Download presentation
Presentation is loading. Please wait.

1
Epidemiology of Neurological Disorders
Dr. Yeşim YASİN Fall-2013

2
Outline: Global burden of neurological disorders
National burden of neurological disorders Most commonly seen neurological disorders: a public health approach Prevention

3
Global burden of disesase
Neurological diseases are becoming increasingly important in terms of public health throughout the world and in Turkey. One of the most remarkable collaborative endeavours was the Global Burden of Disease study, which was a result of the coordinated effort of WHO, the World Bank and Harvard School of Public Health. The Global Burden of Disease report drew the attention of the international health community to the fact that the burden of mental and neurological disorders had been seriously underestimated by traditional epidemiological methods that took into account only mortality, not disability rates. This report specifically showed that while mental and neurological disorders are responsible for about 1% of deaths, they account for almost 11% of disease burden worldwide (2).
.")
4
Global burden of disesase
The Global Burden of Disease report drew the attention of the international health community to the fact that the burden of mental and neurological disorders had been seriously underestimated by traditional epidemiological methods that took into account only mortality, not disability rates.

5
Global burden of disease
The Global Burden of Disease report specifically showed that while mental and neurological disorders are responsible for about 1% of deaths, they account for almost 11% of disease burden worldwide The Global Burden of Disease (GBD) approach is one of the most widely used frameworks for information on summary measures of population health across disease and risk categories
 approach is one of the most widely used frameworks for information on summary measures of population health across disease and risk categories.")
6
Many conditions including neuropsychiatric disorders and injuries cause considerable ill-health but no or few direct deaths. Separate measures of survival and of health status among survivors needed to be combined to provide a single, holistic measure of overall population health.

7
Many conditions including neuropsychiatric disorders and injuries cause considerable ill-health but no or few direct deaths.

8
To assess the burden of disease; measures both
premature mortality (years of life lost because of premature mortality or YLL) disability (years of healthy life lost as a result of disability or YLD, weighted by the severity of the disability). YLL (years of life lost) erken mortaliteye bağlı kaybedilen yılları ifade eder (yaşam beklentisi x ölüm sayısı). YLD (years with lived disability) sakatlık nedeniyle kaybedilen sağlıklı yıllar DALY=YLL + YLD
 disability (years of healthy life lost as a result of disability or YLD, weighted by the severity of the disability). YLL (years of life lost) erken mortaliteye bağlı kaybedilen yılları ifade eder (yaşam beklentisi x ölüm sayısı). YLD (years with lived disability) sakatlık nedeniyle kaybedilen sağlıklı yıllar. DALY=YLL + YLD.")
9
The sum of these two components, disability-adjusted life years (DALYs),
provides a measure of the future stream of healthy life (years expected to be lived in full health) lost as a result of the incidence of specific diseases and injuries
 lost as a result of the incidence of specific diseases and injuries.")
10
Neuropsychiatric disorders and injuries in particular were major causes of lost years of healthy life as measured by DALYs, were significantly underestimated when measured by mortality alone

11
The cause categories used in the GBD study is divided into three broad groups of causes:
Group I consists of communicable diseases, maternal causes, conditions arising in the perinatal period and nutritional deficiencies; Group II encompasses the noncommunicable diseases (including neuropsychiatric conditions); and Group III comprises intentional and unintentional injuries.
; and. Group III comprises intentional and unintentional injuries.")
12
Common neurological disorders
Stroke Dementia Epilepsy parkinsonS disease Headeache disorders Multiple sclerosis Neuroinfections Neurological disorders associated with malnutrition Pain associated with neurological disorders Traumatic brain disorder Stroke is one of the main noncommunicable diseases of public health importance. After coronary heart disease and cancer, stroke is the most common cause of death in most industrialized countries. In general terms, stroke is a sudden neurological deficit owing to localized brain ischaemia or haemorrhage. Most strokes are attributed to focal occlusion of the cerebral blood vessel (ischaemic stroke) and the remainder are the result of rupture of a blood vessel (haemorrhagic stroke). Serebrovasküler hastalıklar dünyada 3. ölüm nedeni
 and the remainder are the result of rupture of a blood vessel (haemorrhagic stroke). Serebrovasküler hastalıklar dünyada 3. ölüm nedeni.")
13
Estimates of disability adjusted life years (DALYs)
")
14
Table 1. Number of DALYs for neurological disorders and as percentage of global DALYs projected for and 2030 neuropsychiatric category 2% 4.3%

