Download presentation
Presentation is loading. Please wait.

1
CFS/ME Clinical and Research Network and Collaboration Esther Crawley

2
Formation of the CCRNC 1999 Research Network Forum researchers and clinicians - 50 members 2004 Collaborative 13 Centres, 37 adult teams, 11 paediatric teams 2009: Collaborative Increased number of clinical teams / patients seen Active work streams 2009: Research network 250 members Active training programme 1999 Research Network Forum researchers and clinicians - 50 members 2004 Collaborative 13 Centres, 37 adult teams, 11 paediatric teams 2009: Collaborative Increased number of clinical teams / patients seen Active work streams 2009: Research network 250 members Active training programme

3
CCRNC 2007: Joint meeting 2009: Merged to form CCRNC Constitution Combined Executive Increasing number of members 2007: Joint meeting 2009: Merged to form CCRNC Constitution Combined Executive Increasing number of members

4
AIM The CCRNC is a multidisciplinary organisation which exists to promote and support the delivery of evidenced based treatment for children, young people and adults with CFS/ME throughout the UK.

5
Objectives 2.2.1 To champion evidence-based approaches to the treatment of CFS/ME, such as those provided in the NICE guidelines 2.2.2 To provide a forum for the monitoring and dissemination of new evidence for the management of CFS/ME as it emerges 2.2.3 To advocate for excellence in the provision of, and for equity of access to, clinical services for children, young people and adults with CFS/ME 2.2.4 To support the delivery of services and to enable services to maintain standards of care in the treatment of CFS/ME as set out in the NICE guidelines 2.2.1 To champion evidence-based approaches to the treatment of CFS/ME, such as those provided in the NICE guidelines 2.2.2 To provide a forum for the monitoring and dissemination of new evidence for the management of CFS/ME as it emerges 2.2.3 To advocate for excellence in the provision of, and for equity of access to, clinical services for children, young people and adults with CFS/ME 2.2.4 To support the delivery of services and to enable services to maintain standards of care in the treatment of CFS/ME as set out in the NICE guidelines

6
Objectives (2) 2.2.5 To use clinical expertise and evidence to influence and inform healthcare policy 2.2.6 To promote, facilitate and provide training for clinicians and researchers from all disciplines involved in the diagnosis and treatment of CFS/ME 2.2.7 To foster research collaborations and communication between clinicians, researchers, professional bodies and charities 2.2.5 To use clinical expertise and evidence to influence and inform healthcare policy 2.2.6 To promote, facilitate and provide training for clinicians and researchers from all disciplines involved in the diagnosis and treatment of CFS/ME 2.2.7 To foster research collaborations and communication between clinicians, researchers, professional bodies and charities
 To use clinical expertise and evidence to influence and inform healthcare policy To promote, facilitate and provide training for clinicians and researchers from all disciplines involved in the diagnosis and treatment of CFS/ME To foster research collaborations and communication between clinicians, researchers, professional bodies and charities To use clinical expertise and evidence to influence and inform healthcare policy To promote, facilitate and provide training for clinicians and researchers from all disciplines involved in the diagnosis and treatment of CFS/ME To foster research collaborations and communication between clinicians, researchers, professional bodies and charities")
7
Objectives (3) 2.2.8 To facilitate patient involvement in the development of evidence-based services and to promote patient centred care. To foster co-operation and collaboration with teams, charities and individuals that share these principles 2.2.9 To encourage and facilitate the systematic and rigorous audit, benchmarking and evaluation of CFS/ME assessment, treatment and services. 2.2.8 To facilitate patient involvement in the development of evidence-based services and to promote patient centred care. To foster co-operation and collaboration with teams, charities and individuals that share these principles 2.2.9 To encourage and facilitate the systematic and rigorous audit, benchmarking and evaluation of CFS/ME assessment, treatment and services.

8
Work streams Training Patient participation Research Minimum Data Set Implementation Pod: information resource Training Patient participation Research Minimum Data Set Implementation Pod: information resource

9
Patient & Carer involvement The CCRNC Executive will have no less than two and not more than four patient/carer members….. The patient or carer will be involved in work streams The CCRNC Executive will invite no more than four people drawn from National UK CFS/ME organisations which explicitly support the aims and constitution of the organisation to sit on the Executive committee as either observers or members The CCRNC Executive will have no less than two and not more than four patient/carer members….. The patient or carer will be involved in work streams The CCRNC Executive will invite no more than four people drawn from National UK CFS/ME organisations which explicitly support the aims and constitution of the organisation to sit on the Executive committee as either observers or members

