Download presentation
Presentation is loading. Please wait.

1
The Socio-economic Burden of Diabetes in Developing Countries Lessons from studies in Egypt Professor Morsi Arab Egypt

2
Socioeconomics of Diabetes 1- The patient and human environment. 2- Patient’s Right and Obligations. 3- Factors deciding the burden of diabetes. 4- Size of the problem : Prevalence 5- Life Style 6- The national cost 7- Government and Household expenditure. 8- Cost of O.P. care 9-The hospital burden 10- Costs comparative to other countries.

3
The people with Diabetes and their Environment IDF Media Public. Com. Diab. Associations Family Friends Health Care Team Pharm. Ind. Syndicates Health Autho. WHO Patient

6
Determinants of impact 1. High prevalence 2. High cost of disease 3. Low economics 4. Adverse social conditions

8
CAIRO

11
Geographical distribution of the Egyptian population 56% 1% 43%

12
Age structure of the Egyptian population 40 30 20 10 0 10 20 30 40 60 -50 -40 -30 -60 -20 -10

13
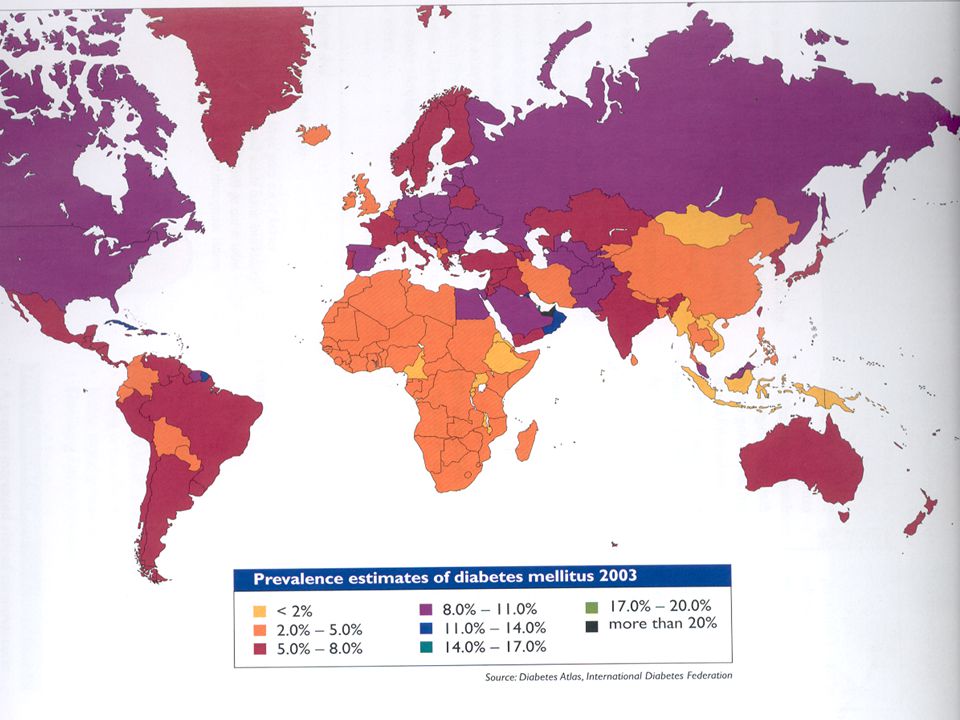
The estimated prevalence with DM by IDF region, 2000 Region Prevalence (%)
")
16
Prevalence of DM in the whole of Egypt in different age groups ? Prevalence (%)
")
17
Prevalence of DM Age range Prevalence (%)
")
18
Effect of change of the life style in migrating ethnic groups on metabolic parameters related to diabetes A lesson from the Nubians of Egypt Professor Morsi Arab University of Alexandria - Egypt

21
Prevalence of DM in patients over 40 yrs % Prevalence (>40yrs)
")
22
Conclusions 1. Changes in life style (diet & exercise( of susceptible individuals or groups is liable to increase their predisposition to DM (incidence of transformation of IGT to DM and consequently increased DM prevalence). 2. The change is more profoundly demonstrated among groups that might be originally protected by some genetically inherited characteristics. 3. Most of the parameters of the metabolic syndrome seem to be closely bound together and are prone to change under the influence of the adverse changes of life style.
. 2. The change is more profoundly demonstrated among groups that might be originally protected by some genetically inherited characteristics. 3. Most of the parameters of the metabolic syndrome seem to be closely bound together and are prone to change under the influence of the adverse changes of life style..")
23
Controlled metabolic parameters (% in diab. population Egypt 2003 ) - Fasting Bl. Glucose : 19.8% - P.P Bl. Glucose : 21.4% - S. Cholesterol : 56.4 % - S. Triglycerides : 50.4% - Syst. B.P. : 53.7% - Diastolic B.P. : 64.6%

24
Diabetes Complications (Egypt 2003) % in Diabetic population Retinopathy : 32.3% Neuropathy : 55.5% Nephropathy : 5.0% Cardiac Dis. : 21.3% Foot ulcers : 6.8% Foot amputations : 3.0% Foot deformities : 1.0%

25
The cost of Diabetes Data from Alexandria hospitals

26
Allocation of Direct Costs in hospital Medical supplies: –insulin etc.… Doctors Lab charges Basal cost: –Salaries, equipment, food, water, electricity’ laundry etc. Control of diabetes: –Insulin, OHA, medical supplies Rx complications: –Antibiotics, laser, haemo- dialysis, surgery etc. DIRECT COST Out-patient Hospital care

