Download presentation
Presentation is loading. Please wait.

1
Cary Hopkins Eyles, MA, CAP Samantha A. Farro, PhD Colleen Clark, PhD Annual Conference August 25, 2011 Orlando, Florida

2
The Centrality of Trauma What is Trauma-Informed Care? Assessing Readiness for Trauma- Informed Care Integrating Care for Co-occurring Disorders and Trauma Issues Making it all Work for the Client

3
Clients seeking substance abuse and mental health treatment often have history of trauma. History of trauma complicates treatment. Integrated care is more cost effective and demonstrates more positive outcomes of treatment

5
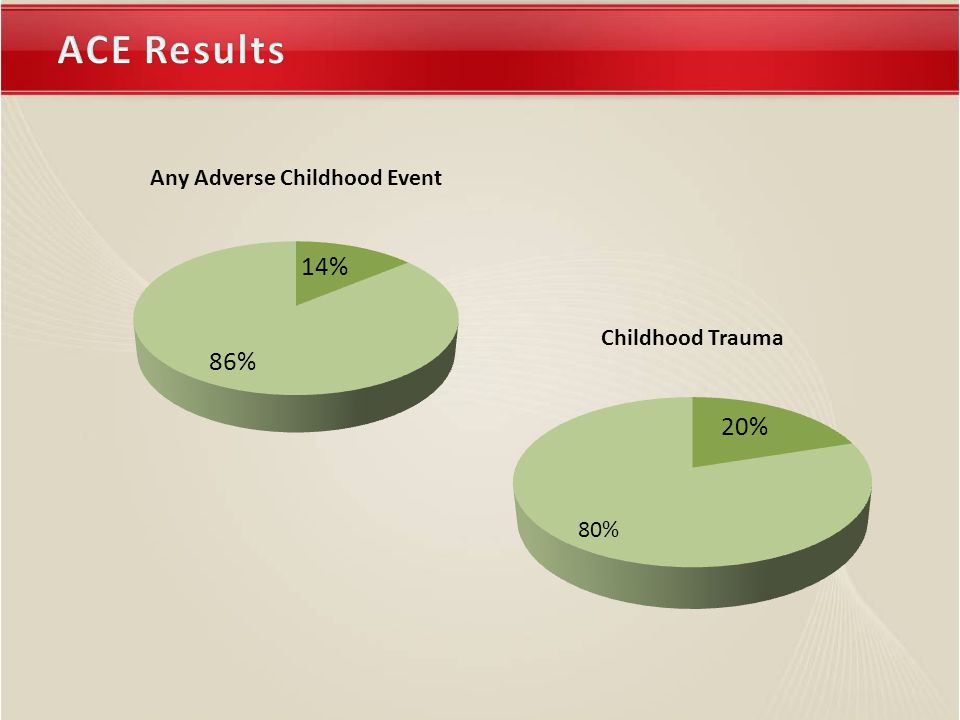
5 Recurrent & severe physical abuse11% Recurrent & severe emotional abuse11% Contact sexual abuse22% Growing up in a household with: Alcoholic or drug-user25% Member being imprisoned3% Mentally ill, chronically depressed, or institutionalized member 19% The mother being treated violently12% Both biological parents NOT present 22%

6
6 ACE Score vs. Adult Alcoholism Family Care Version: Understanding Trauma & Trauma-Informed Care

7
7 Significant odds ratios- compared to twins with no CSA (n=1411 twins) 72.7% Kendler et. al 2000 DiagnosisAny CSA Nongen -ital CSA Genita l CSA Interco urse Major depression1.931.733.14 GAD1.891.592.94 Panic disorder1.892.55 Bulimia3.30 Alcohol depend.2.802.422.394.01 Drug dependence3.092.931.975.70 ≧ Disorders 2.581.612.045.47

8
How mental health, substance abuse, violence work together

9
9 Trauma Substance Abuse ♀

10
10 Following traumatic event – substance abuse as “self-medication” “self-soothing” Substance abuse leading to high risk situations or poor judgment increasing chances of victimization

11
11 Trauma Mental illness, Emotional disorders ♀

12
12 Violence and abuse, especially over a long term, abuse by multiple perpetrators and/or extremely violence abuse is associated with the development of many disorders. Some responses to abuse – SIV, flashbacks, result in involuntary hospitalization, seclusion, restraints and possible retraumatization People with mental illnesses are more likely to be victims of violence

