Download presentation
Presentation is loading. Please wait.

1
Surviving a Large Scale Organized Hunger Strike at your institution
California Correctional Health Care Services 2011

2
Authors Have No Conflict of Interest Disclosures
Alan Frueh MD Bonnie Gieschen MD Linda Maclachlan Pharm.D Jane Robinson RN Rebecca Yager RD John Zweifler MD Douglas Peterson MD

3
Objectives Distinguish between the handling of an individual hunger strike and a mass hunger strike. Describe the pathophysiology, stages, and risks of starvation. Stratify the risk of refeeding and prescribe an appropriate refeeding diet.

4
Outline CCHCS Policy Highlights Challenges of a Mass Hunger Strike
How it usually works Challenges of a Mass Hunger Strike What we knew and expected-July 2011 HS 1-July 1-July 21, 2011 Lessons learned Mass Hunger Strike Policy HS 2 September 26-October 14, 2011 Starvation and Refeeding Syndrome Stages of Hunger and Starvation Refeeding Risk Stratification Clinical Guidance

5
CCHCS Policy Highlights

6
CCHCS Medical Services Program P & P: Hunger Strike Policy Chapter 22 (2006)
")
7
CCHCS Medical Services Program P & P: Hunger Strike Policy Chapter 22 (2006)
Front loaded with work Intense utilization of resources before most P/I experience adverse effects Inefficient, but manageable for sporadic strikers who are more likely to: Have mental health issues Have individual goals or grievances Respond to early and intense interventions by healthcare and custody.

8
Challenges of a Mass Hunger Strike

9
CCHCS Medical Services Program P & P: Hunger Strike Policy Chapter 22 (2006)
Existing policy poorly adapted to a mass hunger strike which is likely to: Have large numbers of participants Be politically motivated Less likely participant has mental health condition contributing to strike Be organized/pre-planned (food storage) Be pre-announced
 Be pre-announced.")
10
What we knew and expected July 2011
Strike rumors circulated in June 2011 CDCR Intelligence expected: 1000+ strike participants at Pelican Bay State Prison Unknown numbers at CSP Corcoran

11
Limitations with existing policy:
CCHCS medical leadership recognized the limitations of existing policy and the difficulties it created: How to do RN face-face assessments within 2 days How to do full RN daily assessments thereafter How to determine which participants are high risk How to have PCP evaluation within 72 hrs and order labs How to have Mental Health see every participant How to keep track of this many participants

12
Limitations with existing policy:
Initial plans Follow policy whenever possible Fallback to declaring Emergency and following Emergency Incident Command System if needed

13
HS 1: July 1-July 21, 2011 First day 6553 participants 16 sites
Maximum 9,079 participants Challenge was much greater than anticipated

14
July 2011 Strike: Number of participants by Institution (Does not include Out of State)
")
15
Experience July 1-July 21, 2011 Due to large numbers of refusals staff was generally able to follow policy in spite of the large number of strike participants Of the 9079 participants only 143 were deemed Persistent Hunger Strikers defined as: Actively striking > 2 weeks and Had a beginning wt and > one wt recorded during strike Only 8 participants had weight loss > 15 lbs

