumulation possible in small infants who void frequently Infants <3 months old may not have mature enough immune system to induce leukocytes in urine (beware neutropenia on CBC)
")
36
Nitrites By-products of E. coli and other lactose fermenters (glucose digestion) Insufficient accumulation possible in small infants who void frequently Insufficient accumulation possible in older child during the day and in older patient who has significant frequency If positive, highly suggestive of UTI (high specificity)
")
37
Microscopy >10 WBC/hpf on spun urine
Bacteria on unspun urine are common unless catheterized specimen Gram stain is very helpful on spun urine Standard UA plus gram stain is “enhanced UA” Usually reported as “5-20” or “<5”…so what to do if you are looking for >10??

38
Urine Culture >100,000 cfu per mL on any culture
>10,000 cfu per mL on cath specimen ANY bacterial growth on bladder tap (at least 1,000 cfu/mL)
")
39
Sensitivity and Specificity of
Components of the UA Sensitivity % (Range) Specificity % (Range) Test Leukocyte esterase Nitrite Leukocyte esterase or nitrite positive Microscopy: white blood cells Microscopy: bacteria Leukocyte esterase or nitrite or Microscopy positive 83 (67.94) 53 (15-82) 93 (90-100) 73 (32-100) 81 (16-99) 99.8 (99.100) 78 (64-92) 98 (90-100) 72 (58-91) 81 (45-98) 83 (11-100) 70 (60-92)
 Specificity % (Range) Test. Leukocyte esterase. Nitrite. Leukocyte esterase or nitrite positive. Microscopy: white blood cells. Microscopy: bacteria. Leukocyte esterase or nitrite or. Microscopy positive. 83 (67.94) 53 (15-82) 93 (90-100) 73 (32-100) 81 (16-99) 99.8 (99.100) 78 (64-92) 98 (90-100) 72 (58-91) 81 (45-98) 83 (11-100) 70 (60-92)")
40
Urine Cultures Held for 48 h but usually positive at 24 h for true UTI
Requires another day for ID of organism May require another day for sensitivities If contains skin flora (S. epi., S. aureus or α-strep.) considered contamination secondary to poor specimen collection
 considered contamination secondary to poor specimen collection.")
41
Diagnosis Urinalysis Can be obtained by most convenient means if infant is not ill UTI CANNOT be diagnosed with UA alone If suspicious UA, the Urine Culture must be obtained via SPA or catheter specimen If UA does not suggest UTI, it is reasonable to follow child clinically

42
Sensitivity % (Range) Specificity % (Range)
Table 1. Sensitivity and Specificity of Components of the Urinalysis, Alone and in Combination (References in Text) Test Sensitivity % (Range) Specificity % (Range) Leukocyte esterase 83 (67-94) 78 (64-92) Nitrite 53 (15-82) 98 (90-100) Leukocyte esterase or nitrite positive 93 (90-100) 72 (58-91) Microscopy: WBCs 73 (32-100) 81 (45-98) Microscopy: bacteria 81 (16-99) 83 (11-100) Leukocyte esterase or nitrite or microscopy positive 99.8 (99-100) 70 (60-92) Pediatrics 1999; 103:
 Test. Sensitivity % (Range) Specificity % (Range) Leukocyte esterase. 83 (67-94) 78 (64-92) Nitrite. 53 (15-82) 98 (90-100) Leukocyte esterase or nitrite positive. 93 (90-100) 72 (58-91) Microscopy: WBCs. 73 (32-100) 81 (45-98) Microscopy: bacteria. 81 (16-99) 83 (11-100) Leukocyte esterase or nitrite or microscopy positive (99-100) 70 (60-92) Pediatrics 1999; 103:")
43
Diagnosis Urine Culture MUST be collected via catheter or SPA
UTI CANNOT be diagnosed from a bag specimen Diagnosis of UTI requires Urine Culture LOE--Strong

44
Urine Collection: Suprapubic Aspirate
“Gold standard” - >99% specificity Positive culture: any number of g- bacilli or >3000 CFU of g+ cocci

45
Urine Collection: Transuretheral Catherization
>105 CFU - 95% specificity 104 – 105 CFU – infection is likely 103 – 104 CFU – Suspicious <103 CFU – infection unlikely

