Download presentation
Presentation is loading. Please wait.

1
Dr. David R. Barnum Research Lecture
The Use of Beta Blockers in Patients with COPD on Long Term Oxygen Therapy Dr. David R. Barnum Research Lecture May 26, 2017 Author: John Matera, MD

2
Objectives To provide background information on COPD
To discuss the research methods used in this study To examine the effect of beta-blockers on mortality in Chronic Obstructive Pulmonary Disease Patients on Long Term Oxygen Therapy.

3
Background Chronic Obstructive Pulmonary Disease (COPD)
Disease characterized by airflow obstruction 3rd ranked cause of death in the United States Mortality 120,000 deaths per year Airflow obstruction is treated with inhaled beta-agonists Non-selective beta-blockade can worsen airflow obstruction

4
GOLD Treatment Guidelines
Long-term oxygen therapy usually indicated severe disease Short-acting bronchodilators usually are beta-agonists

5
Why This Question The effects of beta blockers in COPD has controversial effects on mortality rate McGarvey et al. in 2007 studied severe COPD and causes of mortality findings included: 26% of patients with a cardiovascular source of death 35% with a respiratory cause of death 21% caused by malignancy- so we know cardiac disease is a significant contributor to all cause mortality (but there was no risk stratification correlating this with long term oxygen therapy) A meta-analysis by Etminan et al in 2012 showed: Improved mortality in patient’s with COPD on beta blockers But as with any meta-analysis there is the risk for confounding by indication (i.e. clinicians would only prescribe beta-blockers to patients with mild COPD due to theoretical risks of beta-blockade upon lung function) Note to self, mention the opening of a Christmas carol and “marley was dead, that must be abundantly clear or nothing thereafter will make any sense” as the reason for the thorough explanation of why this question is being asked, its not enough to say the literature is unclear- show them in this context as people are hesitant to prescribe beta blockers to patient’s with COPD, so when they are knowingly withheld from patient’s with severe COPD it appears that there is a potentially beneficial effect when treating comorbid conditions)
 A meta-analysis by Etminan et al in 2012 showed: Improved mortality in patient’s with COPD on beta blockers. But as with any meta-analysis there is the risk for confounding by indication (i.e. clinicians would only prescribe beta-blockers to patients with mild COPD due to theoretical risks of beta-blockade upon lung function) Note to self, mention the opening of a Christmas carol and marley was dead, that must be abundantly clear or nothing thereafter will make any sense as the reason for the thorough explanation of why this question is being asked, its not enough to say the literature is unclear- show them. in this context as people are hesitant to prescribe beta blockers to patient’s with COPD, so when they are knowingly withheld from patient’s with severe COPD it appears that there is a potentially beneficial effect when treating comorbid conditions)")
6
Increased mortality with use of beta-blockade in COPD
Ekstrom et al. in 2013 studied the effects of cardiovascular drugs in patients with COPD using long term oxygen: Drugs included ACE inhibitors, ARBS, antiplatelet agents, and beta blockers All patients had severe COPD on long term oxygen Used probability of drug exposure If a prescription was placed it was assumed to be exposure for 3 months Results showed worsening mortality rate with use of beta blockade when controlled for ischemic heart disease Keep in mind this study also demonstrated Increased hazard ratio with use of oral glucocorticoids Findings may reflect severity of disease and exacerbations rather than the drugs themselves Any 1 diagnosis was sufficient to qualify for heart disease, including heart failure or ischemic disease A-fib was not considered as a diagnosis for heart disease In first study, all patient’s had severe COPD, and 50% of the subjects diet, this was severe

7
Confounding Information
No mention of A-fib as a diagnosis pertaining to heart disease Ekstrom et al. in 2013 – diagnosis codes used to define heart disease

8
And Yet…beta-blockers could be useful in COPD to lower mortality
COPD patients who have atrial fibrillation have an increased risk of mortality [Varun Shah et al 2016] Elevated heart rate is an independent predictor of mortality [Jensen, M.T., et al., 2013] Post myocardial infarction, use of beta-blockers [carvedilol] can decrease atrial fibrillation [McMurray, J., et al, 2005]

