Download presentation
Presentation is loading. Please wait.

1
Jason Ryan, MD Intern Report
How to Read an EKG Jason Ryan, MD Intern Report

2
How to read an EKG Rate and Rhythm Axis and Intervals Hypertrophy
how fast/slow regular/irregular wide/narrow Axis and Intervals PR, QRS, QT Hypertrophy LAE/RAE LVH/RVH ST Changes and Q waves

3
How to read an EKG Rate 300 100 60 40 150 75 50

4
How to read an EKG Axis QRS Lead aVF (+) (-) -90o LAD Lead I (-) (+)
RAD Normal Axis 90o

5
How to read an EKG Intervals Correct QT 1. QTc=QT/(RR)1/2 (Bazett)
2. QTC=QT (HR-60) (Hodges) QRS QTc <0.46 PR
 (Hodges) QRS QTc. <0.46. PR")
6
How to Read and EKG Atrial Enlargement

7
How to Read and EKG Ventricular Enlargement

9
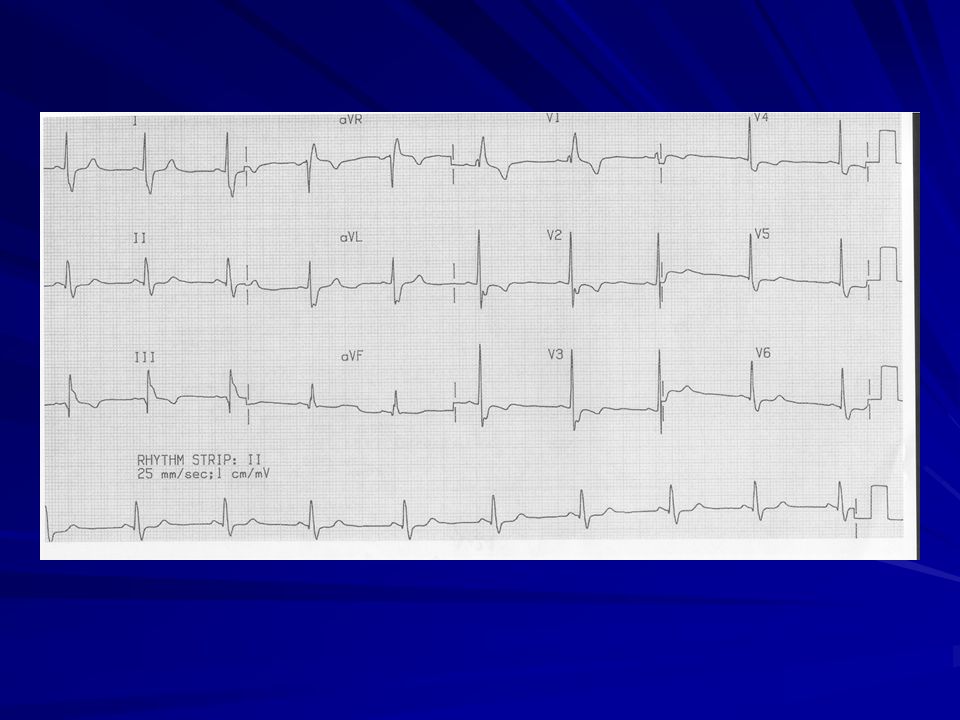
Sinus Rhythm Rate between 60 to 100 P wave before every QRS
Smooth contour Either all positive or all negative except V1 <0.12s and <0.2mv Upright P waves in I, II, aVF Negative P wave in aVR

