Download presentation
Presentation is loading. Please wait.

1
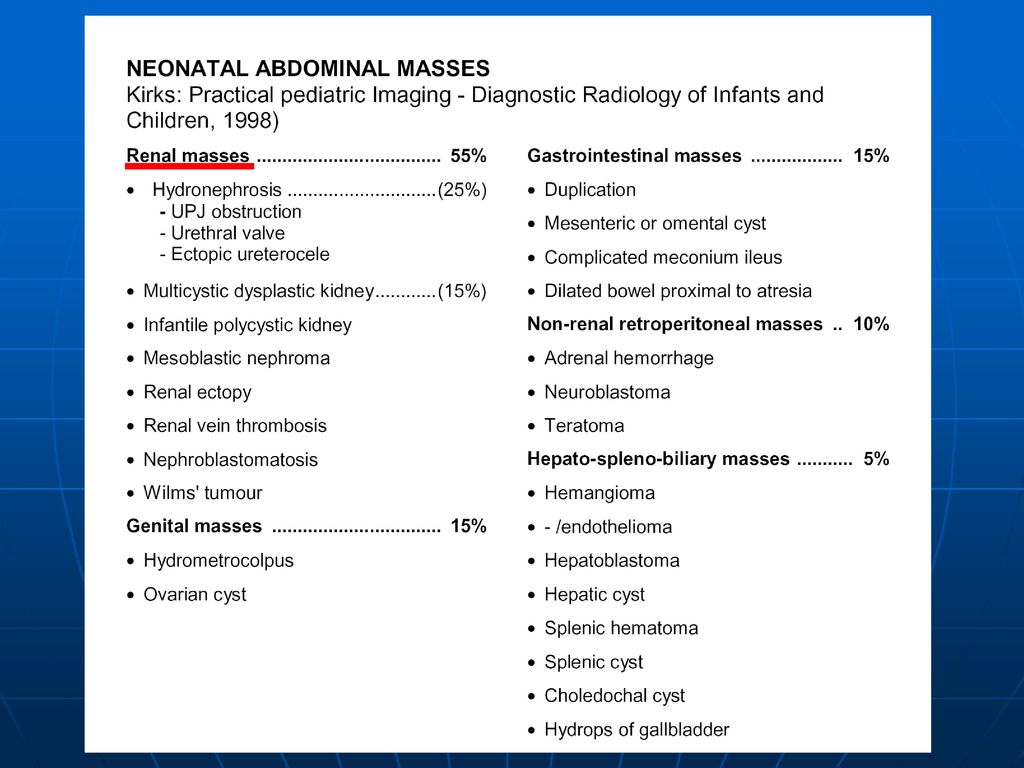
Pediatric Abdominal Mass
Discussion Pediatric Abdominal Mass

4
Wilms’ tumor Undifferentiated metanephric blastema
Most common malignant abdominal neoplasm in children 1-8 years old (10%) 3rd most common malignancy in childhood (after leukemia + brain tumors; neuroblastoma more common in infancy)!
 3rd most common malignancy in childhood (after leukemia + brain tumors; neuroblastoma more common in infancy)!")
5
Incidence:1:10,000 livebirths; familial in 1-2%; multifocal in 10%; bilateral in 4.4-9%
Age:peak age at years (range of 3 months to 8 years) rare during first year; 50% before 3 years, 75% before 5 years; 90% before 8 years; rare in adults; M:F = 1:1
6
Clinical evalution Palpable abdominal mass, usually unilateral (90%)
Hypertension (47-90%) Abdominal pain (25%), fever (15%), hematuria (7-15%) Paraneoplastic syndromes Congenital anomaly (15%)
 Abdominal pain (25%), fever (15%), hematuria (7-15%) Paraneoplastic syndromes. Congenital anomaly (15%)")
7
Radiologic evaluation
Plain film: US: CT: -- Unenhanced : round, well-defined, solid, less dense, intrarenal mass -- Distortion of collecting system -- Calcification 15% -- Partially cystic = focal hemorrhage and necrosis (71%) -- Enhanced: inhomogenous, less dense MR: hypointense on T1WI, variable on T2WI
 -- Enhanced: inhomogenous, less dense. MR: hypointense on T1WI, variable on T2WI.")
8
Mass displacing adjacent bowel or collecting system
Calcification(5%)
")
9
fairly evenly echogenic mass
± irregular anechoic areas due to central necrosis + hemorrhage