9
Confounding Information
Heart Disease (including A-fib) Mortality ? Beta Blocker Use The question becomes
 Mortality. Beta Blocker Use. The question becomes.")
10
Despite This Current GOLD guidelines endorse the treatment of heart disease as if COPD did not exist. Beta blockers may worsen airflow obstruction, but may reduce cardiac related mortality in a number of ways So really we are discussing possible cardioprotective effects of beta blockers, vs possible effects on lung function

11
To Summarize: Comorbid Conditions with COPD
COPD is associated with Heart disease (including CHF, coronary artery disease and A-fib) Hypoxia Mortality from COPD is typical caused by Coronary artery disease
 Hypoxia. Mortality from COPD is typical caused by. Coronary artery disease.")
12
Research Design Retrospective study based on chart review.
Patient charts from April 2009 to April 2015 for patients with a diagnosis of COPD who are on long term oxygen therapy (LTOT) age 18-95 COPD was defined by: Pulmonary function tests showing FEV1/FVC ratio less than 0.70 or less than the lower limit of normal [LLN] plus an FEV1 less than 80 percent of predicted and only partially reversible with bronchodilator therapy Clinical diagnosis
 age COPD was defined by: Pulmonary function tests showing FEV1/FVC ratio less than 0.70 or less than the lower limit of normal [LLN] plus an FEV1 less than 80 percent of predicted and only partially reversible with bronchodilator therapy. Clinical diagnosis.")
13
Definitions Long term oxygen therapy (LTOT) was defined by a diagnosis of COPD and one of the following PaO2 of <55mmHg (O2 sats <88%) on rest or ambulation PaO2 of mmHg (O2 sats <89%) and who exhibit signs of tissue hypoxia eg, pulmonary hypertension, cor pulmonale, erythrocytosis, edema from right heart failure or impaired mental status. Beta blocker use was defined as Current use of any class of beta blocker (selective or nonselective) Present in the ambulatory encounter For a minimum duration of 6 months
 on rest or ambulation. PaO2 of mmHg (O2 sats <89%) and who exhibit signs of tissue hypoxia. eg, pulmonary hypertension, cor pulmonale, erythrocytosis, edema from right heart failure or impaired mental status. Beta blocker use was defined as. Current use of any class of beta blocker (selective or nonselective) Present in the ambulatory encounter. For a minimum duration of 6 months.")
14
Definitions Coronary Artery Disease Heart Failure Atrial Fibrillation
Defined by evidence of obstruction on cardiac angiogram, the presence of calcified plaques on CT imaging, or by clinical history Heart Failure Left sided heart failure defined by clinical symptoms or supporting echocardiography demonstrating impaired left sided systolic or diastolic cardiac function. Atrial Fibrillation We define atrial fibrillation as the presence of an irregularly irregular rhythm without the presence of p-waves captured on an electrocardiogram. A single episode of this event is enough to diagnose a subject as having a history of atrial fibrillation.

15
Main Group Analysis Subdividing our subjects into two groups:
Patients who have used any beta blocker in the outpatient setting for 6 months or more Patients who have not been a beta blocker for 6 months or more Secondary sub-group analysis with respect to co-morbidities including Atrial fibrillation, Congestive heart failure (either systolic or diastolic) CAD.
 CAD.")
16
Outcomes Primary outcome: all-cause mortality rates
3 year survival propensity match, patients will be deemed alive if they were alive on 1/1/16 (given potential lag from social security office reporting deaths) This guarantees that all patients had a minimum of 6 months of beta blocker use prior to the end of the study, or prior to death Secondary analysis includes Hospital admission and exacerbation rates
 This guarantees that all patients had a minimum of 6 months of beta blocker use prior to the end of the study, or prior to death. Secondary analysis includes. Hospital admission and exacerbation rates.")
17
Data Gathering Initial screening found > 4000 patients with COPD in the NorthShore system with the dates and ages defined Further screening was performed to identify patients on long term oxygen with a documented indication [excluded home oxygen for comfort, OSA, or palliative measures] Cohort was assessed for the presence or absence of: A-fib CHF CAD PFT results

18
Results Filler pending ed results from data scientist

19
Conclusions Filler pending ed results from data scientist

20
Acknowledgements Thank you to the following people for all of your help with this project Dr. Shashi Bellam Mohammad Imran Beig Daniel Chertok Shad Mahmood