11
Limb Lead Reversal Right and Left arm reversed
P wave positive aVR P wave negative aVL and I Limb leads look normal Right arm and Right leg reversed P wave negative I, L Lead II isoelectric (almost no QRS)
")
14
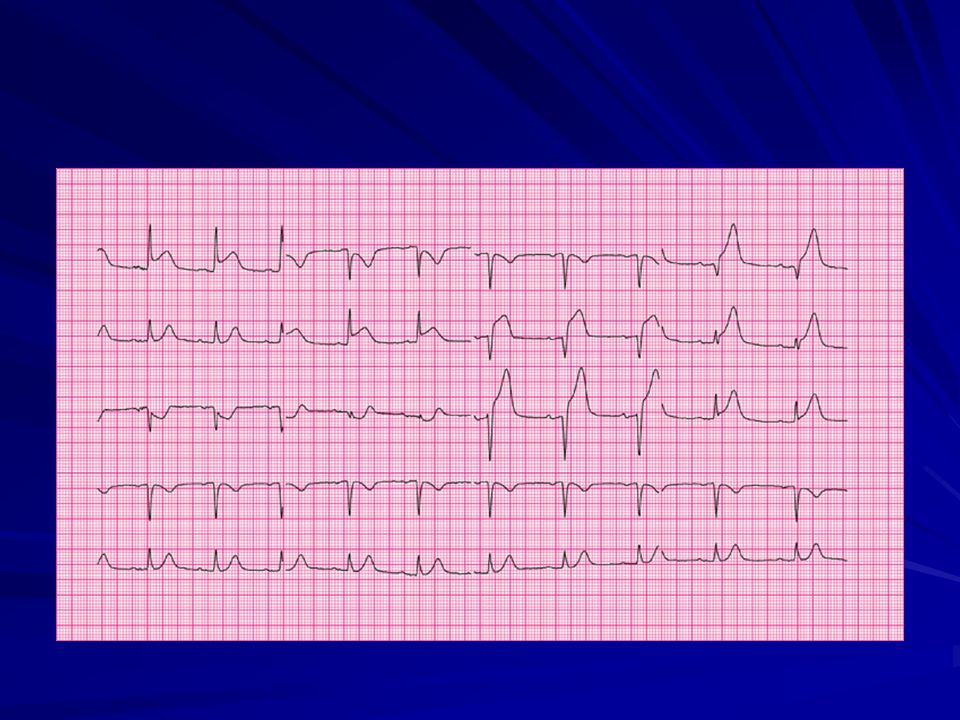
Left Bundle Branch Block
Criteria: QRS > 120ms (3 small boxes) Broad, notched, or slurred R waves in I, aVL, and V5-V6 Secondary ST-T changes in I, aVL, and V5-V6 Absence of Q waves in I, V5-V6 R-wave peak time >60ms (1.5 small boxes) V5-V6 Separate criteria for STE AMI
 Broad, notched, or slurred R waves in I, aVL, and V5-V6. Secondary ST-T changes in I, aVL, and V5-V6. Absence of Q waves in I, V5-V6. R-wave peak time >60ms (1.5 small boxes) V5-V6. Separate criteria for STE AMI.")
16
Right Bundle Branch Block
Criteria: QRS >120ms (3 small boxes) R’ in the right precordial leads with R’>R Secondary ST-T changes in R precordial leads Supporting findings: Slurred S wave in I, aVL, left precordial leads Usual criteria for STE AMI apply
 R’ in the right precordial leads with R’>R. Secondary ST-T changes in R precordial leads. Supporting findings: Slurred S wave in I, aVL, left precordial leads. Usual criteria for STE AMI apply.")
18
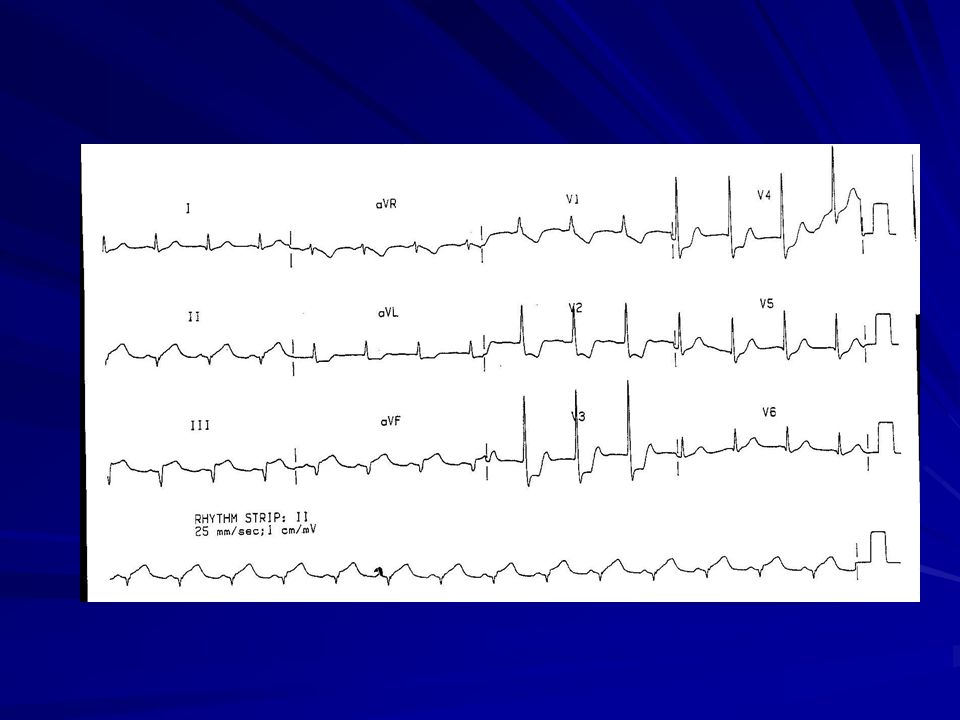
Left Ventricular Hypertrophy
SV1orV2+ RV5orV6>35mm >40 if 30-40yrs old >60 if 16-30yrs old RaVL>11mm RI + SIII >25mm RaVL + SV3 >28mm(men) or 20mm(wmn)
 or 20mm(wmn)")
19
Left Ventricular Hypertrophy
Associated ST-T wave abnormalities STD and TWI in V5-V6 Leads where QRS is mainly positive Slight STE with upright T in V1-V2 Leas where QRS is mainly negative

