Download presentation
Presentation is loading. Please wait.

1
Frederick C. Fehl, III MD Dept of Dermatology SCPMG San Diego
PHOTOTHERAPY UPDATE 2009 Frederick C. Fehl, III MD Dept of Dermatology SCPMG San Diego

2
Disclosures I have no known conflicts with any of the products, medications or devices, discussed in this lecture I am receiving no honoraria

3
The Electromagnetic spectrum
Figure shows electromagnetic spectrum divided into the major regions: UVA (UVA I and UVA II ) UVB UVC
 UVB UVC")
4
UV Spectrum UVC ( nm) An arbitrary division was made between UVB and UVC at 290nm because wavelengths shorter then 290nm do not reach the earth’s surface Absorbed by the ozone layer These wavelengths are absorbed by DNA, RNA and proteins of cells and can be lethal to organisms Hence the term germicidal radiation Used in germicidal lamps that emit 254nm

5
UV Spectrum UVB (280-320nm) Strongly erythemogenic (sunburn rays)
Ordinary window glass filters out wavelengths shorter then 320nm There is great variation of the erythemogenic potential within the range: For example 297nm is nearly 100 times more erythemogenic then 313nm radiation even though they are both in the UVB spectrum

6
UV Spectrum UVA ( nm) Divided into two groups: UVA1 ( nm) and UVA2 ( nm) aka as “tanning rays” (tanning parlors emit) Not blocked by window glass unless… UVA radiation is more deeply penetrating (penetrates to the deeper dermis whereas UVB is absorbed by the epidermis This is why I often refer to it as the wrinkle rays

7
UV FACTS Ultraviolet light is “light” we can not see…it’s radiation!
Comprises 5% of terrestrial radiation It spans the region of “light” from 400 to 100nm UV is 7% more intense in the Southern Hemisphere summer than Northern Hemisphere summer UVB comprises 5% of total UV compared to 95% for UVA…but UVB is more biologically active!

8
UV FACTS On a cloudy day…66% of UV gets to ground (75% in the tropics)
In the tropics….a cloudy day get 75% to ground Reflection off the ground is less than 10% except for snow which can reflect 90%! Choppy water more reflective than calm water For every 1,000 feet in elevation, there can be 7% more UV What about the Ozone depletion?

9
“Their may be more ozone depletion in Blue States then Red States”
Red States vs. Blue States Summary 2008 Election Results “Their may be more ozone depletion in Blue States then Red States” Bush, Limbaugh et al

10
UV FACTS UVB inflammation is a delayed effect:
Develops 1-5 hrs after high dose Max effect at 24 hrs fades in 3 days UVA inflammation is immediate (immediate pigment darkening) The UVA “tan” offers little protection compared to UVB UVA penetrates deep to dermis…UVB affects epidermis
 The UVA tan offers little protection compared to UVB. UVA penetrates deep to dermis…UVB affects epidermis.")
11
UV FACTS UVB is considered more carcinogenic: AK, SCC and BCC’s
UVA does have detrimental clinical effects ( e.g., flares autoimmune skin diseases such as lupus etc, has been linked to melanoma) UV can be our friend…Vitamin D, mood elevation UV is immunosuppressive! 70% of UV damage occurs before age 20!
 UV can be our friend…Vitamin D, mood elevation. UV is immunosuppressive! 70% of UV damage occurs before age 20!")
13
Historical Aspects: Phototherapy
Ancient times: Topical exposure to plants containing psoralens + natural sunlight used in Egypt and India to treat vitiligo 1925: Use of crude coal tar and UV radiation was introduced by Goeckerman (Mayo Clinic); became the standard therapy for psoriasis for the next 50 years 1974: PUVA developed (oral regimen) PUVA was quite effective for severe psoriasis 1970’s: broadband UVB also introduced BB UVB IF given in doses that produce a slight erythema could clear mild psoriasis
; became the standard therapy for psoriasis for the next 50 years. 1974: PUVA developed (oral regimen) PUVA was quite effective for severe psoriasis. 1970’s: broadband UVB also introduced. BB UVB IF given in doses that produce a slight erythema could clear mild psoriasis.")
14
Mechanisms of Action of UVL
Reduction in skin proliferation (1st way): UVL is absorbed by chromophore The most important chromophore for UVB is DNA Pyrimidine dimers are formed These toxic photoproducts reduce DNA synthesis Reduction in skin proliferation (2nd way): UVL induces the expression of p53 tumor suppressor gene p53 causes cell cycle arrest and/or apoptosis (cell death)
: UVL is absorbed by chromophore. The most important chromophore for UVB is DNA. Pyrimidine dimers are formed. These toxic photoproducts reduce DNA synthesis. Reduction in skin proliferation (2nd way): UVL induces the expression of p53 tumor suppressor gene. p53 causes cell cycle arrest and/or apoptosis (cell death)")
15
Mechanisms of Action of UVL
Immunosuppressive effects: Induces Interleukin 6 and 10 (sunburn sxs) Langerhans cells (antigen presenting cells) are inhibited by UVL Keratinocytes release IL-1 and 6, Prostaglandins E2 and TNF-α Secretion of these compounds alters the local immune response and may contribute to suppression of disease
 Langerhans cells (antigen presenting cells) are inhibited by UVL. Keratinocytes release IL-1 and 6, Prostaglandins E2 and TNF-α. Secretion of these compounds alters the local immune response and may contribute to suppression of disease.")
16
Action Spectrum The effectiveness of clearing psoriasis plotted against wavelength is defined as the action spectrum of phototherapy It is most desirable to use wavelengths (λ) which are maximally therapeutic and minimally erythemogenic
 which are maximally therapeutic and minimally erythemogenic.")
17
Action Spectrum Studies in the early 1980’s demonstrated that 304 and 313nm had the optimal anti-psoriatic effect within the UVL spectrum: For wavelengths shorter then 295nm, no improvement in psoriasis occurred (remember shorter λ’s are more erythemogenic then therapeutic) 304nm 313nm <295nm Parrish, JA and Jaenicke, KF J Invest Dermatol 1981; 76:
 304nm. 313nm. <295nm. Parrish, JA and Jaenicke, KF J Invest Dermatol 1981; 76:")
18
Action Spectrum The Philips Corp armed with the knowledge regarding the action spectrum of psoriasis develops a fluorescent lamp, TL 01, that emits the optimal narrow band UVB frequency: nm

