Download presentation
Presentation is loading. Please wait.

1
Proprioceptive Neuromuscular Facilitation
National Rehabilitation Center Kim, Seok-Hwan

2
Proprioceptive Neuromuscular Facilitation (PNF)
Methods of promoting or hastening the response of the neuromuscular mechanism through stimulation of the proprioceptor. Major Goal – Restore or enhance postural responses or normal patterns of motion.

3
Basic Neurophysiologic Principles of PNF Diagonals of Movement
Innate path in which maximal response of the trunk and extremities can be facilitated. Components associated with antagonistic motion: Flexion versus extension. Abduction versus adduction in extremities and lateral movement of trunk. Internal vs. external rotation.

4
Reflects functional relationship of trunk
Normal coordinated patterns of motion are diagonal in direction with spiral components – Facilitate strongest output. Reflects functional relationship of trunk and extremities. Diagonals may be used to identify: Quality of contractions Range of motion Functional impairments/limitations

5
Motor Development PNF is based on 11 principles drawn from:
Neurophysiology Motor learning Motor behavior

6
Examination and Evaluation Assessed Areas:
Impaired ROM and muscle length Impaired muscle power Impaired muscle endurance Impaired balance Impaired posture Impaired motor control Pain

7
Factors Included During the Evaluation
Patient’s short-term and long-term goals. Patient’s receptive potential for language, vision, and manual contacts to promote cuing. Patient’s strengths. Patient’s weaknesses.

8
Treatment Implementation
Treatment interventions may include: Modification of environment Education and compensation for the impairment Treatment directed at changing the patient’s neuromuscular capabilities

9
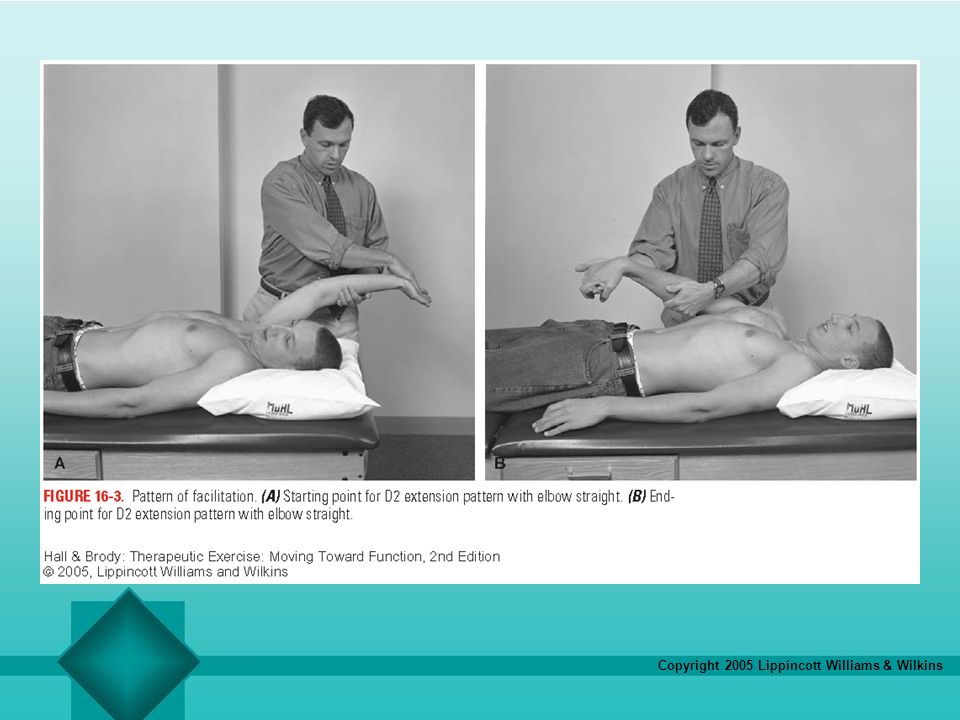
Patterns of Facilitation
Manually resistive exercises that create the diagonals of movement by coupling pairs of antagonistic patterns, providing a path for reversing motions, and using the agonist–antagonist relationship of the nervous system as techniques are applied.

10
Procedures Body positioning and mechanics Manual contacts
Manual and maximal resistance Irradiation Verbal and visual cuing Traction and approximation Stretch Timing

11
Body Positioning and Mechanics
Be positioned in the diagonal plane or treatment plane whenever possible. Shoulders and hips face toward direction of movement. Forearms in this plane is important.

13
Manual Contacts Use contacts overlying agonist muscle group to strengthen contractions and/or direction of movement. Use lumbrical grip to provide contact. Contact the target group (direct effect) or synergist or antagonist (indirect).
 or synergist or antagonist (indirect).")
14
Manual and Maximal Resistance
Resistance to motion enhances muscle activation. Direction, quality, and quantity of resistance are adjusted according to treatment goals. Resistance should be no greater than the resistance that allows full ROM.

15
Irradiation (Overflow)
Spread of energy from agonist to complimentary agonists and antagonists within a pattern. Irradiation is stimulated through clinician’s use of resistance. Weaker muscle groups benefit while working in synergy with more normal partners.

16
Verbal Cuing Should be clear and concise.
Begin by detailing a particular patient response. Change to more simple cues for subsequent repetitions. Alter tone according to goal (e.g., soft voice for inhibition)
")
17
Approximation and Traction
Stimulates receptors to facilitate co-contraction and stability around the joint. Employed through the use of weight-bearing developmental postures. Traction is commonly used with pulling movements to inhibit compression.

18
Stretch Often performed at the starting position of a pattern or movement. Result – Reflex activation. Resistance through entire range provides continued stretch through tension. Stretch can be repeated at start of range or superimposed during a pattern.

19
Techniques of Facilitation
Rhythmic initiation Repeated contractions Reversals of antagonists Dynamic reversals of antagonists Stabilizing reversals 6. Rhythmic stabilization 7. Hold and relax 8. Contract and relax 9. Combination of isotonics (dynamics)
")
20
Uses of Rhythmic Initiation
Initiate movement. Define the direction or pattern of movement. Set the appropriate rate of movement. Improve coordination and sense of motion. Promote general relaxation.

21
Uses of Repeated Contractions
Help to initiate movement. Strengthen agonist movement pattern from lengthened range. Strengthen agonist movement pattern within available ROM. Redirect motion within pattern or task.

22
Use of Reversals of Antagonists
To facilitate agonist. Improve balance between agonist and antagonist.

23
Use of Dynamic Reversals of Antagonists
Increase active ROM. Improve strength in the available ROM. Improve balance and coordination of antagonist. Improve endurance of antagonistic patterns.

24
Use of Stabilizing Reversals
Improve balance and stability. Improve strength. Integrate a new posture or ROM into function.

25
Use of Rhythmic Stabilization
Improve strength of antagonists. Improve balance of antagonists. Improve stability. Increase active and passive ROM following technique. Decrease pain.

26
Use of Hold and Relax Improve PROM. Provide relaxation. Reduce pain.

27
Use of Contract and Relax
Improve passive ROM. Provide relaxation.

28
Use of Combination of Isotonics
Increase strength of agonist. Increase active ROM. Teach functional control.

29
Summary PNF is a manual therapy approach that applies postures, movement patterns, contacts, cues, and goals. All = Maximally facilitating. Treatment is based on improving function, and using functions that are possible to reach those are attainable goals. PNF lends itself to use as an adjunct to other treatment approaches.

Similar presentations



 Techniques in Rehabilitation Chapter 14.>")





>")

>")
 connected in bundles Muscle fibers are made up of myofibrils Strength training increases the.>")