16
July Strike: Outcome Weight Loss
Weight Lost 7/20/2011 > 20 lbs lost 4 lbs lost lbs lost 29 9.9-0 lbs lost 101 > 0 lbs gained 6 Grand Total 143 Note >7700 participants never had a weight done (refused) Custody did not clear or restrict canteen during HS 1
 Custody did not clear or restrict canteen during HS 1.")
17
July Strike: Outcome Admissions
37 admissions out of 9079 participants 1/3 of these appeared related to lack of intake Most were “Persistent Hunger Strikers” Primary Diagnosis Muscle weakness (generalized) 3 Dehydration 2 Abdominal pain, unspecified site Other disorder metabolism 1 Other disorder eating Except for one patient inmate at PBSP, there was no evidence of refeeding problems at 3 wks.
 3. Dehydration. 2. Abdominal pain, unspecified site. Other disorder metabolism. 1. Other disorder eating. Except for one patient inmate at PBSP, there was no evidence of refeeding problems at 3 wks.")
18
Lessons learned from HS 1
Routine labs are not supported by available data: Especially electrolytes in the first 3 wks Glucose (mild hypoglycemia) can be done by FS UA (does not change management) Labs may remain normal until refeeding begins
 can be done by FS. UA (does not change management) Labs may remain normal until refeeding begins.")
19
Lessons learned from HS 1
Existing Policy not appropriate for a mass event Need a policy covering a large scale strike Identify, evaluate and follow high risk participants (underlying illness, meds, underweight etc.) Institution/provider high risk patient lists Clinically Complex Registry. UHR Mental Health Tracking System for MH patients. Clinical assessments safely delayed until participant has lost 5% body weight (except for high risk persons)
 Institution/provider high risk patient lists. Clinically Complex Registry. UHR. Mental Health Tracking System for MH patients. Clinical assessments safely delayed until participant has lost 5% body weight (except for high risk persons)")
20
Lessons learned from HS 1
Baseline/periodic weights useful if can be obtained: Participants status –risk of adverse events Predicting risk of refeeding (Daily weights are not necessary) The large majority of participants refused weights AND evaluations. Close clinical observation needed for the participants who refuse weight and exam
 The large majority of participants refused weights AND evaluations. Close clinical observation needed for the participants who refuse weight and exam.")
21
Lessons learned from HS 1
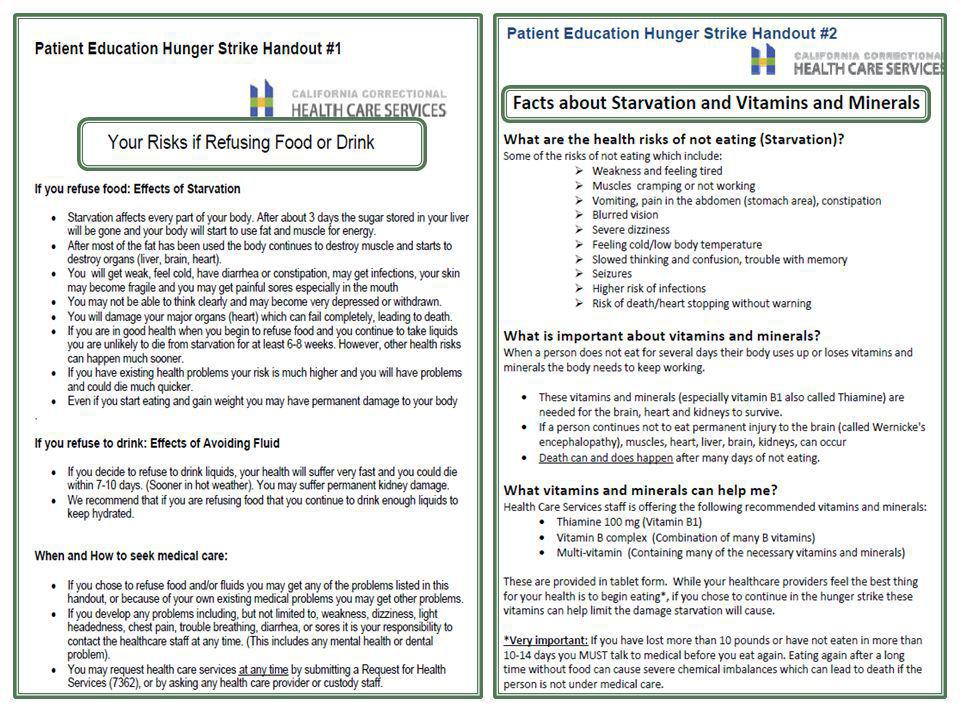
Routine, early AD/POLST completion not useful Time consuming Many participants refused Those who completed chose full resuscitation and Rx Appropriate for participants who have lost significant weight and are at higher risk. Participants need education on responsibility to notify staff of need for health care Participants need education on risks of starvation and refeeding. Patient education hand-outs Documentation of informed consent/effective communication once weight loss documented.