15
Percentage of total DALYs for selected diseasesa and neurological disordersb
Neurological disoerders constitute slightly over 6% of total burden,

16
DALYs for individual neurological disorders as percentage of total neurological disorders
Among neurological disorders, more than half of the burden in DALYs is contributed by cerebrovascular disease, 12% by Alzheimer and other dementias and 8% each by epilepsy and migraine

17
Neurological disorders as percentage of total DALYs for 2005, 2015 and 2030 across income category
Neurological disorders contribute to 10.9%, 6.7%, 8.7% and 4.5% of the global burden of disease in high, upper middle, lower middle and low income countries, respectively, in 2005.

18
Estimates of deaths

19
Deaths attributable to neurological disorders as percentage of total deaths, 2005, 2015, 2030
Neurological disorders are an important cause of mortality and constitute 12% of total deaths globally (see Table 2.7). Within these, cerebrovascular diseases are responsible for 85% of the deaths due to neurological disorders
. Within these, cerebrovascular diseases are responsible for 85% of the. deaths due to neurological disorders.")
20
Deaths from selected neurological disorders as percentage of total neurological disorders
cerebrovascular diseases are responsible for 85% of the deaths due to neurological disorders

21
Deaths and DALYs from selected neurological disorders as percentage of total neurological disordres
Among neurological disorders, more than half of the burden in DALYs is contributed by cerebrovascular Disease cerebrovascular diseases are responsible for 85% of the deaths due to neurological disorders Deaths

22
Neurological disorders as percentage of total deaths for 2005, 2015 and 2030 across World Bank income category Neurological disorders constitute 16.8% of the total deaths in lower middle income countries compared with 13.2% of the total deaths in high income countries. Neurological disorders constitute 16.8% of the total deaths in lower middle income countries compared with 13.2% of the total deaths in high income countries.

23
Estimates of years of healthy life lost as a result of disability (YLDs)
")
24
The number of YLDs per population associated with neurological disorders and other diseases and injuries with neurological sequelae is projected to decline from 1264 in 2005 to 1109 in 2030 YLDs per population associated with neurological disorders and other diseases and injuries with neurological sequelae and as percentage of total YLDs projected for 2015 and 2030

25
YLDs per population associated with neurological disorders and other diseases and injuries with neurological sequelae and as percentage of total YLDs projected for 2015 and 2030 YLDs associated with Alzheimer and other dementias, however, are projected to increase by 38%. YLDs associated with Alzheimer and other dementias, however, are projected to increase by 38%. When expressed as a percentage of the total, YLDs associated with neurological disorders and other diseases and injuries with neurological sequelae comprise 14% of the total in 2005 and are projected to remain the same by 2030.

26
Top five causes of YLDs among neurological disorders, by income category
YLDs per population for neuroinfections, and the nutritional deficiencies and neuropathies category are highest for low income countries neurological injuries, epilepsy and migraine, they are highest in upper middle income countries For Alzheimer and other dementias they are highest for high income countries

27
YLDs associated with neurological disorders by income category
almost half of the burden in terms of YLDs attributable to neurological disorders is in low income countries followed by lower middle income countries YLDs associated with neurological disorders by income category