10
Benchmarking services Constitution Largest longitudinal cohort in the world Constitution Largest longitudinal cohort in the world

11
National Outcomes Dataset (NOD) All teams: Minimum Data set allow audit and bench marking MDS: demographic, markers of severity, goal, employment and education Assessment and follow up 22 teams contributing (> 3000 new per year) All teams: Minimum Data set allow audit and bench marking MDS: demographic, markers of severity, goal, employment and education Assessment and follow up 22 teams contributing (> 3000 new per year)
 All teams: Minimum Data set allow audit and bench marking MDS: demographic, markers of severity, goal, employment and education Assessment and follow up 22 teams contributing (> 3000 new per year) All teams: Minimum Data set allow audit and bench marking MDS: demographic, markers of severity, goal, employment and education Assessment and follow up 22 teams contributing (> 3000 new per year)")
12
What do we want?

13
We all want Excellent services Treatment that works Accessibility for all including children and severely affected Excellent services Treatment that works Accessibility for all including children and severely affected

14
What do we need Research into causes and treatment Benchmarking and audit of services Increased accessibility Research into causes and treatment Benchmarking and audit of services Increased accessibility

15
Bench marking & APPG

17
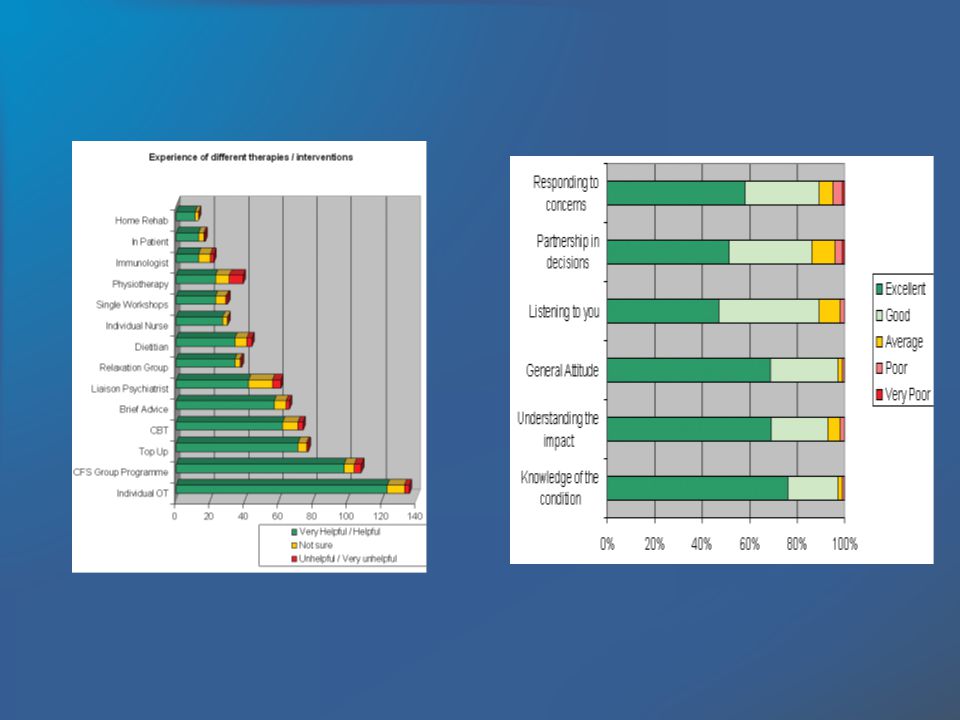
1.I feel that the professionals who saw me listened to me, 2. It was easy to talk to the professionals who saw me, 3. I was treated well by the professionals who saw me, 4. My views and worries were taken seriously