21
References 1. Centers for Disease, C. and Prevention, Chronic obstructive pulmonary disease among adults--United States, MMWR Morb Mortal Wkly Rep, (46): p 2. Soriano, J.B., et al., Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest, (4): p 3. Mannino, D.M., et al., Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J, (4): p 4. McGarvey, L.P., et al., Ascertainment of cause-specific mortality in COPD: operations of the TORCH Clinical Endpoint Committee. Thorax, (5): p 5. Rutten, F.H., et al., Beta-blockers may reduce mortality and risk of exacerbations in patients with chronic obstructive pulmonary disease. Arch Intern Med, (10): p 6. Dransfield, M.T., et al., Use of beta blockers and the risk of death in hospitalised patients with acute exacerbations of COPD. Thorax, (4): p 7. van Gestel, Y.R., et al., Impact of cardioselective beta-blockers on mortality in patients with chronic obstructive pulmonary disease and atherosclerosis. Am J Respir Crit Care Med, (7): p 8. Stefan, M.S., et al., Association between beta-blocker therapy and outcomes in patients hospitalised with acute exacerbations of chronic obstructive lung disease with underlying ischaemic heart disease, heart failure or hypertension. Thorax, (11): p 9. Etminan, M., et al., Beta-blocker use and COPD mortality: a systematic review and meta-analysis. BMC Pulm Med, : p. 48. 10. Jensen, M.T., et al., Resting heart rate is a predictor of mortality in COPD. Eur Respir J, (2): p
: p Soriano, J.B., et al., Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest, (4): p Mannino, D.M., et al., Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J, (4): p McGarvey, L.P., et al., Ascertainment of cause-specific mortality in COPD: operations of the TORCH Clinical Endpoint Committee. Thorax, (5): p Rutten, F.H., et al., Beta-blockers may reduce mortality and risk of exacerbations in patients with chronic obstructive pulmonary disease. Arch Intern Med, (10): p Dransfield, M.T., et al., Use of beta blockers and the risk of death in hospitalised patients with acute exacerbations of COPD. Thorax, (4): p van Gestel, Y.R., et al., Impact of cardioselective beta-blockers on mortality in patients with chronic obstructive pulmonary disease and atherosclerosis. Am J Respir Crit Care Med, (7): p Stefan, M.S., et al., Association between beta-blocker therapy and outcomes in patients hospitalised with acute exacerbations of chronic obstructive lung disease with underlying ischaemic heart disease, heart failure or hypertension. Thorax, (11): p Etminan, M., et al., Beta-blocker use and COPD mortality: a systematic review and meta-analysis. BMC Pulm Med, : p Jensen, M.T., et al., Resting heart rate is a predictor of mortality in COPD. Eur Respir J, (2): p")
22
References 11. Chhabra, S.K. and S. De, Cardiovascular autonomic neuropathy in chronic obstructive pulmonary disease. Respir Med, (1): p 12. Bangalore, S., et al., Clinical outcomes with beta-blockers for myocardial infarction: a meta-analysis of randomized trials. Am J Med, (10): p 13. Behar, S., et al., Long-term prognosis of patients with paroxysmal atrial fibrillation complicating acute myocardial infarction. SPRINT Study Group. Eur Heart J, (1): p 14. Pedersen, O.D., et al., The occurrence and prognostic significance of atrial fibrillation/-flutter following acute myocardial infarction. TRACE Study group. TRAndolapril Cardiac Evalution. Eur Heart J, (10): p 15. McMurray, J., et al., Antiarrhythmic effect of carvedilol after acute myocardial infarction: results of the Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN) trial. J Am Coll Cardiol, (4): p 16. Ekstrom, M.P., A.B. Hermansson, and K.E. Strom, Effects of cardiovascular drugs on mortality in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med, (7): p 17. Minino, A.M., et al., Deaths: final data for Natl Vital Stat Rep, (10): p 18. Varun Shah, et al., The Association Between Chronic Obstructive Pulmonary Disease (COPD) and Atrial Fibrillation: A Review. Chronic Obstructive Pulmoanry Disease: Open Access, 2016 19. UpToDate, Chronic obstructive pulmonary disease: Definition, clinical manifestations, diagnosis, and staging; 20. UpToDate, Management of stable chronic obstructive pulmonary disease;
: p Bangalore, S., et al., Clinical outcomes with beta-blockers for myocardial infarction: a meta-analysis of randomized trials. Am J Med, (10): p Behar, S., et al., Long-term prognosis of patients with paroxysmal atrial fibrillation complicating acute myocardial infarction. SPRINT Study Group. Eur Heart J, (1): p Pedersen, O.D., et al., The occurrence and prognostic significance of atrial fibrillation/-flutter following acute myocardial infarction. TRACE Study group. TRAndolapril Cardiac Evalution. Eur Heart J, (10): p McMurray, J., et al., Antiarrhythmic effect of carvedilol after acute myocardial infarction: results of the Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN) trial. J Am Coll Cardiol, (4): p Ekstrom, M.P., A.B. Hermansson, and K.E. Strom, Effects of cardiovascular drugs on mortality in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med, (7): p Minino, A.M., et al., Deaths: final data for Natl Vital Stat Rep, (10): p Varun Shah, et al., The Association Between Chronic Obstructive Pulmonary Disease (COPD) and Atrial Fibrillation: A Review. Chronic Obstructive Pulmoanry Disease: Open Access, UpToDate, Chronic obstructive pulmonary disease: Definition, clinical manifestations, diagnosis, and staging; source=search_result&search=COPD&selectedTitle=1~ UpToDate, Management of stable chronic obstructive pulmonary disease; source=search_result&search=copd%20treatment&selectedTitle=1~150.")
23
Alan Moreno MD Louisa Tammy Ho MD 5/26/2017
Empiric cefazolin and ceftazidime in outpatient treatment of peritonitis in peritoneal dialysis patients Alan Moreno MD Louisa Tammy Ho MD 5/26/2017