24
Lessons learned from HS 1
Institutions need to stock up on supplies and equipment : Scales (mark them, digital if possible), BP cuffs Oral and intravenous rehydration supplies MVI, thiamine (oral and IV or IM) Pre-printed documentation templates .
, BP cuffs. Oral and intravenous rehydration supplies. MVI, thiamine (oral and IV or IM) Pre-printed documentation templates. .")
25
Lessons learned from HS 1
Literature based clinical guidance useful for staff Role of vitamins/mineral supplements Assessment of risk/management of refeeding Share with ED doc’s if participant transferred out Communication and tracking issues: Daily manual tracking + large # of participants = errors Participants start and stop eating Recognize data limitations due to refusals and initial collection and recording errors do not allow firm conclusions

26
Mass Organized Hunger Strike Policy

27
HS 2: Sept. 26-Oct. 17, 2011 Custody had different approach:
Treated HS 2 as a “disturbance” Separated HS leaders from rest of population Removed food and canteen items from identified participants’ cells Disallowed canteen privileges (except for hygiene items) for participants Coordinated tracking with medical via SharePoint site.
 for participants. Coordinated tracking with medical via SharePoint site.")
28
HS 2: Experience with new policy
High numbers but: Resources focused more appropriately Improved organization and communication Less staff and leadership stress and fatigue

29
HS 2: Experience with new policy

30
HS 2: Experience with new policy
Weight loss: HS 1 vs HS 2 0-9.9 lbs lbs lbs > 20 lbs HS 1 10 29 4 HS 2 417 90 40 18

31
HS 2: Experience with new policy
Larger numbers of weights recorded probably due to: Greater number of inmates consenting to being weighed Improved tracking on the SharePoint Increased weight loss could be due to: More weights taken Participants did not have access to stored food this time No deaths or serious morbidity occurred

32
Lessons learned-HS 2 Continue to improve shared tracking
Removal/restriction of canteen helpful Dis-incentive to participants More certain of actual intake, clinically more predicable Mass HS Policy needs improvement How best to monitor large #’s of participants Time vs Weight vs Both? Regular direct observation of refusers? How best to manage starvation- when start vitamins? How best to address refeeding Determine risk and control initial intake Institution and HQ meeting to revise… stay tuned…
![]()
33
Starvation and Refeeding Syndrome

34
Effects of Malnutrition

35
Stages of Hunger Strike
4-7 days Muscle protein metabolized to glucose Depletion of K+ Phos, Mg++ 8-14 days Risk of refeeding syndrome begins Day 10 1-3 days Use up glycogen

36
Stages of Hunger Strike
35-42 d “oculo-motor “ nystagmus diplopia trouble swallowing extreme vertigo vomiting converging strabismus > 42 days Loss of > 30% body wt life-threatening increased confusion trouble concentrating somnolent state incoherent arrhythmias 15-18 d ataxia difficulty standing bradycardia orthostasis “mental sluggishness” sensation of cold weakness

37
Clinical Interventions- Early
Initiate applicable CCHCS Hunger Strike Policy Baseline weight (same scale/digital if possible) Identify high risk participants Refer as appropriate to Mental Health Review medication lists Stop nonessential mediations Stop antacids (interfere with phosphate absorption) Stop diuretics if possible Offer educational information Document refusals
 Identify high risk participants. Refer as appropriate to Mental Health. Review medication lists. Stop nonessential mediations. Stop antacids (interfere with phosphate absorption) Stop diuretics if possible. Offer educational information. Document refusals.")
38
Clinical Interventions
Offer patients: Thiamine 100 mg po daily B complex 1 po daily Multi-vitamin (e.g. Tab-a-vite) one po daily Encourage 1.5L or more /day fluid intake Watch more closely if refusing fluids If clinically significant dehydration offer: Oral rehydration Pedialyte- (IV only if refuses) Symptomatic hypoglycemia treat as clinically indicated: Food, LNS, Glucose gel, D50 IV Fall precautions Before voluntary refeeding assess risk
 one po daily. Encourage 1.5L or more /day fluid intake. Watch more closely if refusing fluids. If clinically significant dehydration offer: Oral rehydration Pedialyte- (IV only if refuses) Symptomatic hypoglycemia treat as clinically indicated: Food, LNS, Glucose gel, D50 IV. Fall precautions. Before voluntary refeeding assess risk.")
39
Refeeding Syndrome Definition:
Wide spectrum of biochemical abnormalities and clinical consequences Hypophosphatemia is the adopted surrogate marker but not pathognomonic.