12
Treatment and prognosis
Treatments for Wilms' tumor depend on the stage of your child's disease, the cell type (histology), and your child's age and general health. Surgery, CT, and RT Prognosis:90% survival rate depending on pathologic pattern, age at time of diagnosis, extent of disease
, and your child s age and general health. Surgery, CT, and RT. Prognosis:90% survival rate depending on pathologic pattern, age at time of diagnosis, extent of disease.")
13
Neuroblastoma Origin: neural crest
Most common solid abdominal mass of infancy (12.3% of all perinatal neoplasms), 3rd most common malignant tumor in infancy (after leukemia + CNS tumors), 2nd most common tumor in childhood (Wilms tumor more common in older children), 7% of all childhood cancers; 15% of cancer deaths in children
14
Incidence:1:7,100 to 1:10,000 livebirths; 20% hereditary
Age: peak age at 2 years; 25% during 1st year; 50% <2 years; 75% in <4 years; 90% in <8 years; occasionally present at birth; M:F = 1:1 Location: anywhere within sympathetic neural chain
15
Clinical evaluation Palpable, firm, irregular, slightly tender abdominal mass, often cross the midline Hypertension (up to 30%) Silent until invasion or compression adjacent structures: -- Edema of legs, constipation, oligouria, radicular pain or paraplegia Fever, weight loss, and gerenalized pain
 Silent until invasion or compression adjacent structures: -- Edema of legs, constipation, oligouria, radicular pain or paraplegia. Fever, weight loss, and gerenalized pain.")
16
Metastases: bone (60%), regional lymph nodes (42%), orbit (20%), liver (15%), intracranial (14%), lung (10%) Encase the great vessels Paraneoplastic syndrome: -- opsoclonus - myoclonus syndrome -- Intractable watery diarrhea

17
Increased 24-hour urinary levels of catecholamine metabolites
Elevated Dopamine Bone marrow aspirate positive in 50-70% at time of initial diagnosis

18
Radiologic evaluation
Plain film: mass, calcification (50%) US: hyper- / hypoechoic mass with acoustic shadows CT: calcification(60%) -- Enhanced : irregular, lobulated, unencapsulated, inhomogeneous tumor, often with central necrosis -- encasement of IVC + aorta, celiac axis, SMA (32%) MRI: low on T1 and high on T2, uniform and well-defined
 US: hyper- / hypoechoic mass with acoustic shadows. CT: calcification(60%) -- Enhanced : irregular, lobulated, unencapsulated, inhomogeneous tumor, often with central. necrosis. -- encasement of IVC + aorta, celiac axis, SMA. (32%) MRI: low on T1 and high on T2, uniform and well-defined.")
21
Neuroblastoma VS Wilms’ tumor
Predominant suprarenal mass Growth across the midline Multifocal calcification within mass Displacement of the great vessels

22
Treatment and Prognosis
Complete resection is difficult due to vascular invasion Multiple chemotherapy or radiation therapy Prognostic factor: Age, stage and location 2-year survival rate versus age at presentation: -- 60%if patients age<1year -- 20%if patients age1-2years -- 10%if patients age>2years

23
HEPATOBLASTOMA Incidence: 3rd most common abdominal tumor in children; most frequent malignant hepatic tumor in children (51%) Age: <3 years; <18 months (in 50%); peak age between 18 and 24 months; range from newborn to 15 years; M:F = 2:1 --epithelial type = small cells resembling embryonal / fetal liver --mixed type = epithelial cells + mesenchymal cells
; peak age between 18 and 24 months; range from newborn to 15 years; M:F = 2:1. --epithelial type = small cells resembling. embryonal / fetal liver. --mixed type = epithelial cells + mesenchymal cells.")
24
Clinical evaluation Upper abdominal mass Weight loss, nausea, vomiting
Precocious puberty (production of endocrine substances) Persistently + markedly elevated AFP (66%) Metastases to: lung (frequent)
 Persistently + markedly elevated AFP (66%) Metastases to: lung (frequent)")
25
Location: right lobe of the liver
Usually solitary mass with an average size of cm Coarse calcifications / osseous matrix (12-30%) US: -- large heterogeneous echogenic mass, sometimes with calcifications, occasionally cystic areas (necrosis / extramedullary hematopoiesis) CT: -- hypointense tumor with peripheral rim enhancement
 US: -- large heterogeneous echogenic mass, sometimes with calcifications, occasionally cystic areas (necrosis / extramedullary hematopoiesis) CT: -- hypointense tumor with peripheral rim enhancement.")
27
MR: -- inhomogeneously hypointense on T1WI with hyperintense foci (hemorrhage) -- inhomogeneously hyperintense with hypointense bands (fibrous septa) on T2WI Angio: -- hypervascular mass with dense stain -- NO AV-shunting -- vascular lakes may be present -- may show caval involvement (= unresectable)
 on T2WI. Angio: -- hypervascular mass with dense stain. -- NO AV-shunting. -- vascular lakes may be present. -- may show caval involvement (= unresectable)")
29
Treatment and Prognosis
Complete excision 50%~60% Adjuvant chemotherapy Prognosis:60% resectable; 75% mortality; better prognosis than hepatoma; better prognosis for epithelial type than mixed type

Similar presentations










.>")
>")