24
Objectives Background on peritoneal dialysis Peritonitis
Current treatment guidelines Results Conclusions and future consideration

25
Peritoneal Dialysis – the dominant method of home dialysis
Background Peritoneal Dialysis – the dominant method of home dialysis

26
Background Benefits Drawbacks Flexible Cheaper
Afford active lifestyle Less fluid/dietary restrictions Cheaper No adverse vascular events No survival/mortality difference between HD and PD Higher health literacy required Preexisting conditions Previous abdominal surgeries Psychiatric conditions Cumbersome hardware PD fluid Cyclers Cost comparison of peritoneal dialysis versus hemodialysis in end-stage renal disease.

27
Background Types Continuous ambulatory peritoneal dialysis (CAPD) Typically 4 exchanges throughout the day Automated peritoneal dialysis (APD) A “CYCLER” does multiple exchanges for you while asleep All forms of PD require patient or family access of indwelling catheter to connect to a system of dialysis
 A CYCLER does multiple exchanges for you while asleep. All forms of PD require patient or family access of indwelling catheter to connect to a system of dialysis.")
30
Background Northshore has a greater number of ESRD patients performing PD Approximately 10% of ESRD patients nationally perform PD. In USRDS data as of 2016: 421,219 HD 46,121 PD In our system 20% of ESRD as of 2016 perform PD 289 HD patients 75 PD patients

31
Background There is a growing number of both incident and prevalent home dialysis patients Centers for Medicare & Medicaid 2011 financial incentives increased favoring home dialysis In 2011, IHI published a case study of Swedish dialysis patients who had taken on self-management of their own dialysis and care. The operating costs of the unit dropped 33% because of reduced complications, and patient satisfaction was undeniably improved. Net profits are greater In 2011, Medicare began bundling dialysis care payments in an attempt to better control expenses, paying about $240 per treatment, or around $37,000 a year to empower patients in managing overall costs.