13
13 Substance abuse Mental illness, Emotional disorders ♀

14
Integrated treatment is complex to assess and difficult to implement. Current empirical approaches require a great deal of time and resources

15
Consumer Perspective Description: Examines prevalence of childhood trauma and perceptions of service integration and choice at DACCO’s residential treatment Method: Survey data is statistically analyzed to examine mean differences, correlations, and frequencies. Sample: Female and male clients in residential treatment Staff Perspective Description: Assesses staff perspective about residential treatment’s level of trauma informed care on six dimensions Method: Semi-structured interviews of staff are qualitatively coded using an anchored rating scale Sample: Agency’s staff leaders in residential treatment

16
Adverse Childhood Experiences Scale Consumer Perceptions of Care Scale Community Readiness Model Interviews

17
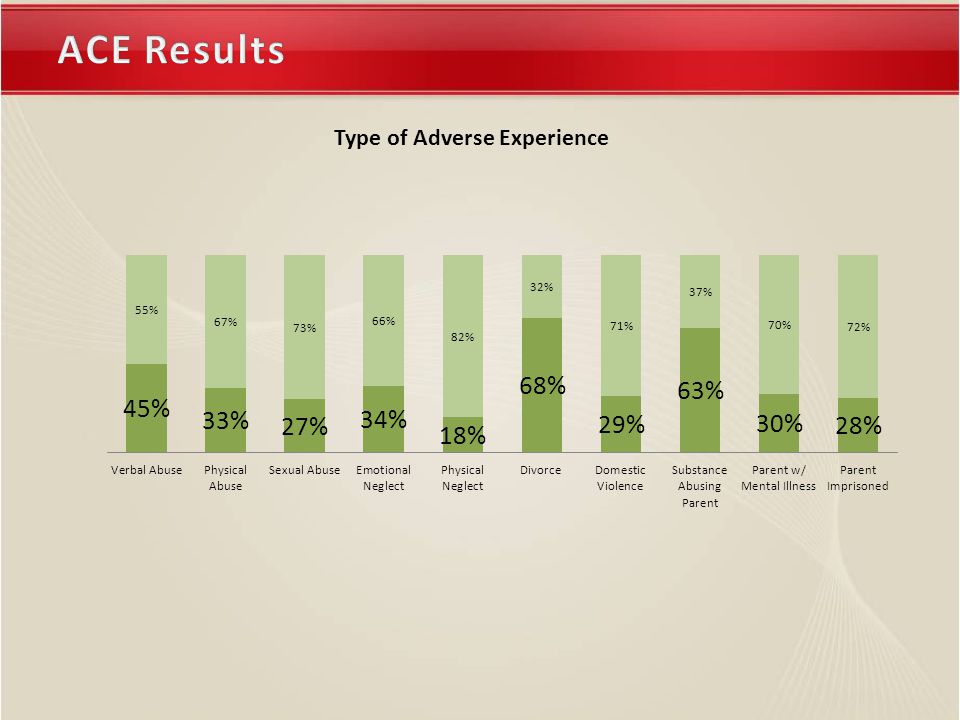
Adverse Childhood Experiences – Measures the extent of exposure from the study’s sample to different types of childhood trauma.

