Download presentation
Presentation is loading. Please wait.

1
Understanding Dementia
Colin MacDonald Trainer in Dementia Care

2
Dementia: some important facts
An organic (physical) illness Irreversible damage to brain cells Progressive decline – ending in death Affects approx. 750,000 people in UK Prevalence increases with age (demographic changes) More common in women Increased prevalence in long term care settings Major source of increased pressure and stress on carers and organisations A person’s gender can have a bearing on their experience of and approach to pain. Under experimental circumstances women are shown to have a slightly “lower threshold, higher rating and less tolerance” (Berkley, 1997 p: 372) to pain than men. Women report more experiences of pain. This is in part due to differences in nerve structures (Hawkes 2000), which result in women experiencing increased levels of hyperalgesia* (Berkley 1997). Pain also interferes to a greater degree with the traditional tasks undertaken by women, for example housework (Oakley, 1974), and this extends into older age (Scudds and Østbye 2001). However, the research as a whole suggests that the differences are negligible and relate more to social and cultural factors. Within most cultures women generally discuss pain more openly and seek assistance when needed (Berkley, 1997). Cultures in which strong male hegemonies exist show lower levels of pain reporting (Skevington 1995), though men have been shown to worry about the meaning of prolonged pain to a greater extent than women (Morin et al., 2000). Different cultures may use various forms of support to address pain. African-Americans have been found to use distraction and praying more than American Caucasians (Edwards et al., 2001) to support them through a physical pain experience. The individual’s historical or religious background can also significantly affect the response to pain (Skevington, 1995; Zborowski, 1952). Particular concern has been raised about the level of discrimination that exists in care for people of different ethnicities in areas such as dementia care (Yeo et al., 1996) and studies have evidenced inequality in the treatment of pain for people from minority ethnic communities (Bonham, 2001; Todd et al., 1993). At a personal level, childhood victimization (Raphael et al., 2001) as well as a family history of pain (Fillingim et al., 2000) are associated with a higher reporting of physical pain. * Referred sensation such as parasthesia like tingles, itch or numbness, changes in the perceived temperature of a body part or a feeling of pressure or constriction (Skevington, 1996)
 illness. Irreversible damage to brain cells. Progressive decline – ending in death. Affects approx. 750,000 people in UK. Prevalence increases with age (demographic changes) More common in women. Increased prevalence in long term care settings. Major source of increased pressure and stress on carers and organisations. A person’s gender can have a bearing on their experience of and approach to pain. Under experimental circumstances women are shown to have a slightly lower threshold, higher rating and less tolerance (Berkley, 1997 p: 372) to pain than men. Women report more experiences of pain. This is in part due to differences in nerve structures (Hawkes 2000), which result in women experiencing increased levels of hyperalgesia* (Berkley 1997). Pain also interferes to a greater degree with the traditional tasks undertaken by women, for example housework (Oakley, 1974), and this extends into older age (Scudds and Østbye 2001). However, the research as a whole suggests that the differences are negligible and relate more to social and cultural factors. Within most cultures women generally discuss pain more openly and seek assistance when needed (Berkley, 1997). Cultures in which strong male hegemonies exist show lower levels of pain reporting (Skevington 1995), though men have been shown to worry about the meaning of prolonged pain to a greater extent than women (Morin et al., 2000). Different cultures may use various forms of support to address pain. African-Americans have been found to use distraction and praying more than American Caucasians (Edwards et al., 2001) to support them through a physical pain experience. The individual’s historical or religious background can also significantly affect the response to pain (Skevington, 1995; Zborowski, 1952). Particular concern has been raised about the level of discrimination that exists in care for people of different ethnicities in areas such as dementia care (Yeo et al., 1996) and studies have evidenced inequality in the treatment of pain for people from minority ethnic communities (Bonham, 2001; Todd et al., 1993). At a personal level, childhood victimization (Raphael et al., 2001) as well as a family history of pain (Fillingim et al., 2000) are associated with a higher reporting of physical pain. * Referred sensation such as parasthesia like tingles, itch or numbness, changes in the perceived temperature of a body part or a feeling of pressure or constriction (Skevington, 1996)")
3
Dementia is often associated with challenging behaviour
BUT it is NOT an inevitable consequence of the disease Process ! !