19
Differences: broadband and narrowband UVB
NB UVB is much less erythemogenic then BB UVB For example: 297nm is nearly 100 times more erythemogenic then 313nm radiation even though they are both in the UVB spectrum Shown to be as effective as PUVA in the treatment of psoriasis Theoretically safer then BB UVB or PUVA

23
UVB Protocol

24
Pre-treatment Check List: UV Therapy
Review the patient’s history (Snapshot)? What disease is the MD treating? Does the patient have co-morbidities that may make UV contraindicated?
 What disease is the MD treating Does the patient have co-morbidities that may make UV contraindicated")
25
Diseases Treated with UV
Psoriasis, psoriasis, and mostly psoriasis Atopic Dermatitis PMLE Pruritus of renal failure Pruritus of liver Disease (e.g., PBC) Scleroderma Idiopathic Pruritus of unknown etiology CTCL Vitiligo Eosinophilic folliculitis of HIV Winter Mood Affective Disorder
 Scleroderma. Idiopathic Pruritus of unknown etiology. CTCL. Vitiligo. Eosinophilic folliculitis of HIV. Winter Mood Affective Disorder.")
26
Pre-treatment Check List: UV Therapy
Review the patient’s history (Snapshot)? What disease is the MD treating? Does the patient have co-morbidities that may make UV contraindicated?
 What disease is the MD treating Does the patient have co-morbidities that may make UV contraindicated")
27
UV AGRAVATED DISEASES PMLE SLE DLE SCLE Solar Urticaria
Xeroderma Pigmentosa Chronic Actinic Dermatitis Cockayne’s Syndrome, Blooms PCT Dermatomyositis Pemphigus Actinic Reticuloid Actinic LP

28
Pre-treatment Check List: UV Therapy
Review the Medications List: Are there any medications listed that are photosensitizing? Will they be using any topical medications in conjunction with their UV therapy? Dovonex Vectical Tazorac Are they taking any oral agents to facilitate their Rx? Acitretin, Isotretinoin

29
Medications known to cause photosensitivity
Every light box facility should have a list such as this one to cross check medications prior to starting UVB Examples include: Zanolli et al textbook: Phototherapy Treatment Protocols (listed in KP protocol) Litt’s Drug Eruption Reference Manual will also list
 Litt’s Drug Eruption Reference Manual will also list.")
30
Pre-treatment Check List: UV Therapy
Labs: Did the MD order any pre-treatment labs? Physical Exam: Do you agree with the MD’s Fitzpatrick skin type assessment? Orders: Do the orders make sense! Right protocol for the disease c/w published protocols Broadband UVB vs. Narrow Band UVB

31
How do you do it? What mj do you start at?
How much do you increase at each visit? What happens if you miss a day, a week or a month? What happens if the patient sunburns? Do you ask if the patient started any new meds?