29
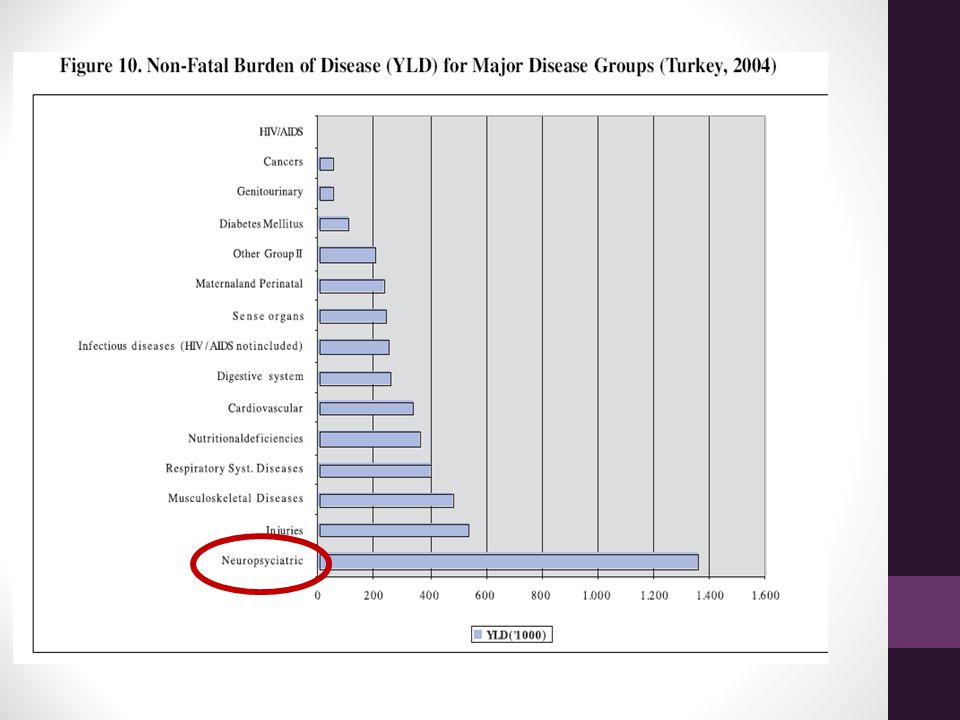
Turkey, Burden of Disease
In our country neurological diseases are becoming increasingly important because of increasing life expectancy and related to incerasing elderly population.

30
Turkey, Burden of disease
As seen in Table 5, ischaemic heart diseases occupy the first rank with 21,7 %, cerebrovascular diseases occupy the second rank with 15 %

31
As seen in Table 11, first three ranks in total burden of disease are occupies orderly by perinatal causes (8,9 %), ischemic heart diseases (8 %) and cerebrovascular diseases (5,9 %). Daly hesaplamsında kaybedilen yıllar da dikkate alındığından ilk sırayı daha genç ölümlerle seyreden perinatal nedenler almıştır.

35
BURDEN ATTRIBUTABLE TO SEVEN BASIC RISK FACTORS
High colesterol Smoking High body mass index High blood pressure Alcohol use Insufficient consumption of fruits and vegetables Physical inactivity Türkiye hastalık yükü çalışması bize kardiyovasküler ve serebrovasküler hastalıklar için risk faktörlerinin durumu ile de değerli bilgiler sağlamıştır. Ve bu risk faktörlerine atfedilen hızlar hesaplanmıştır.

36
Hypertension as a common risk factor
number of deaths attributed to hypertension, which refers to the fact that they could be prevented by keeping hypertension under control is for cerebrovascular diseases

37
alcohol consumption-attributed deaths are mostly the
consequences ischemic heart diseases and hemorragic stroke. 2088 deaths caused by hemorrhagic stroke could be prevented by prevention of alcohol consumption

38
11109 deaths caused by ischemic stroke could be prevented by prevention of obesity

39
high cholesterol is among major risk factors of ischemic heart diseases and ischemic stroke.
Prevention of high cholesterol could prevent deaths caused by ischemic stroke

40
Sufficient amount of physical activity could prevent 10
Sufficient amount of physical activity could prevent deaths caused by ischemic stroke. As for burden of disease which is preventable, physical activity could prevent DALY in ischemic stroke.