4
Dementia: its importance quantified?
In the United States it takes: * 1,500 hours of training, passing a proficiency and written exam to get a license to be a Barber or Beautician; * 400 hours of training, passing a proficiency and written exam to get a license to be a Dog Groomer; * 75 hours of training, passing a proficiency and written exam to get a license to be a Paid Care Worker/Front-line Worker.

5
Changes to the brain memory thinking learning reasoning
Characterised by a decline in: cognitive abilities memory thinking learning reasoning emotional control social behaviour motivation

6
Vascular (Multi-Infarct)
Types of Dementia CJD Alzheimer’s AIDs Related Alcohol Related Vascular (Multi-Infarct) Dementia With Lewy Bodies DAT 50-60% VD 20-30, Mixed 10% A significant number of people diagnosed with dementia are found to have tiny spherical structures called Lewy bodies in the nerve cells of their brains. It is thought these may contribute to the death of brain cells. Dementia is often mild at the outset and can be extremely variable from day to day. The symptoms are the fluctuation in the condition, visual hallucinations and extreme sensitivity to classical anti psychotic medications leading to marked symptoms of stiffness, tremor and restriction of movement. Dementia with Lewy bodies sometimes co-occurs with Alzheimer’s disease and Vascular dementia. Alcohol Related Dementia: Korsakoff’s Syndrome Too much alcohol, particularly if associated with a diet deficient in thiamine (Vitamin B1) can lead to irreversible brain damage. This dementia is preventable. If people don’t drink, or they drink at a safe level, they don’t get it. The most vulnerable parts of the brain are those used for memory, and for planning, organizing and judgement, social skills and balance. If drinking stops there may be some improvement. Taking thiamine appears to help prevent and improve the condition. Frontal Lobe Dementia e.g. Picks Lewy Body's
 Dementia With Lewy Bodies DAT 50-60% VD 20-30, Mixed 10% A significant number of people diagnosed with dementia are found to have tiny spherical structures called Lewy bodies in the nerve cells of their brains. It is thought these may contribute to the death of brain cells. Dementia is often mild at the outset and can be extremely variable from day to day. The symptoms are the fluctuation in the condition, visual hallucinations and extreme sensitivity to classical anti psychotic medications leading to marked symptoms of stiffness, tremor and restriction of movement. Dementia with Lewy bodies sometimes co-occurs with Alzheimer’s disease and Vascular dementia. Alcohol Related Dementia: Korsakoff’s Syndrome. Too much alcohol, particularly if associated with a diet deficient in thiamine (Vitamin B1) can lead to irreversible brain damage. This dementia is preventable. If people don’t drink, or they drink at a safe level, they don’t get it. The most vulnerable parts of the brain are those used for memory, and for planning, organizing and judgement, social skills and balance. If drinking stops there may be some improvement. Taking thiamine appears to help prevent and improve the condition. Frontal Lobe Dementia. e.g. Picks. Lewy Body s.")
7
Dementia – what it isn’t
Not the same as normal ageing - some symptoms may be similar - Not severe or progressive - Do not normally die from normal ageing (esp < 10 years) Confusion (acute confusional states or delirium) Brain Damage (one-off) Pychiatric illnesses
 Confusion (acute confusional states or delirium) Brain Damage (one-off) Pychiatric illnesses.")
8
Understanding the Persons reality and experience
What is it like to have dementia? Try to imagine the experience… BUT CAN WE !!

9
Ref. The Last Escape. J. Nicol. Penguin
Whose experience? “Throughout the ordeal you have to rely on your own strength of character. But the harsh reality is that control is out of your hands. You go from being confident to a terrified, lonely, simple human being at the mercy of others. Weeks are punctuated by isolation, fear, boredom, an awful, tragic, mind numbingly terrible time” Ref. The Last Escape. J. Nicol. Penguin