40
Refeeding Syndrome Physiology
When a malnourished person begins to eat: Glucose enters blood Insulin follows Glucose takes K+, P, Mg++ into the cells Increased demand for thiamine (cofactor cellular enzymatic reactions) How to recognize and respond to refeeding syndrome: Yantis, Mary Ann; Velander, Robyn Nursing2011 Critical Care. 4(3):14-20, May 2009.
 How to recognize and respond to refeeding syndrome: Yantis, Mary Ann; Velander, Robyn Nursing2011 Critical Care. 4(3):14-20, May")
41
Refeeding Syndrome Clinical Manifestations: Symptoms: Unpredictable
Deterioration can be rapid May occur late. Variable Mild derangements may have no symptoms. Spectrum: N/V, lethargyrespiratory insufficiency, cardiac failure, hypotension, arrhythmias, delirium, coma death.

42
Evaluation and Management
Clinical Evaluation: Screening exam, review medications Risk assessment based on: BMI, wt loss , length of fasting What if no baseline weight? ECG (if irregular pulse, abnormal HR, ↓ K+ or Phos) If cardiac abnormalities-monitoring recommended
 If cardiac abnormalities-monitoring recommended.")
43
Evaluation and Management
Clinical Evaluation: (cont) Labs: Baseline Phos +, Mg + +, Ca + +, K +, Na +, urea, Cr before refeeding During refeeding monitor electrolytes daily (as indicated based upon refeeding risk assessment) Life-threatening changes usually seen in the first 3 days Watch fluid intake/output and weight If gain > ½ lb per day or 3.3 lbs/wk likely fluid retention
 Labs: Baseline Phos +, Mg + +, Ca + +, K +, Na +, urea, Cr. before refeeding. During refeeding monitor electrolytes daily (as indicated based upon refeeding risk assessment) Life-threatening changes usually seen in the first 3 days. Watch fluid intake/output and weight. If gain > ½ lb per day or 3.3 lbs/wk likely fluid retention.")
44
Risk Stratification: adapted from

45
Risk Stratification Negligible risk:
Fasting < 7-9 days, with BMI>18.5 kg/m2 Modest risk: Any one of the following criteria: a BMI > 16 but <18.5 kg/m2 or loss of >10% body weight (but < 15%) High risk: (either) Major risk factors (any one of the following) a BMI <16 kg/m2 weight loss >15% Low K+, Mg++,Phos Lesser risk factors: (two or more of the following) a BMI <18.5 kg/m2 weight loss >10% H/O ETOH, co-morbid/meds Extreme risk: More than one of the following: BMI <16 kg/m2 Low K+, Mg++, Phos No food > 21 days ChemoRx, other significant comorbidity
 High risk: (either) Major risk factors (any one of the following) a BMI <16 kg/m2. weight loss >15% Low K+, Mg++,Phos. Lesser risk factors: (two or more of the following) a BMI <18.5 kg/m2. weight loss >10% H/O ETOH, co-morbid/meds. Extreme risk: More than one of the following: BMI <16 kg/m2. Low K+, Mg++, Phos. No food > 21 days. ChemoRx, other significant comorbidity.")
46
Refeeding Guidance adapted…