27
Indirect Costs Loss of working hours Diabetes mortality Premature death PRODUCTION

28
The cost of diabetes in Egypt O.P. care (per person per year) –Doctors’ charges:35.84 L.E. –Medical supplies30.36 L.E. –Laboratory charges19.68 L.E. 85.88 L.E. per year In-patient hospital care –Average total cost for one single admission/year, at average stay: 148.31 L.E. per year Alexandria Hospitals (86/88)
.")
29
The economic burden of direct cost of DM Total direct cost of diabetes in 1986: 160m Average inflation rate (1986-90)11.85% Estimated total direct cost in 1990235.2m Total Government expenditure on health, 1990: –National production31.3bn –Government expenditure at 40%12.6bn –2.8% Gov. expenditure on health351.8m

30
Cost of DM in relation to funds available DIRECT COST OF TREATMENT OF DM L.E.235.2m AVAILABLE GOVERNMENT EXPENDITURE ON HEALTH L.E. 351.8m 2/3!!

31
National economics and Reflections on health Per capita income %Government expenditure on health % Household consumption PARAMETERS

32
Gross National Product/Capita $000s NIESEE

33
NIES Percentage share of government expenditure HealthDefenceEducation %

34
% NIESEE Percentage share of total household consumption Medical careTotal foodEducation

35
Middle East Countries - economic status Kuwait Emerates Qatar Bahrain Oman Saudi Arabia Libya Israel Syria Jordan Tunisia Egypt Turkey Yemen Iraq Cyprus Iran HIGH ECONOMY LOW ECONOMY MIDDLE ECONOMY >5,000US$<2,000US$

36
Cost of out-patient ambulatory care of DM in Egypt compared with other Mediterranean countries (US$/month) *including treatment by dialysis
 *including treatment by dialysis")
37
Socio-economics - Some health and education parameters in 20 African countries

38
Socio-economics - Increasing total calorific intake

39
Distribution of costs of Hospital Treatment of Diabetic Patients ( L.E. per day ) at a Private Hospital for Middle Class Egyptian Population at the City of Alexandria, Egypt 2001
 at a Private Hospital for Middle Class Egyptian Population at the City of Alexandria, Egypt")
40
55% Medicine & Supp. 45% Basic ( Food : 5% H.C.Team 11% Others: 29%) Distribution of Hospital Cost
 Distribution of Hospital Cost")
41
Hospital Treatment 2001 Cost /Day

42
Estimated Costs of Ambulatory (out patient) Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year Estimated Costs of Ambulatory (out patient) Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year (A) Insulin ( Dose 10-80 units /d ) (B) Oral Antidiabetic Agents * Heavily subsidized ** moderately subsidized
 Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year Estimated Costs of Ambulatory (out patient) Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year (A) Insulin ( Dose units /d ) (B) Oral Antidiabetic Agents * Heavily subsidized ** moderately subsidized")
43
Animal u/40 Human u/40 Human u/100 Human/pen Metformin Glibenclam Gliclazide Glimeperide Rapiglinide Nateglinide Rosiglitazone Cost of O.P. Treatment (Egypt 2001) $/ y
 $/ y.")
44
Estimated Costs of Ambulatory (out patient) Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year ( Cont.) Estimated Costs of Ambulatory (out patient) Treatment of Diabetes in Egypt at 2001 Cost Prices in USD/ year ( Cont.) ( C ) Other costs at average frequencies per year Laboratory, and other follow – up investigations (E.C.G radiol., etc. ) Physician fees and other specialist consultations Total 143 USD/Year ( C ) Other costs at average frequencies per year Laboratory, and other follow – up investigations (E.C.G radiol., etc. ) Physician fees and other specialist consultations Total 143 USD/Year 76.4 66.6 76.4 66.6
 Physician fees and other specialist consultations Total 143 USD/Year ( C ) Other costs at average frequencies per year Laboratory, and other follow – up investigations (E.C.G radiol., etc. ) Physician fees and other specialist consultations Total 143 USD/Year")
45
The Burden of the Cost of Ambulatory Treatment of Diabetes on Individuals at Low-Income and High-Income Middle East Countries, based on the Cost Prices of Insulins and Oral Antidiabetic Agents (in USD per year) * Heavily subsidized ** moderately subsidized
 * Heavily subsidized ** moderately subsidized")
46
8.85% EGYPT 1.9% QATAR 3.1% SAUDI ARABIA Year Cost / percapit. Burden for Human Insulin (40 u /d)
")
47
The Burden of the Cost of Ambulatory Treatment of Diabetes on Individuals at Low-Income and High-Income Middle East Countries, based on the Cost Prices of Insulins and Oral Antidiabetic Agents ( in USD per year) (Cont.)
 (Cont.)")
49
EGYPT 29.9% Cost Burden of Oral Treatment related to Percapitum QATAR 4.2% 8.4% SAUDI ARABIA

50
Socio-economic impact on diabetes education 1. Lower economy; –less available resources for education 2. Lack of rational plan for: –patient education –physician education –other health personnel (nurses,dieticians,foot care etc…) –general public (awareness: food intake, obesity, exercise, early detection etc…)
 –general public (awareness: food intake, obesity, exercise, early detection etc…).")
51
Socio-economic impact on diabetes education 3. Lack of government awareness –of cost/benefit of education 4. Maldistribution –of available education facilities (urban/rural) 5. High illiteracy –adversely affects diabetes education & requires special methods -2
 5. High illiteracy –adversely affects diabetes education & requires special methods -2.")
52
Socio-economic impact on diabetes education 6. Misconceptions &... 7. Special education programmes –e.g for Ramadan fasting 8. Need to tailor diabetes education –& arrangements to suit local habits, traditions & lifestyle -3

53
Alexandrie – Palais du Montazah Thank You

Similar presentations