18
Improved a great deal/ moderately improved (41%) Improved Slightly (22%) Stayed the same (27%)
 Improved Slightly (22%) Stayed the same (27%)")
19
My referral to the CFS/ME service has been a godsend. I wasnt looking for a miracle cure from this clinic and I think that is possibly the right attitude to have because there is no miracle cure. However, it has provided me a real lifeline in giving me belief that I wasnt going mad nor was the illness in my head (unlike my unsupportive GP) and my OT really seemed to understand the condition. Her advice has proved very helpful. Also, my meeting with the dietician was very productive. I absolutely cannot fault the service I received/receive. The support of the service has helped me to go from being nearly housebound to back to work. I had a great feeling of relief when I came to the service because I had a formal diagnosis by a person who is fully informed about the condition. I found my sessions essential – I do not think I would have been able to cope alone without the support given. It was helpful being able to discuss my concerns with a knowledgeable person, we were able to work together towards a recovery programme that was suitable for me. I am so pleased with the service provided and I wish I had found out about the CFS ward when I first got ME. My quality of life would have been better and I would not have been thinking for the past 9 year that it was all in my head. Every aspect of the treatment I received from the CFS Clinic was really helpful, kind, understanding, thoughtful and practical My referral to the CFS/ME service has been a godsend. I wasnt looking for a miracle cure from this clinic and I think that is possibly the right attitude to have because there is no miracle cure. However, it has provided me a real lifeline in giving me belief that I wasnt going mad nor was the illness in my head (unlike my unsupportive GP) and my OT really seemed to understand the condition. Her advice has proved very helpful. Also, my meeting with the dietician was very productive. I absolutely cannot fault the service I received/receive. The support of the service has helped me to go from being nearly housebound to back to work. I had a great feeling of relief when I came to the service because I had a formal diagnosis by a person who is fully informed about the condition. I found my sessions essential – I do not think I would have been able to cope alone without the support given. It was helpful being able to discuss my concerns with a knowledgeable person, we were able to work together towards a recovery programme that was suitable for me. I am so pleased with the service provided and I wish I had found out about the CFS ward when I first got ME. My quality of life would have been better and I would not have been thinking for the past 9 year that it was all in my head. Every aspect of the treatment I received from the CFS Clinic was really helpful, kind, understanding, thoughtful and practical
 and my OT really seemed to understand the condition. Her advice has proved very helpful. Also, my meeting with the dietician was very productive. I absolutely cannot fault the service I received/receive. The support of the service has helped me to go from being nearly housebound to back to work. I had a great feeling of relief when I came to the service because I had a formal diagnosis by a person who is fully informed about the condition. I found my sessions essential – I do not think I would have been able to cope alone without the support given. It was helpful being able to discuss my concerns with a knowledgeable person, we were able to work together towards a recovery programme that was suitable for me. I am so pleased with the service provided and I wish I had found out about the CFS ward when I first got ME. My quality of life would have been better and I would not have been thinking for the past 9 year that it was all in my head. Every aspect of the treatment I received from the CFS Clinic was really helpful, kind, understanding, thoughtful and practical My referral to the CFS/ME service has been a godsend. I wasnt looking for a miracle cure from this clinic and I think that is possibly the right attitude to have because there is no miracle cure. However, it has provided me a real lifeline in giving me belief that I wasnt going mad nor was the illness in my head (unlike my unsupportive GP) and my OT really seemed to understand the condition. Her advice has proved very helpful. Also, my meeting with the dietician was very productive. I absolutely cannot fault the service I received/receive. The support of the service has helped me to go from being nearly housebound to back to work. I had a great feeling of relief when I came to the service because I had a formal diagnosis by a person who is fully informed about the condition. I found my sessions essential – I do not think I would have been able to cope alone without the support given. It was helpful being able to discuss my concerns with a knowledgeable person, we were able to work together towards a recovery programme that was suitable for me. I am so pleased with the service provided and I wish I had found out about the CFS ward when I first got ME. My quality of life would have been better and I would not have been thinking for the past 9 year that it was all in my head. Every aspect of the treatment I received from the CFS Clinic was really helpful, kind, understanding, thoughtful and practical.")
20
The Future Strengths Weaknesses Opportunities Threats Strengths Weaknesses Opportunities Threats