18
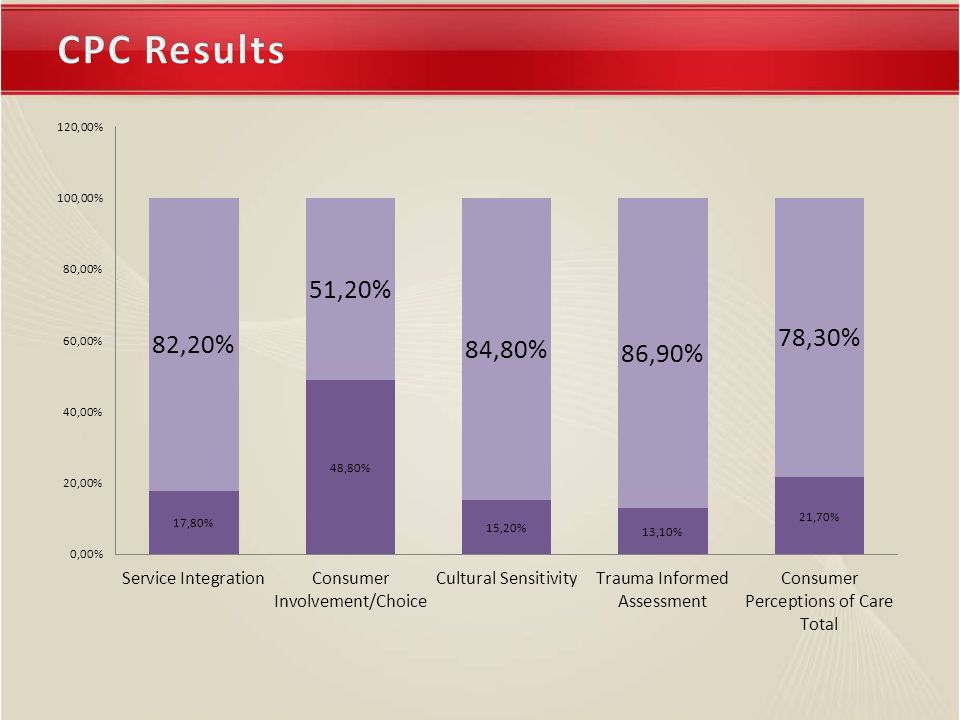
Consumer Perceptions of Care – Measures client’s perceptions of and satisfaction with services for substance abuse, mental health, and trauma related disorders.

19
Community Readiness Model – Guide for assessing readiness and capacity to successfully develop and implement a program on a community/organizational level – Theoretically based on stages of change

20
Developed by Prochaska and DiClemente Change is a process and each person progresses at their own rate through this process Decisions must come ultimately from inside, an internal locus of control, as long-term stable change cannot be externally imposed The stages describe an individual's attitude toward behavior change Precontemplation Contemplation Preparation Action Maintenance Relapse

21
Assess where the person or system is in the change process to determine the appropriate intervention Once you assess where you are in the process then you can what steps you need to take next to get to your goal This research will help us determine our readiness as a division and then each of us will need to personally decide how ready we are to focus on trauma with our population Stages of Change

26
ScaleGenderNMeanSig (2-tail) Service Integration*Male 742.925 0.000 Female 443.432 Consumer Involvement*Male 792.498 0.008 Female 422.901 Cultural Sensitivity*Male 732.808 0.001 Female 393.321 Trauma Informed Assessment*Male 782.944 0.000 Female 443.439 CPC Total*Male 742.820 0.001 Female 413.257 ACE Total*Male 923.304 0.046 Female 464.261 ACE Total (9)Male 922.6957 0.065 Female 463.5000
 Service Integration*Male Female Consumer Involvement*Male Female Cultural Sensitivity*Male Female Trauma Informed Assessment*Male Female CPC Total*Male Female ACE Total*Male Female ACE Total (9)Male Female")
28
Community Efforts 7 Stabilization Community Knowledge of the Efforts 6 Initiation Leadership 6 Initiation Community Climate 7 Stabilization Community Knowledge About the Issue 5 Preparation Resources for Efforts 5 Preparation

29
Community Efforts and Community Climate Level 7 - Stabilization One or two efforts are running, supported by administrators/community decision-makers Programs and activities are viewed as stable Staff are trained and experienced No in-depth evaluation of effectiveness as of yet Climate supports activities

30
Level 7 – Stabilization Goal and Strategies Goal: Stabilize efforts or establish programs Plan events to maintain support for TIC efforts Introduce evaluation results through multiple media sources Review efforts/activity progress on a quarterly basis Maintain business and outside organizational support for the effort/activity Increase and further develop media exposure to reach community, use evaluation data

31
Community Knowledge of the Efforts and Leadership Level 6 – Initiation Information is available to justify the efforts Activity and action is underway but still viewed as a new effort Staff are being trained Great enthusiasm in leaders, as limitations and issues have yet to be met Improved attitude in community members is reflected by continued modest support

32
Level 6 – Initiation Goal and Strategies Goal: Provide Community Specific Information If local data sources are non-existent or unreliable, plan how to begin accurate local data collection Inform other community providers and leaders through multidisciplinary meetings, administrative meetings, in-service trainings, etc. and talk about the progress of your efforts Network with existing resources to enhance your efforts Sponsor or co-sponsor larger community events Plan publicity efforts associated with start up of activity, program, or efforts Begin discussion about basic evaluation efforts