21
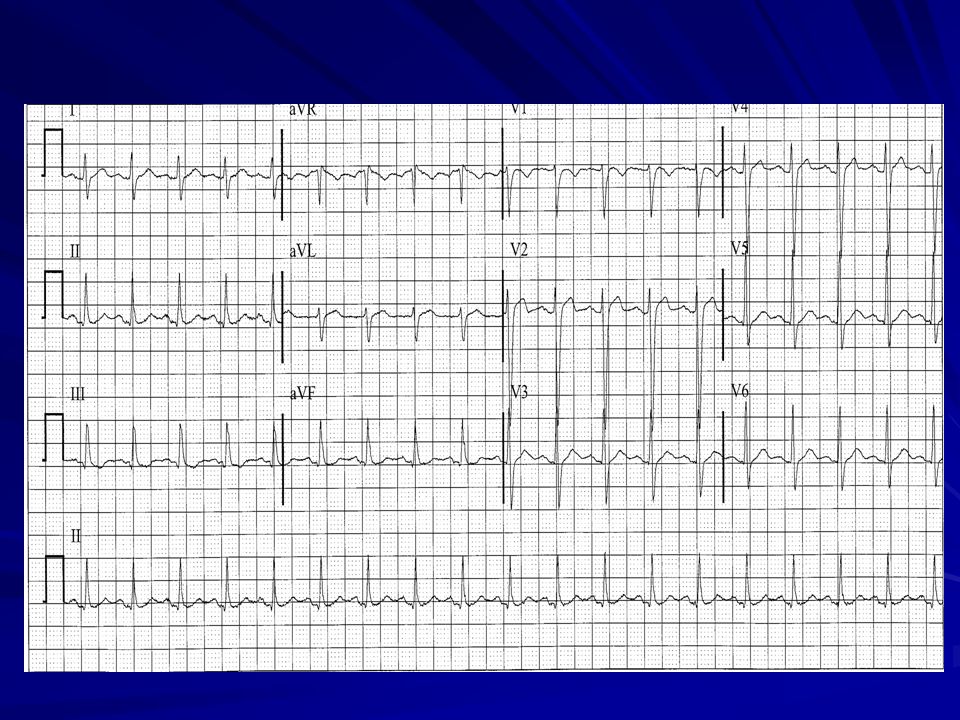
Sinus Tachycardia All sinus rhythm criteria Rate >100
P before every QRS Upright P in I, II, aVF Inverted P aVR Rate >100

23
T Wave Inversions Indicative of subendocardial or evolving ischemia
Can be a normal variant in several leads or in the presence of BBB Can be caused by several other conditions Hypertrophic obstructive cardiomyopathy Intracranial processes (hemorrhage) Medications or electrolyte abnormalities Myocarditis/pericarditis or pulmonary embolism
 Medications or electrolyte abnormalities. Myocarditis/pericarditis or pulmonary embolism.")
25
ST depressions Horizontal ST depressions are strongly suggestive of ischemia in the appropriate clinical setting Don’t necessarily localize Stress testing Reciprocal changes Several other conditions can provoke ST depressions: LVH Medications or electrolytes Bundle Branch Block Pulmonary embolism

27
ST Elevations Localizes best of all ischemic EKG changes
Usually indication of acute myocardial injury (occluded artery) Several conditions can also cause ST elevations: Pericarditis Early repolarization LBBB LVH
 Several conditions can also cause ST elevations: Pericarditis. Early repolarization. LBBB. LVH.")
28
Evolution of EKG changes
ST Elevation MI Evolution of EKG changes Normal Acute Hours 1-2 Days 3-7 Days > 7 Days

29
Leads go together Anterior

30
Leads go together Lateral

31
Leads go together Inferior

Similar presentations





















, tachycardia (170) and “dusky” in appearance.>")