21
Strengths Research: Largest cohort in the world Centralised outcome data (> 3000 patients per year) Evaluation of services Working together: 600 clinicians and researchers MRC, NIHR and Welcome Patient & Carer reps Charity membership Research: Largest cohort in the world Centralised outcome data (> 3000 patients per year) Evaluation of services Working together: 600 clinicians and researchers MRC, NIHR and Welcome Patient & Carer reps Charity membership
 Evaluation of services Working together: 600 clinicians and researchers MRC, NIHR and Welcome Patient & Carer reps Charity membership Research: Largest cohort in the world Centralised outcome data (> 3000 patients per year) Evaluation of services Working together: 600 clinicians and researchers MRC, NIHR and Welcome Patient & Carer reps Charity membership")
22
Current CCRNC research Appendix 3: List of current research studies being carried out by members of the CCRNC 1. Gene expression in CFS 2. Qualitative impact of CFS on young people 3. Cognitive factors and levels of adjustment 4. Changes in cognitive processes and changes in outcome 3. Development of an activity pacing questionnaire 4. Relation between changes in physical activity and treatment outcome 5. Orthostatic Training in Chronic Fatigue Syndrome; A Randomised Placebo-Controlled Trial 6. Defining the prevalence of autonomic dysfunction and its consequences in ME/CFS – a clinical cohort study 9. Longitudinal Cohort Study to determine the Prevalence of Autonomic Dysfunction and Relationship with Outcome in Patients with Myalgic encephalitis (ME)/ Chronic Fatigue Syndrome (CFS). 10 Examining structural and functional abnormalities of brain, heart and muscle using MRI in those with CFS/ME 11. Multi-site peripheral pulse assessment of postural vasomotor reflexes 12. Non-invasive fluorescence spectroscopy measurement of skin tryptophan Appendix 3: List of current research studies being carried out by members of the CCRNC 1. Gene expression in CFS 2. Qualitative impact of CFS on young people 3. Cognitive factors and levels of adjustment 4. Changes in cognitive processes and changes in outcome 3. Development of an activity pacing questionnaire 4. Relation between changes in physical activity and treatment outcome 5. Orthostatic Training in Chronic Fatigue Syndrome; A Randomised Placebo-Controlled Trial 6. Defining the prevalence of autonomic dysfunction and its consequences in ME/CFS – a clinical cohort study 9. Longitudinal Cohort Study to determine the Prevalence of Autonomic Dysfunction and Relationship with Outcome in Patients with Myalgic encephalitis (ME)/ Chronic Fatigue Syndrome (CFS). 10 Examining structural and functional abnormalities of brain, heart and muscle using MRI in those with CFS/ME 11. Multi-site peripheral pulse assessment of postural vasomotor reflexes 12. Non-invasive fluorescence spectroscopy measurement of skin tryptophan
/ Chronic Fatigue Syndrome (CFS). 10 Examining structural and functional abnormalities of brain, heart and muscle using MRI in those with CFS/ME 11. Multi-site peripheral pulse assessment of postural vasomotor reflexes 12. Non-invasive fluorescence spectroscopy measurement of skin tryptophan Appendix 3: List of current research studies being carried out by members of the CCRNC 1. Gene expression in CFS 2. Qualitative impact of CFS on young people 3. Cognitive factors and levels of adjustment 4. Changes in cognitive processes and changes in outcome 3. Development of an activity pacing questionnaire 4. Relation between changes in physical activity and treatment outcome 5. Orthostatic Training in Chronic Fatigue Syndrome; A Randomised Placebo-Controlled Trial 6. Defining the prevalence of autonomic dysfunction and its consequences in ME/CFS – a clinical cohort study 9. Longitudinal Cohort Study to determine the Prevalence of Autonomic Dysfunction and Relationship with Outcome in Patients with Myalgic encephalitis (ME)/ Chronic Fatigue Syndrome (CFS). 10 Examining structural and functional abnormalities of brain, heart and muscle using MRI in those with CFS/ME 11. Multi-site peripheral pulse assessment of postural vasomotor reflexes 12. Non-invasive fluorescence spectroscopy measurement of skin tryptophan.")
23
13. Thermoregulatory dysfunction assessments using whole body thermography 14. What is the prevalence of CFS/ME at age 13: ALPSAC 15. Analysis of the predictors of CFS/ME in children using ALPSAC 16. Outcome in children with CFS/ME - analysis of longitudinal cohort 17. Early intervention to prevent CFS/ME 18. Comparison of service models in the NHS 19. A survey of health needs and experiences of people accessing an NHS Service. 20. Grounded theory study on concepts of use of time, tempo and temporality in CFS/ME. 21. The PACE trial (Pacing, graded Activtiy, and CBT for CFS: a randomised Evaluation)(www.pacetrial.org) 22. Chronic Fatigue and Ethnicity: prevalence, explanatory models and service use in a nationally representative sample of six ethnic groups. 23. Cytokine responses to exercise and activity in patients with the chronic fatigue syndrome: proof of principle study 24. General and specific risk markers and preventive factors for both chronic fatigue and irritable bowel syndromes in a birth cohort. 