46
treatment

47
Treatment May initiate treatment either orally or parenterally
Admit and use parenteral antibiotics if toxic, dehydrated or unable to take PO Choices: TMP/SMX Cephalosporin Amoxicillin (check local resistance)
")
48
Treatment--continued
Improvement should be seen in hours If not having expected clinical response in 2 days, re-culture, consider changing antibiotics and do imaging studies Complete 7-14 day course of antibiotics 14 days should be given for those that were ill with clinical evidence of pyelonephritis

49
Prophylaxis After completion of initial antibiotics, children should be give a prophylactic dose of antibiotics until imaging studies complete Antibiotic should have high urinary excretion and low serum and fecal levels, thus minimizing the development of resistance.

50
Imaging Needs to be performed in ALL children <2 years old with initial UTI Need to perform at least 2 studies to image the upper and lower urinary tracts Acute imaging only necessary when appropriate clinical response is not achieved within 2 days

51
Ultrasound Should be done on all infants < 2yoa after their initial UTI Helps to detect hydronephrosis and ureteral dilation Has replaced IVP Need additional study to evalute VUR Is not as sensitive as renal cortical scintigraphy (DMSA) for detecting inflamation and scarring
 for detecting inflamation and scarring.")
52
Voiding Cystourethrography (VCUG)
Used to identify and grade reflux Also evaluates the urethra and bladder for abnormalities – important for boys who may have posterior urethral valves and girls with voiding dysfunction Radionuclide cystography (RNC) – can also evaluate reflux, but does not delineate the lower tract anatomy well. Can be used for follow-up exams as has low ratiation dose
 – can also evaluate reflux, but does not delineate the lower tract anatomy well. Can be used for follow-up exams as has low ratiation dose.")
53
Renal Cortical Scintigraphy (DMSA)
Very sensitive for evaluating acute inflammation from pyelonephritis as well as renal scarring Role in clinical management is still unclear

54
Treatment No “short course” therapy for small children
No “short course” therapy for males Empiric therapy is directed at organisms and adjusted for age. Choose narrowest spectrum allowable considering host factors Adjust therapy when sensitivities available Short course is NOT indicated for pyelonephritis but a recent study suggests it is acceptable in cystitis in children Arch Dis Childhood 2002 August 87 (2) :
 :")
55
IV antibiotics-Indications
Any person of any age who appears clinically toxic or who has neutropenia Infants <1 mo until bacteremia, sepsis, & meningitis ruled out Children unable to tolerate oral antibiotics Immunocompromised patients Multiple studies show NO benefit to outcome for children treated parentarelly vs orally. Arch Pediatr Adol Medicine 2001 Feb 155(2), “The addition of ceftriaxone to oral threapy does not improve outcome in febrile children with urinary tract infections. J Chemother, 2001, June:13(3): Comparative study of cefixime alone vs. intramuscular ceftizoime followed by cefixime in the treament of urinary tract infections in children
, The addition of ceftriaxone to oral threapy does not improve outcome in febrile children with urinary tract infections. J Chemother, 2001, June:13(3): Comparative study of cefixime alone vs. intramuscular ceftizoime followed by cefixime in the treament of urinary tract infections in children.")
56
Antibiotic choice Neonates
Ampicillin plus a second antibiotic (usually gentamycin or cefotaxime) to cover for GBS, Listeria, as well as gram negative organisms S. aureus and S. epi. can cause hematogenous pyelonephritis (in children instrumented :ET tube,central lines, etc) Vancomycin may be indicated for toxic patients or those unresponsive to initial therapy
 to cover for GBS, Listeria, as well as gram negative organisms. S. aureus and S. epi. can cause hematogenous pyelonephritis (in children instrumented :ET tube,central lines, etc) Vancomycin may be indicated for toxic patients or those unresponsive to initial therapy.")
57
Therapy Cefixime (Suprax) oral is as effective as parenteral ceftriaxone Cefpodoxime (Vantin) Bad tasting 10 mg/kg/day Fluoroquinolones are expensive and ”off label” in pedi Rationale is to cover for fecal coliforms which are usual culprits Need to be cognizant of local organisms; there is literature that supports the idea that Bactrim may be facing increasing levels of resistance in UTI organisms; fluoroquinolones may soon be approved for children less than 12 but are more expensive than most cephalosportins J Chemother Jun;13(3): Related Articles, Links Comparative study of cefixime alone versus intramuscular ceftizoxime followed by cefixime in the treatment of urinary tract infections in children. Gok F, Duzova A, Baskin E, Ozen S, Besbas N, B
: Related Articles, Links. Comparative study of cefixime alone versus intramuscular ceftizoxime followed by cefixime in the treatment of urinary tract infections in children. Gok F, Duzova A, Baskin E, Ozen S, Besbas N, B.")
58
Bacterial virulence Bacterial spectrum at the Ist Dept
Bacterial virulence Bacterial spectrum at the Ist Dept. of Pediatrics, in N= (%) E. coli Enterococcus faecalis 13 Proteus indol neg. 10 Klebsiella Pseudomonas spp 7 Enterobacter spp 6 Proteus indol pos 3 Staphylococcus Other
 E. coli 49. Enterococcus faecalis 13. Proteus indol neg. 10. Klebsiella 7. Pseudomonas spp 7. Enterobacter spp 6. Proteus indol pos 3. Staphylococcus 3. Other 2.")
59
Sensitive host Age related factors
Anatomy (short urethra, phymosis and adhesio cellularis preputii et labia minora, diaper) colonization Immunological susceptibility Mucosal barrier Inherited/acquired immunresponse Ex: IgA deficiency, P1 blood group
 colonization. Immunological susceptibility. Mucosal barrier. Inherited/acquired. immunresponse. Ex: IgA deficiency, P1 blood group.")
60
Sensitive host Anatomical malformations obstruction VUR
meningomyelokele prune-belly syndrome Stone disease, etc