47
Refeeding Risk- Modest
Level of Risk Management of Patient Negligible risk: Fasting < 7-9 days, with BMI>18.5 kg/m2 Eat and drink freely and no monitoring is necessary. Watch hydration if have not been taking fluids Modest risk: BMI > 16 but <18.5 kg/m2 or loss of >10% body weight (but < 15%) Strongly consider giving thiamine 100 mg prior to refeeding Add to D5NS or given IM. <20 kcals/kg/day for the first 2 days CDCR Heart Healthy Diet tray (Provides 2750 kcal) ½ of each meal tray the first 2 days Fluid limited to around 30ml/kg/day (Example 170 lb man= 2310 ml/day) Blood tests above before refeeding starts Repeated at approximately 24 and 48 hours of refeeding Daily multi-vitamin and trace element supplement.
 Strongly consider giving thiamine 100 mg prior to refeeding. Add to D5NS or given IM. <20 kcals/kg/day for the first 2 days. CDCR Heart Healthy Diet tray (Provides 2750 kcal) ½ of each meal tray the first 2 days. Fluid limited to around 30ml/kg/day. (Example 170 lb man= 2310 ml/day) Blood tests above before refeeding starts. Repeated at approximately 24 and 48 hours of refeeding. Daily multi-vitamin and trace element supplement.")
48
Refeeding with “Food”

49
Refeeding Risk- High Level of Risk Management of Patient High risk:
Major risk factors : (any one of the following) a BMI <16 kg/m2 weight loss >15% Low K+, Mg++,Phos Lesser risk factors: (two or more of the following) a BMI <18.5 kg/m2 weight loss >10% H/O ETOH, co-morbid/meds Refeeding in clinical setting with careful observation ( In most cases community hospital) Monitor closely-transfer to higher level of care if: K+ <3.0 mmol/l Mg++ <0.5 mmol/l Phos <0.5 mmol/l Strongly consider Phos, K+, Mg++ even if baseline ok Strongly consider thiamine 100 mg prior to refeeding. Intake 10 kcal/kg/day for the first 24 hours, taking either: CDCR Heart Healthy or Carnation Instant Breakfast Lactose Free Increase by 5-10 kcal/kg/day. Fluid < 30ml/kg/day. (zero” fluid balance x 1 wk) Blood test daily x 1 week (LFT’s 2x/wk) Daily multi-vitamin and trace element supplement.
 a BMI <16 kg/m2. weight loss >15% Low K+, Mg++,Phos. Lesser risk factors: (two or more of the following) a BMI <18.5 kg/m2. weight loss >10% H/O ETOH, co-morbid/meds. Refeeding in clinical setting with careful observation ( In most cases community hospital) Monitor closely-transfer to higher level of care if: K+ <3.0 mmol/l. Mg++ <0.5 mmol/l. Phos <0.5 mmol/l. Strongly consider Phos, K+, Mg++ even if baseline ok. Strongly consider thiamine 100 mg prior to refeeding. Intake 10 kcal/kg/day for the first 24 hours, taking either: CDCR Heart Healthy or. Carnation Instant Breakfast Lactose Free. Increase by 5-10 kcal/kg/day. Fluid < 30ml/kg/day. (zero fluid balance x 1 wk) Blood test daily x 1 week (LFT’s 2x/wk) Daily multi-vitamin and trace element supplement.")
50
Refeeding Risk- Extreme
Level of Risk Management of Patient Extreme risk: More than one of the following: BMI <16 kg/m2 weight loss >15% Low K+, Mg++, Phos No food > 21 days H/O ETOH, co-morbid/meds ChemoRx, other significant comorbidity Admit to hospital Restore volume, fluid balance and electrolytes. IV Thiamine Supplementation of K+, Phos, Mg++ 5 kcal/kg/day for Day 1 NG continuous or intermittent LNS if can’t eat Carnation Instant Breakfast Lactose or If pt can eat CDCR Heart Healthy diet Monitoring of the ECG for at least the first 48 hours Blood test daily x 1 week (LFT’s 2x/wk) Normal labs- can have TOTAL body depletion low Even if high or renal failure may need supplements If low need to give supplements WITH low levels of feeding Once po well established begin daily MVI & trace element
 Normal labs- can have TOTAL body depletion low. Even if high or renal failure may need supplements. If low need to give supplements WITH low levels of feeding. Once po well established begin daily MVI & trace element.")
51
Refeeding with LNS

52
Questions? Terra.Rasmussen@cdcr.ca.gov
For copies of Policy, Clinical Guidance and Decision Support

Similar presentations




>")