42
Prevention Many neurological disorders can be prevented!
One of the important actions required by the health sector is an immunization programme for the prevention of neuroinfections, such as poliomyelitis, and the neurological consequences of infections (e.g. Hemophilus infl uenzae type B (Hib)). Meningitis caused by Hib has been nearly eliminated in the industrialized world since routine vaccination with the H. infl uenzae type B conjugate vaccine was initiated. BCG vaccination does not prevent transmission of tuberculosis but is still recommended because of its high protective effi cacy against serious forms of the disease in children (73% for meningitis and 77% for miliary tuberculosis). A number of strategies implemented at policy level by governments through legislation, tax or fi nancial incentives can reduce risks to health. For example, in the area of road safety, a signifi cant number of people might not choose to drive safely or to use seatbelts or motorcycle helmets, but government action can encourage them to do so, thereby preventing injuries to themselves and to other people. This would also result in prevention of other disorders secondary to trauma such as epilepsy. Control of cardiovascular diseases including stroke can be handled through a comprehensive approach taking account of a variety of interrelated risk factors including blood pressure, cholesterol, smoking, body mass index, low levels of physical activity, diet and diabetes. A comprehensive national strategy thus combining prevention, community-based health promotion and access to treatment can substantially decrease the burden associated with cardiovascular diseases, including stroke. Disability consequent to neurological disorders can be decreased by rehabilitation programmes and policies. For example, building ramps and other facilities to improve access by disabled people falls beyond the purview of the health sector but is nevertheless very important for comprehensive management of people with disability.
). Meningitis caused by Hib has been nearly. eliminated in the industrialized world since routine vaccination with the H. infl uenzae type B conjugate vaccine was initiated. BCG vaccination does not prevent transmission of tuberculosis but. is still recommended because of its high protective effi cacy against serious forms of the disease. in children (73% for meningitis and 77% for miliary tuberculosis). A number of strategies implemented at policy level by governments through legislation, tax or. fi nancial incentives can reduce risks to health. For example, in the area of road safety, a signifi cant. number of people might not choose to drive safely or to use seatbelts or motorcycle helmets, but. government action can encourage them to do so, thereby preventing injuries to themselves and. to other people. This would also result in prevention of other disorders secondary to trauma such. as epilepsy. Control of cardiovascular diseases including stroke can be handled through a comprehensive. approach taking account of a variety of interrelated risk factors including blood pressure, cholesterol, smoking, body mass index, low levels of physical activity, diet and diabetes. A comprehensive. national strategy thus combining prevention, community-based health promotion and access. to treatment can substantially decrease the burden associated with cardiovascular diseases, including stroke. Disability consequent to neurological disorders can be decreased by rehabilitation programmes. and policies. For example, building ramps and other facilities to improve access by disabled people. falls beyond the purview of the health sector but is nevertheless very important for comprehensive. management of people with disability.")
43
Prevention Primary prevention Secondary prevention Tertiary prevention

44
Primary prevention High risk approach (individual approach)
Population based approach

45
Prevention- high risk strategy
Elimination of the major risk factors. Controlling high blood pressure Lowering the level of blood cholesterol Quitting tobacco use Controlling diabetes Maintaining a healthy weight, body mass index Diet Exercising regularly Prevention and treatment of coronary hearth diseases Control of cardiovascular diseases including stroke can be handled through a comprehensive approach taking account of a variety of interrelated risk factors including blood pressure, cholesterol, smoking, body mass index, low levels of physical activity, diet and diabetes. A comprehensive national strategy thus combining prevention, community-based health promotion and access to treatment can substantially decrease the burden associated with cardiovascular diseases, including stroke.

46
Prevention- population based strategy
Raising awareness of health personnel about treatment and prevention of neurological diseases A comprehensive national strategy; community-based health promotion and access to treatment can substantially decrease the burden associated with cerebrovascular diseases (stroke)
")
47
Prevention-population based strategy
Health promotion programmes to prevent risk factors. Smoke free air space Diabet control programmes Promoting and creating built or natural environments that encourage and support physical activity.