32
Dosing determination for UVB
Optimal done uses minimal erythema dose determination (MED) for individual patients by intricate phototesting Not typical used by most Dermatologists since it is time consuming and nurse intensive Most Dermatologists use schedules based on the patients skin type
 for individual patients by intricate phototesting. Not typical used by most Dermatologists since it is time consuming and nurse intensive. Most Dermatologists use schedules based on the patients skin type.")
33
Example of MED determination NB UVB

34
UVB Treatment Protocol Using MED

35
Response to Sun Exposure
Fitzpatrick Skin Type Fitzpatrick Skin Type Response to Sun Exposure Examples I Always burns, never tans Fair skin and freckles, blue eyed, Celts II Always sunburns, tans minimally Fair skin, blond hair, blue eyes, Scandinavian III Sometimes sunburns, tans moderately Fair skin, brown hair, brown eyes, unexposed skin is white IV Seldom sunburns, tans easily Light brown skin, dark hair, brown eyes, unexposed skin is tan; Mediterranean, Hispanic V Rarely sunburn, tans profusely Brown skin; Darker Mediterranean, some Asians, Pacific Islander, Indian subcontinent VI Never sunburns, deeply pigmented African Americans

36
Fitzpatrick Skin Type I

37
Fitzpatrick Skin Type II

38
Fitzpatrick Skin Type III

39
Fitzpatrick Skin Type IV

40
Fitzpatrick Skin Type V & Type III

41
Fitzpatrick Skin Type VI

42
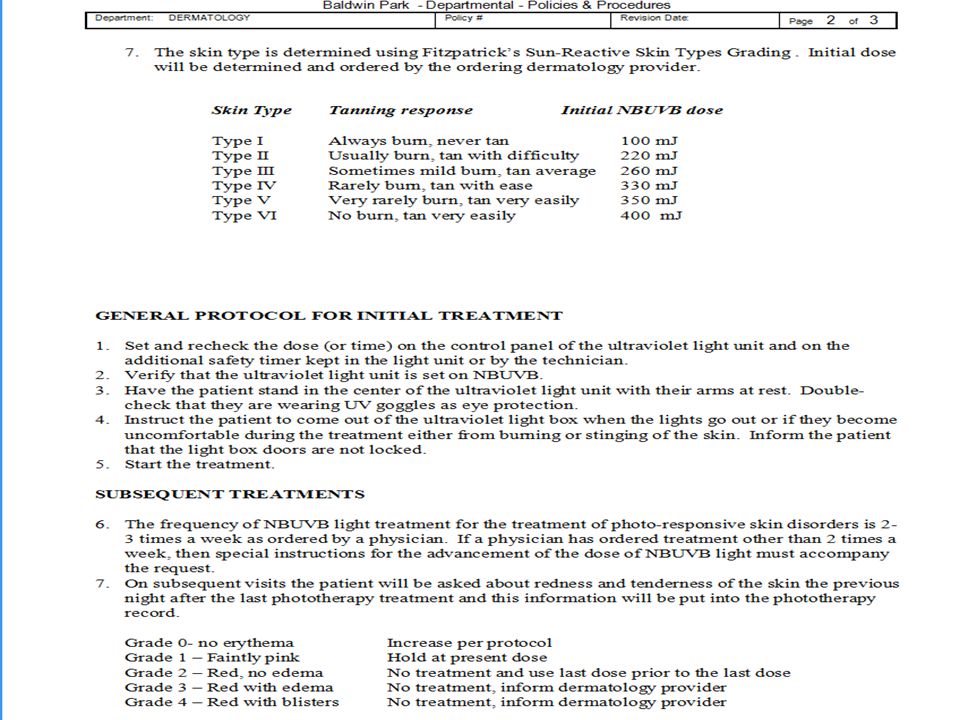
Initial NB UVB Dosing based on Fitzpatrick Skin Type
Tanning Response Initial NB UVB Dose I Always burns, never tans 100 mJ II Usually burn, tans with difficulty 220 mJ III Sometimes mild burn, tan average 260 mJ IV Rarely burns, tans with ease 330 mJ V Very rarely burns, tans very easily 350 mJ VI No burn, tans very easily 400 mJ Kaiser Protocol dated 10/15/07