10
The “Experience” of Dementia (from R
The “Experience” of Dementia (from R. Davis – “My Journey Through Alzheimers Disease). “The blackness” – the sudden and devastating loss of memory “files” “World closing in” – security and confidence Coping with stress / agitation – physical exertion !!? Others reaction to you – - “the diagnosis” - “secrecy and paranioa” - “being talked over..” - “childish/scornful reaction”
. The blackness – the sudden and devastating loss of memory files World closing in – security and confidence. Coping with stress / agitation – physical exertion !! Others reaction to you – - the diagnosis - secrecy and paranioa - being talked over.. - childish/scornful reaction")
11
The experience of Dementia
Consider: Trying to make sense of an increasingly unfamiliar world Unable to make sense of the immediate environment Unable to access areas of memory Being disorientated – to time, place or person Unable to respond to emotional demands as before Being unable to verbally communicate your needs Loss of “strengths” – “weaknesses” come to the fore Loss of personal identity and control over your life Being “ignored”, “talked over” or treated as “stupid” Individual coping skills

12
Attitudes, views, and beliefs about older people
What about us? An ageist society? Stereotypes? Perceptions of behaviour Negative and nihilistic views Care models and approaches Custodial and authoritarian attitudes Inflexible routines and task orientated care Focus on safety and physical care only WILL ALL CONTRIBUTE TOWARDS BEHAVIOUR THAT WE FIND CHALLENGING!

13
The disabling impact of the environment
Does it make sense to the person? Lack of information Reduced Visual Access Lack of signs, cues and landmarks Areas of importance not highlighted Inappropriate lighting Too much noise and conflicting stimuli Patterned carpets and shiny flooring Caution with mirrors

14
Reduce the impact of the environment
Good signage Large size Right height Use of strong contrasts Yellow highly visible Symbol and text On doors, not beside

15
Burnett Pollock Associates

16
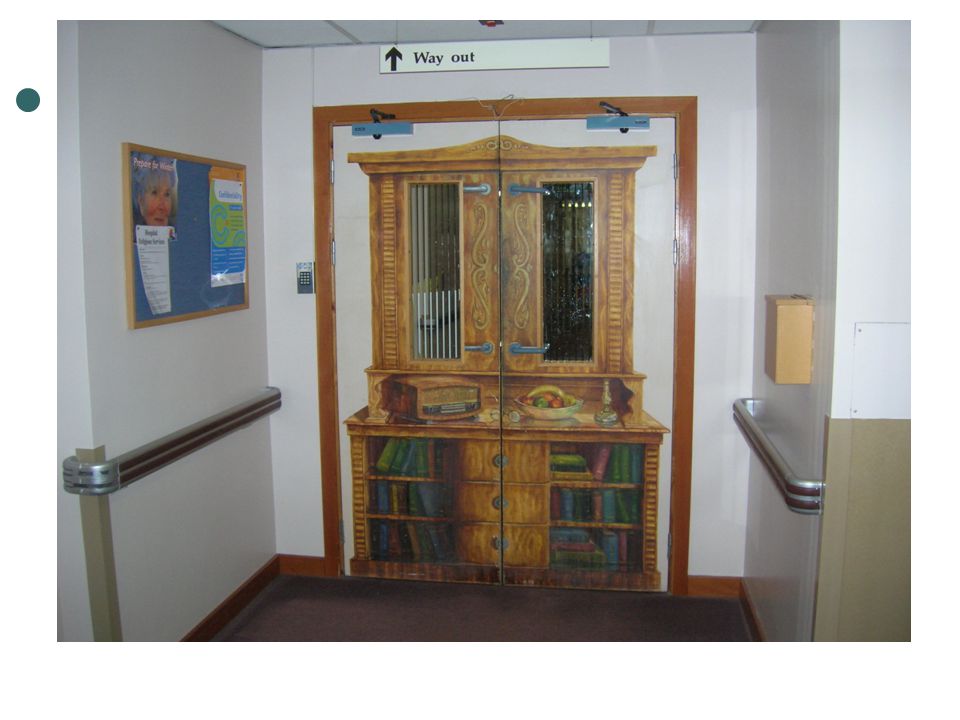
Decoration Enable access Restrict access Burnett Pollock Associates

18
Dementia as a disability is something that CAN be compensated for.
Final Point Dementia as a disability is something that CAN be compensated for. The person with dementia can’t adapt to us – we need to adapt our social and built environment around the person.

19
Thank You

Similar presentations