48
Prevention- population based strategy
immunization programme for the prevention of neuroinfections (poliomyelitis, neurological consequences of infections) Road safety – prevention of traumatic brain injury One of the important actions required by the health sector is an immunization programme for the prevention of neuroinfections, such as poliomyelitis, and the neurological consequences of infections (e.g. Hemophilus infl uenzae type B (Hib)). Meningitis caused by Hib has been nearly eliminated in the industrialized world since routine vaccination with the H. infl uenzae type B conjugate vaccine was initiated. BCG vaccination does not prevent transmission of tuberculosis but is still recommended because of its high protective efficacy against serious forms of the disease in children (73% for meningitis and 77% for miliary tuberculosis). A number of strategies implemented at policy level by governments through legislation, tax or financial incentives can reduce risks to health. For example, in the area of road safety, a signifi cant number of people might not choose to drive safely or to use seatbelts or motorcycle helmets, but government action can encourage them to do so, thereby preventing injuries to themselves and to other people. This would also result in prevention of other disorders secondary to trauma such as epilepsy. VDisability consequent to neurological disorders can be decreased by rehabilitation programmes and policies. For example, building ramps and other facilities to improve access by disabled people falls beyond the purview of the health sector but is nevertheless very important for comprehensive management of people with disability. ASPIRIN In cases of acute stroke, aspirin is given as soon as CT or MRI has excluded intracranial haemorrhage. Immediate aspirin treatment slightly lowers the risk of early recurrent stroke and increases the chances of survival free of disability: about one fewer patient dies or is left dependent per 100 treated. However, because aspirin is applicable to so many stroke patients, it has the potential to have a substantial public health effect. Aspirin is also likely to reduce the risk of venous thromboembolism. Traumatic brain injury is the leading cause of death and disability in children and young adults
 Road safety – prevention of traumatic brain injury. One of the important actions required by the health sector is an immunization programme for the prevention of neuroinfections, such as poliomyelitis, and the neurological consequences of infections (e.g. Hemophilus infl uenzae type B (Hib)). Meningitis caused by Hib has been nearly eliminated in the industrialized world since routine vaccination with the H. infl uenzae type B conjugate vaccine was initiated. BCG vaccination does not prevent transmission of tuberculosis but is still recommended because of its high protective efficacy against serious forms of the disease in children (73% for meningitis and 77% for miliary tuberculosis). A number of strategies implemented at policy level by governments through legislation, tax or financial incentives can reduce risks to health. For example, in the area of road safety, a signifi cant number of people might not choose to drive safely or to use seatbelts or motorcycle helmets, but government action can encourage them to do so, thereby preventing injuries to themselves and. to other people. This would also result in prevention of other disorders secondary to trauma such as epilepsy. VDisability consequent to neurological disorders can be decreased by rehabilitation programmes and policies. For example, building ramps and other facilities to improve access by disabled people falls beyond the purview of the health sector but is nevertheless very important for comprehensive management of people with disability. ASPIRIN In cases of acute stroke, aspirin is given as soon as CT or MRI has excluded intracranial haemorrhage. Immediate aspirin treatment slightly lowers the risk of early recurrent stroke and increases the chances of survival free of disability: about one fewer patient dies or is left dependent per 100 treated. However, because aspirin is applicable to so many stroke patients, it has the potential to have a substantial public health effect. Aspirin is also likely to reduce the risk of venous thromboembolism. Traumatic brain injury is the leading cause of. death and disability in children and young adults.")
49
Tertiary prevention ASPIRIN In cases of acute stroke, aspirin is given as soon as CT or MRI has excluded intracranial haemorrhage. Using medication Rehabilitation Immediate aspirin treatment slightly lowers the risk of early recurrent stroke and increases the chances of survival free of disability about one fewer patient dies or is left dependent per 100 treated. However, because aspirin is applicable to so many stroke patients, it has the potential to have a substantial public health effect. Tertiary prevention is important esp in cerebrovascular diseases. Reccurrence after first stroke is often. For this reason using anticoagulan like aspirin and heparin is necessary to prevent recurrent stroke. Rehabilitation is also imp for stroke patient to control or improve diasbility.

50
WHO recommendations Gain commitment from decision-makers
Increase public and professional awareness Minimize stigma and eradicate discrimination Strengthen neurological care within the existing health systems Incorporate rehabilitation into the key strategies Establish links to other sectors Define priorities for research

51
Conclusions Estimating the burden of diseases is difficult due to
imperfect medical registration, variations in structure of patient referral and influence of secondary diagnoses. Taking into account the current aging of the population, the prevalence of some neurological diseases, such as CVA, Parkinson's disease and dementia will rise. Priority setting for care and treatment is hampered by differences in burden of illness on the individual and on the community level

52
THANK YOU!

Similar presentations








 Prevention and Healthy.>")