43
UVB Phototherapy for Psoriasis
Ideally 3X a week (Dr. Koo recommends up to 5X a week) Combination therapy is ideal! Calicipotriene + UVB 2X/week = UVB 3X/week Tazarotene 3X/week added to UVB requires less than ¼ of UVB to achieve 50% PASI Goeckerman, Anthralin, Keratolytics
 Combination therapy is ideal! Calicipotriene + UVB 2X/week = UVB 3X/week. Tazarotene 3X/week added to UVB requires less than ¼ of UVB to achieve 50% PASI. Goeckerman, Anthralin, Keratolytics.")
44
Current Kaiser Recommendations regarding Dose Escalation based on Skin Type for NB UVB
Interval Increase Estimated Dose Goal Maximum Dose (not to exceed) I 15mJ 520 mJ 2000mJ II 25mJ 880 mJ III 40mJ 1040 mJ 3000mJ IV 45mJ 1320 mJ V 60mJ 1400 mJ 5000mJ VI 65mJ 1600 mJ
 I. 15mJ. 520 mJ. 2000mJ. II. 25mJ. 880 mJ. III. 40mJ mJ. 3000mJ. IV. 45mJ mJ. V. 60mJ mJ. 5000mJ. VI. 65mJ mJ.")
45
Key Safety Points …….Burn Unit!!! Type of box: Remember units matter:
NB vs. BB For clinics with multiple boxes even if same light system we assign a pt to a particular box they always use that box even if they have to wait! Remember units matter: 800 milljoules vs. 800 Joules …….Burn Unit!!!

46
Two different boxes with two different input metrics

47
Not all UV light is Equal

48
Key Safety Points Physicians should order the UVB in Health Connect using the units that you will enter into the box (i.e., avoid unit conversion issues: how many millijoules = a joule?)
")
49
my order I then add my smartphrase .FFUVB These units should correspond to what YOU input into that pt’s light box

54
NB UVB Protocols Remember different diseases use different protocols
Vitiligo protocol quite different then psoriasis Atopic dermatitis protocol different then psoriasis (e.g., much lower max dose) Remember the Kaiser Permanente protocol is a quite conservative NB UVB protocol for the treatment of psoriasis imho When in doubt whether the protocol is appropriate for the disease being treated ask the ordering MD to verify!
 Remember the Kaiser Permanente protocol is a quite conservative NB UVB protocol for the treatment of psoriasis imho When in doubt whether the protocol is appropriate for the disease being treated ask the ordering MD to verify!")
55
Thank You!

56
Vitiligo NB UVB Protocol
Treatment frequency is typically twice weekly Start at all patients at 200 mJ/ cm2 Incremental Dosing If skin was pink the previous night and: Pink now: Skip treatment & notify the MD Not Pink now: Treat at same dose If skin was not pink the previous night: Increase by 50 mJ/cm2 Maximum dose is mJ /cm2 Missed Treatments of NBUVB for Vitiligo: 4-7 days 100% (same as last dose) 8-14 days decrease dose by 50% 15-21 days start over
 8-14 days decrease dose by 50% days start over.")
57
Fig. 134.5 Narrowband phototherapy for vitiligo.
Before treatment after 10 mos of NB UVB twice weekly © 2003 Elsevier - Bolognia, Jorizzo and Rapini: Dermatology -

58
What’s New in Phototherapy
Narrow Band UVB 311 UVA – 1 Photodynamic Therapy Blue Light Red Light Excimer Laser New Lasers

59
UV FACTS UV is a discrete, oscillating electromagnetic pulse of energy, E (joules, J) and a wavelength, lambda (nanometres, nm, 10 -9th m), travelling through space at velocity, c (3x10 8th m/s), such that E=hc/lambda, where h= 6.63 X th J/s (Planck’s Constanat).
 and a wavelength, lambda (nanometres, nm, 10 -9th m), travelling through space at velocity, c (3x10 8th m/s), such that E=hc/lambda, where h= 6.63 X th J/s (Planck’s Constanat).")
60
Common Terms Watt (W) = Unit of power
Energy (Joules) = Power (W) x time (sec) Joule (J) = Unit of energy 1000 Millijoules (mJ) = 1 Joule Fluence (Dose) = Energy delivered to a unit area (J/cm2 ) Irradiance = Power delivered to a unit area (W/m2)
 = Power (W) x time (sec) Joule (J) = Unit of energy Millijoules (mJ) = 1 Joule. Fluence (Dose) = Energy delivered to a unit area (J/cm2 ) Irradiance = Power delivered to a unit area (W/m2)")
Similar presentations





>")








 Light? UV Light is very short wave light! –U–UVA 320-400 nm (Nano Meter) –U–UVB 290-320 nm –U–UVB Narrow Band (313 nm) –U–UVC.>")