33
Community Knowledge About the Issue and Resources for Efforts Level 5 – Preparation Planning is going on and focuses on details General information about problem and pros and cons of efforts Leadership is active and energetic Resources (people, money, time, etc) are actively being sought Community climate offers modest support
 are actively being sought Community climate offers modest support")
34
Level 5 – Preparation Goal and Strategies Goal: Gather pertinent information Organize and present local statistics, local efforts, and survey information to the community through agency newsletters, emails, etc. (Compile the facts: locals statistics, local stories, emotional cost, consequences to the division, future impact, financial costs, etc) Begin searching for potential funding for resources through state federal and foundation sources Network within your agency to foster support for initiatives
 Begin searching for potential funding for resources through state federal and foundation sources Network within your agency to foster support for initiatives.")
35
Co-occurring initiative has been strong for 10 years at DACCO Have made significant changes in terms of having services available to clients on-site, assessing for comorbidity, making clients’ mental health concerns part of the treatment planning and clinical chart, etc Realization that trauma is at the root of many of the clients’ disorders (both SA and MH)
")
36
Integrating Care

37
Co-Occurring Disorders – Definition – CCISC (Minkoff & Cline) Model Trauma-Informed Care – Components of Trauma Informed Care – System changes Fully Integration Care – Combining Mental Health, Substance Abuse, and Trauma Treatment
 Model Trauma-Informed Care – Components of Trauma Informed Care – System changes Fully Integration Care – Combining Mental Health, Substance Abuse, and Trauma Treatment")
38
People who are diagnosed with both mental health and substance abuse disorders and are, therefore, living with symptoms of both. – Often struggle to cope with past trauma, medical problems, social concerns (i.e., involvement in the child welfare system), criminal justice/legal problems.
, criminal justice/legal problems..")
39
Designed to improve access and implementation of treatment for clients in a holistic manner

40
Welcoming Accessible Integrated Continuous Comprehensive Consumer / Family Oriented

41
Dual diagnosis is an expectation, not an exception Empathic, hopeful, integrated treatment relationships are one of the most important contributors to treatment success in any setting; provision of continuous integrated treatment relationships is an evidence based best practice for individuals with the most severe combinations of psychiatric and substance difficulties

42
All COD clients are not the same (quadrant model) Case management and care must be balanced with empathic detachment, expectation, contracting, consequences, and contingent learning for each client, and in each service setting Quadrant I Less severe MH Less severe SA Quadrant II More severe MH Less severe SA Quadrant III Less severe MH More severe SA Quadrant IV More severe MH More severe SA
 Case management and care must be balanced with empathic detachment, expectation, contracting, consequences, and contingent learning for each client, and in each service setting Quadrant I Less severe MH Less severe SA Quadrant II More severe MH Less severe SA Quadrant III Less severe MH More severe SA Quadrant IV More severe MH More severe SA")
43
When psychiatric and substance disorders coexist, both disorders should be considered primary, and integrated dual (or multiple) primary diagnosis-specific treatment is recommended. “Disease and recovery model” (Minkoff) No single correct intervention for persons with COD (quadrants, diagnoses, level of functioning, stage of change, etc)… Clinical outcomes for persons with COD must also be individualized, based on similar parameters for individualizing treatment interventions
 No single correct intervention for persons with COD (quadrants, diagnoses, level of functioning, stage of change, etc)… Clinical outcomes for persons with COD must also be individualized, based on similar parameters for individualizing treatment interventions.")
44
Change to occur throughout the system of care Tries to use the existing resources or the most efficient use of existing resources Use of evidence-based practices and consensus- based best practices Integrated treatment

45
Co-morbidity Integrated treatment Acknowledgement that readiness varies (which fits best with what modalities?) Continuous relationships with providers Both dx are primary Chronic, relapsing illnesses
 Continuous relationships with providers Both dx are primary Chronic, relapsing illnesses")
46
Create a Committee or sub-committee in your organization to discuss issues of co-occurring disorders Leadership and Change Agents need to prioritize Review the following areas: – Admission Are you currently excluding clients who have substance abuse (if a MH agency) or mental health (if a SA agency) Do you have standard methods of screening for both disorders? – Records Are both diagnoses documented? Do staff include treatment plan objectives for both?