13. Thermoregulatory dysfunction assessments using whole body thermography 14. What is the prevalence of CFS/ME at age 13: ALPSAC 15. Analysis of the predictors of CFS/ME in children using ALPSAC 16. Outcome in children with CFS/ME - analysis of longitudinal cohort 17. Early intervention to prevent CFS/ME 18. Comparison of service models in the NHS 19. A survey of health needs and experiences of people accessing an NHS Service. 20. Grounded theory study on concepts of use of time, tempo and temporality in CFS/ME. 21. The PACE trial (Pacing, graded Activtiy, and CBT for CFS: a randomised Evaluation)(www.pacetrial.org) 22. Chronic Fatigue and Ethnicity: prevalence, explanatory models and service use in a nationally representative sample of six ethnic groups. 23. Cytokine responses to exercise and activity in patients with the chronic fatigue syndrome: proof of principle study 24. General and specific risk markers and preventive factors for both chronic fatigue and irritable bowel syndromes in a birth cohort.
( 22. Chronic Fatigue and Ethnicity: prevalence, explanatory models and service use in a nationally representative sample of six ethnic groups. 23. Cytokine responses to exercise and activity in patients with the chronic fatigue syndrome: proof of principle study 24. General and specific risk markers and preventive factors for both chronic fatigue and irritable bowel syndromes in a birth cohort. 13. Thermoregulatory dysfunction assessments using whole body thermography 14. What is the prevalence of CFS/ME at age 13: ALPSAC 15. Analysis of the predictors of CFS/ME in children using ALPSAC 16. Outcome in children with CFS/ME - analysis of longitudinal cohort 17. Early intervention to prevent CFS/ME 18. Comparison of service models in the NHS 19. A survey of health needs and experiences of people accessing an NHS Service. 20. Grounded theory study on concepts of use of time, tempo and temporality in CFS/ME. 21. The PACE trial (Pacing, graded Activtiy, and CBT for CFS: a randomised Evaluation)( 22. Chronic Fatigue and Ethnicity: prevalence, explanatory models and service use in a nationally representative sample of six ethnic groups. 23. Cytokine responses to exercise and activity in patients with the chronic fatigue syndrome: proof of principle study 24. General and specific risk markers and preventive factors for both chronic fatigue and irritable bowel syndromes in a birth cohort..")
24
25. Service evaluation on practice nurses knowledge of the NICE guidelines for CFS/ME primary care 26. T and B Memory cell function and NK activity. Along with Dr XX at XX Hospital Med School investigation genetic alterations in CFS and possible infectious agents. 27. Systematic literature review investigating the effectiveness of videoconferencing as a means of delivering therapy to CFS/ME patients 28. Scoping exercise investigating the feasibility of delivering therapy via in-home desktop videoconferencing to CFS/ME patients in North Cumbria 29. Pilot trial investigating the feasibility of delivering therapy via in-home desktop videoconferencing to CFS/ME patients in North Cumbria 30. Pilot user-led qualitative project on Users Perspectives of a Mindfulness Approach within a CFS/ ME service 31. Cochrane review of pharmacological treatments for CFS 32. Actigraphy as a measure of sleep quality in CFS 33. Post-exertional malaise in CFS/depression/MS 34. Attitudes to CFS amongst medical students and other student groups 25. Service evaluation on practice nurses knowledge of the NICE guidelines for CFS/ME primary care 26. T and B Memory cell function and NK activity. Along with Dr XX at XX Hospital Med School investigation genetic alterations in CFS and possible infectious agents. 27. Systematic literature review investigating the effectiveness of videoconferencing as a means of delivering therapy to CFS/ME patients 28. Scoping exercise investigating the feasibility of delivering therapy via in-home desktop videoconferencing to CFS/ME patients in North Cumbria 29. Pilot trial investigating the feasibility of delivering therapy via in-home desktop videoconferencing to CFS/ME patients in North Cumbria 30. Pilot user-led qualitative project on Users Perspectives of a Mindfulness Approach within a CFS/ ME service 31. Cochrane review of pharmacological treatments for CFS 32. Actigraphy as a measure of sleep quality in CFS 33. Post-exertional malaise in CFS/depression/MS 34. Attitudes to CFS amongst medical students and other student groups

25
Weaknesses

26
Specialist services

27
Weaknesses Limited coverage - diagnosis and tx Inadequate resources for children and severely affected Havent bench marked yet Inadequate evidence base particularly for children and severely affected Patient involvement Limited coverage - diagnosis and tx Inadequate resources for children and severely affected Havent bench marked yet Inadequate evidence base particularly for children and severely affected Patient involvement

28
Opportunities Research: Only place able to do large scale biological research eg Genome Wide Association studies Potential to transform care Research Political pressure Ability to provide national training programmes Research: Only place able to do large scale biological research eg Genome Wide Association studies Potential to transform care Research Political pressure Ability to provide national training programmes

29
Threats

Similar presentations