61
Age-related incidence of UTI

62
Management of UTI

63
Prognosis

64
UTI Controversy #1: Antibiotic Prophylaxis
Indications grade 1 VUR frequent UTI recurrences Problems Pt Rxd with antibiotic prophylaxis Increased infection with Proteus and Enterobacter pseudomonas and Candida increased in children with urogenital abnormalities Drug toxicity and sensitivities Antimicrobial choices (qhs better) TMP-SMX or Nitrofurantoin (GI disturbance) Keflex if < 3 months Quinolones in some circumstances
 TMP-SMX or Nitrofurantoin (GI disturbance) Keflex if < 3 months. Quinolones in some circumstances.")
65
Posterior Urethral Valves
Abnormal congenital mucosal folds that are thin membranes impeding bladder drainage. Most common obstructive urethral lesion in male newborns found at the distal prostatic urethra. Incidence is approx’ly 1 in 8,000 males. Approx’ly 50% have reflux. VCUG is the modality of choice.

66
Radiographic signs of PUV:
distended prostatic urethra valve leaflets bladder and/or bladder neck hypertrophy diverticula narrow stream in the penile urethra incomplete emptying of the bladder

67
Treatment of PUV: Transurethral valve ablation, vesicostomy or upper tract diversion Urethral stricture is a common complication Fetal intervention carries a high risk with mortality rate of 43% ESRD, renal insufficiency and chronic renal failure are long-term consequences

68
30% of boys with posterior urethral valves whose symptoms present in infancy are at risk for progressive renal insufficiency.

70
PUV, 2 months , MCU

71
PUV, 2months

72
Mcu done for suspected PUV

73
9 months old child with dribbling of urine and difficulty in passing urine
?PUV MCU done Uroprophylaxis suggested Told by another Doc: not necessary Came with high grade fever after 1 month UTI

75
Vesicoureteral Reflux
Retrograde propulsion of urine into the upper urinary tract during bladder contraction. Primary reflux is caused by attenuation of the trigone and the contiguous intravesical ureteral musculature. May be caused by the ectopic insertion of the ureter into the bladder wall resulting in a shorter intravesicular ureter, which acts as an incompetent valve during urination.