47
– Treatment Quality Enhancements Manualized groups discuss the integration of SA and MH. Use of the stages of change in a systematic way. Program employs drug testing procedures, routinely or as indicated Program participants have access to self-help groups onsite or are regularly transported to groups that specifically address COD (e.g., Dual Recovery / Double Trouble)
.")
48
– Staff Structure Program staff includes persons onsite that have expertise / professional backgrounds in mental health and substance use disorders Human resource policies and written training expectations focus on the acquisition of skills related to the treatment of persons with co-occurring disorders – Program Administration Program Mission Statement specifically welcomes persons with active co-occurring disorders MIS / data entry systems are employed that identify and track services delivered to persons with COD

50
For an organization to be trauma-informed, “all staff…from the receptionist to the direct care workers to the board of directors, must understand how violence impacts the lives of people being served, so that every interaction is consistent with the recovery process and reduces the possibility of re-traumatization (Elliot, 2005, pg 462).”
.")
51
It is when every part of a human service program’s organization, management, and service delivery system is assessed and potentially modified to include an understanding of how trauma affects the life of an individual seeking services. Trauma-informed organizations, programs, and services are based on an understanding of the vulnerabilities or triggers of trauma survivors that traditional service delivery approaches may exacerbate, so that these services and programs can be more supportive to help engage the client.

52
Client Focused: – Client Safety – Trustworthiness – Client Choice – Collaboration – Client Empowerment

53
Relationships Heal…..Relationships Heal….. Family Care Version: Understanding Trauma & Trauma-Informed Care 53

54
Healing Happens in Relationships when…..Healing Happens in Relationships when….. Safety is ensured Connection happens Empathy is present Attunement occurs New skills are taught & practiced There is focus on the positive The helpers remain calm, committed, and are also cared for 54 Family Care Version: Understanding Trauma & Trauma-Informed Care

55
Healing Happens in Environments where…… Physical & psychological safety is ensured Trustworthiness is present There is choice rather than compliance There is collaboration rather than control There is empowerment rather than coercion There is transparency rather than secrecy There is resiliency rather than despair 55 Family Care Version: Understanding Trauma & Trauma-Informed Care

56
Trauma-Informed Care in all SettingsTrauma-Informed Care in all Settings Maximizes survivor’s sense of physical and psychological safety Avoids re-traumatization of the survivor through recognition of triggers Helps survivor to reduce overwhelming emotion 56 Family Care Version: Understanding Trauma & Trauma-Informed Care

57
Trauma-informed services 1.recognize the impact of violence and victimization on development and coping strategies. 2.identify recovery from trauma as a primary goal. 3.employ an empowerment model. 4.strive to maximize women’s/men’s choices and control over her/his recovery. 5.are based in a relational collaboration. Note: taken from Elliot et al., 2005

58
Trauma-informed services create an atmosphere that is respectful of survivors’ need for safety, respect, and acceptance. emphasize women’s strengths, highlighting adaptations over symptoms, resilience over pathology. minimize the possibilities of retraumatization. strive to be culturally competent and to understand each women in the context of her life experiences and cultural background. solicit consumer input and involve consumers in designing and evaluating services. Note: taken from Elliot et al., 2005

59
Supports Clients In: 1.Relationship Building 2.Skills Training 3.Personal Safety

60
Central tenants: relationship building, skill training, and safety. Relationship Building. Trauma informed care treats clients in a way that is understanding of their traumatic experiences rather than focusing on their current “inappropriate” behavior. It is a philosophy that involves asking “What happened to you?” versus “What’s wrong with you?” or “Why do you continue to behave this way?” By respecting the effects traumatic experiences have, rather than focusing on behavior modification, organizations develop strong relationships with clients.

61
Skill Training. Skill building, which leads to increased self- worth, is another important aspect of trauma-informed care. It is important to teach skills, as well as provide them with a safe environment to practice these newly acquired skills. Because skill development equips clients with new options when making decisions in the future, this will hopefully lead them to experience less trauma in the future. Safety. Safety is a huge component of trauma informed care. Clients must feel safe in their treatment and/or residential program. Otherwise, they will not trust and respect staff enough to talk about and discuss “What happened to you?” Safety includes consistency, respect, environment, and trust. It is essential that staff are trained in and understand safety concepts as they relate to trauma informed care.

62
A program that provides Trauma Informed Treatment is made up of the following components, or parts: Treatment and care providers who understand the dynamics of trauma and violence. Staff training about trauma and violence issues, and how to provide treatment and care to individuals who have experienced trauma or violence. Treatment and care providers understand and recognize that the use of seclusion and restraint and the forcing of intramuscular shot medications is re-traumatizing.

63
Assessment of an individual's experiences with trauma and violence. Treatment planning that facilitates consumer choice, control, and participation in: treatment, program/policy development, and evaluation. An environment that is physically and practically designed to avoid re-traumatization. An environment that is safe and nurturing. An environment that is empowering. An environment that is culturally competent.

64
Trauma-specific interventions are designed specifically to address the consequences of trauma in the individual and to facilitate healing. Treatment programs generally recognize the following: The survivor's need to be respected, informed, connected, and hopeful regarding their own recovery The interrelation between trauma and symptoms of trauma (e.g., substance abuse, eating disorders, depression, and anxiety) The need to work in a collaborative way with survivors, family and friends of the survivor, and other human services agencies in a manner that will empower survivors and consumers
 The need to work in a collaborative way with survivors, family and friends of the survivor, and other human services agencies in a manner that will empower survivors and consumers.")
65
Behavioral Health treatment providers must understand the dynamics and impact of trauma on people's lives. Individuals who have experienced trauma in their lives must be involved in the design, delivery and evaluation of treatment services. Providers must be culturally sensitive while incorporating evidence based, best practice, Trauma Informed Treatment models in their programs.

66
Trauma-specific interventions are designed specifically to address the consequences of trauma in the individual and to facilitate healing. Treatment programs generally recognize the following: The survivor's need to be respected, informed, connected, and hopeful regarding their own recovery The interrelation between trauma and symptoms of trauma (e.g., substance abuse, eating disorders, depression, and anxiety) The need to work in a collaborative way with survivors, family and friends of the survivor, and other human services agencies in a manner that will empower survivors and consumers
 The need to work in a collaborative way with survivors, family and friends of the survivor, and other human services agencies in a manner that will empower survivors and consumers.")
67
Develop a trauma team, including trauma survivors, in your facility. Implement evidence based Trauma-Informed Treatment models. Develop a facility culture that is trauma sensitive. Review policies and procedures from a trauma awareness perspective. Assess current treatment environments to eliminate possible re-traumatization.

68
Provide on-going staff training on trauma and its impact on children. Conduct thorough trauma assessments on admission. Include children in all aspects of planning and evaluation. Collaborate with other providers by combining their training money for county or regional training consultants. Provide culturally competent services for persons of all races, colors, religions, sexes, sexual orientations, national origins, disabilities and ages.

70
Have a welcome statement and/or agency mission that welcomes people with co-occurring disorders and trauma. Ensure that even non-clinical staff have knowledge that the people walk through the door are likely to have experienced trauma and be dealing with complicated issues and multiple disorders so we need to be compassionate and patient. Review policies and add language about trauma and COD. Provide trainings in COD and TIC. On-site talent, free local trainings, webinars. Does not have to be expensive. Put on the agenda at committee meetings in agency.

71
When doing bio-psychosocial assessments, ask about childhood/family history. Don’t be afraid to ask about physical, sexual, or psychological abuse – both past and present – in a direct but caring way. Provide group interventions that allow clients to share and hear others’ stories. Seeking Safety is a good example that can be run by a direct care staff and is a safe environment for clients. Ask what the client needs and hopes to achieve in treatment. Ask about prior treatment (mental health, suicidal ideation).
..")
72
Start with baby steps and measurable, achievable goals Change one policy this quarter, add one thing to a form, provide one training

73
What do you see that you need to do to make your system Co-Occurring Capable? What do you need to do to make your system Trauma-Informed? What would be similar? Different?

74
http://www.kenminkoff.com/ Kenneth Minkoff, M.D. & Christie Cline, M.D. COMPASS, CODECAT, CO-FIT Becoming Dual Diagnosis Capable: An Overview (2007) Holly Hills, PhD SAMHSA: http://www.samhsa.gov/nctic/trauma.asp#care http://www.samhsa.gov/nctic/trauma.asp#care Trauma Informed Treatment in Behavioral Health Settings: http://www.olrs.ohio.gov/trauma- informed-treatmenthttp://www.olrs.ohio.gov/trauma- informed-treatment
 Holly Hills, PhD SAMHSA: Trauma Informed Treatment in Behavioral Health Settings: informed-treatmenthttp:// informed-treatment.")
Similar presentations