76
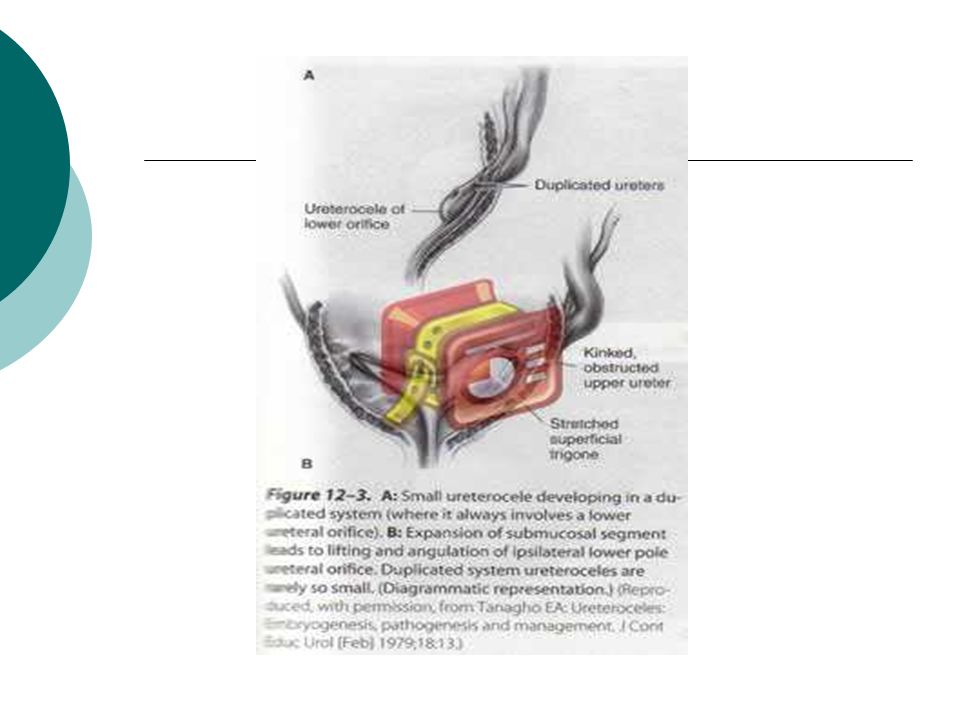
The ratio of the submucosal tunnel length to the ureteral diameter is the primary factor determining the effectiveness of the normal valve mechanism. It is normally 5:1, and in those with reflux it is 1.4:1. The intramural length increases from 0.5 cm at birth to 1.3 cm by 12 years of age. Duplication of the collecting system and ureteroceles should also be considered.

78
Some clinical facts about VUR:
It is genetic. Occurs in about 30% of first-degree relatives. 1/3 of children with a urinary tract infection has reflux on VCUG. Primary reflux tends to resolve over time as intravesical segment elongates with growth.

79
Grading of Vesicoureteral Reflux

80
VUR Grading Prognosis - 5% adults Scarring - 5-50% Screening UTI
Grade I Grade II Grade III Prognosis - 5% adults Scarring % Screening UTI Grade IV Grade V

81
Prognosis: Resolves spontaneously before adolescence in:
Kidney is most susceptible to scarring in the first year of life and at the time of first upper tract infection. Scars less frequently develop after the age of 5. VUR and scarring lead to hypertension, progressive renal insufficiency and failure. Resolves spontaneously before adolescence in: 90% of Gr. 1 reflux 80% of Gr. 2 50% of Gr. 3 10% of Gr. 4 0 in Grade 5 reflux

82
Treatment: Observation Medical treatment of infections
Surgical treatment significant hydroureteronephrosis indicated if impossible to keep urine sterile and reflux persists acute pyelonephritis occurs evidence of increasing renal damage

83
VUR

84
MCU C/o Recurrent UTI

86
Endoscopic submucosal injection

87
Endoscopic submucosal injection
Teflon Silicon Collagen

88
Bacterial virulence Virulence=factors that enable bacteria to invade the urinary tract Surface antigenes O: lipopolysacharides with endotoxin properties. Induces fever, local inflammation K, (capsular) antigene, prevents phagocytosis “P” fimbriae: bind to glycolipid receptors of the P blood group family A number of further factors not routinely checked
 antigene, prevents phagocytosis. P fimbriae: bind to glycolipid receptors of the P blood group family. A number of further factors not routinely checked.")
89
Bacterial virulence Pyelonephritis: 3-4 (known) virulence factors
Cystitis: 0-2 factors CAVE: OBSTURCTION !! MALFORMATION !!

Similar presentations













 as PID is an infection that affects a woman’s reproductive.>")



 Have a seat Take out a pen/pencil Be Quiet.>")





 are caused by pathogenic microorganisms in the urinary tract (the normal urinary tract is sterile above the.>")