32
Figure Trends in number of prevalent ESRD cases (in thousands) using home dialysis, by type of therapy, in the United States, Data Source: Reference Table D.1. December 31 prevalent ESRD patients; Peritoneal dialysis consists of CAPD and CCPD only. Abbreviations: CAPD, continuous ambulatory peritoneal dialysis; CCPD, continuous cycler peritoneal dialysis; ESRD, end-stage renal disease. 2016 Annual Data Report, Vol 2, ESRD, Ch 1

33
Figure Trends in the number of incident ESRD cases (in thousands) using home dialysis, by type of therapy, in the U.S. population, Data Source: Reference Table D.1. Abbreviations: ESRD, end-stage renal disease; PD, peritoneal dialysis. 2016 Annual Data Report, Vol 2, ESRD, Ch 1

34
Peritonitis The number one cause of loss of patient from PD to HD is peritonitis peritoneal inflammation and changes in peritoneal transport can lead to therapy failure Early and effective management of peritonitis is essential to any home program Peritonitis incidence is variable from center to center significant differences in rates are seen in different countries Hsieh Y-P, Chang C-C, Wen Y-K, Chiu P-F, Yang Y. Predictors of Peritonitis and the Impact of Peritonitis on Clinical Outcomes of Continuous Ambulatory Peritoneal Dialysis Patients in Taiwan—10 Years’ Experience in a Single Center. Peritoneal Dialysis International : Journal of the International Society for Peritoneal Dialysis. 2014;34(1): doi: /pdi Peritonitis is associated with peritoneal inflammation leading to hyperemia and changes in peritoneal transport. The changes of impaired ultrafiltration increased peritoneal transport of low-molecular-weight solutes and increased rates of glucose absorption, are usually transient and typically resolve within a month after resolution of the peritonitis
: doi: /pdi Peritonitis is associated with peritoneal inflammation leading to hyperemia and changes in peritoneal transport. The changes of impaired ultrafiltration increased peritoneal transport of low-molecular-weight solutes and increased rates of glucose absorption, are usually transient and typically resolve within a month after resolution of the peritonitis.")
35
Peritonitis Etiology of infection Interluminal Periluminal
Secondary to non-sterile techniques with exchanges Periluminal Skin infections at the catheter exit site Spontaneous bacterial peritonitis Bacterial translocation Hematologous Rare Transvaginal Grading of exit site infections - Keane WF, Bailie GR, Boeschoten E, Gokal R, Golper TA, Holmes CJ, Kawaguchi Y, Piraino B, Riella M, Vas S, International Society for Peritoneal Dialysis SOPerit Dial Int. 2000;20(4):396.
:396.")
36
Peritonitis Most common international infections Gram positive
Coagulase negative staphylococci Staphylococcus epidermidis Staphylococcus aureus Streptococcus sp. Enterococcus sp. Gram negative Pseudomonas sp. Klebsiella sp. Proteus sp. Bianchi P, Buoncristiani E, Buoncristiani U. Antisepsis. Contrib Nephrol. 2007;154:1–6. Brook NR, White SA, Waller JR, Nicholson ML. The surgical management of peritoneal dialysis catheters. Ann R Coll Surg Engl. 2004;86:190–195. Renaud CJ, Subramanian S, Tambyah PA, Lee EJ. The clinical course of rapidly growing nontuberculous mycobacterial peritoneal dialysis infections in Asians: A case series and literature review. Nephrology (Carlton) 2011;16:174–179. Gupta S, Muralidharan S, Gokulnath H. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in southern India using an automated blood culture system to culture peritoneal dialysate. Nephrology (Carlton) 2011;16:63–67. Davies S. Clinical practice guidelines module 3b: peritoneal dialysis, UK Renal Association Third Edition, Available from: Epidemiology of PD related infections etc - Akoh JA. Peritoneal dialysis associated infections: An update on diagnosis and management. World Journal of Nephrology. 2012;1(4): doi: /wjn.v1.i4.106. - prophylactic antibiotic administration before catheter placement, adequate patient training, exit-site care
 2011;16:174–179. Gupta S, Muralidharan S, Gokulnath H. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in southern India using an automated blood culture system to culture peritoneal dialysate. Nephrology (Carlton) 2011;16:63–67. Davies S. Clinical practice guidelines module 3b: peritoneal dialysis, UK Renal Association Third Edition, Available from: Epidemiology of PD related infections etc - Akoh JA. Peritoneal dialysis associated infections: An update on diagnosis and management. World Journal of Nephrology. 2012;1(4): doi: /wjn.v1.i prophylactic antibiotic administration before catheter placement, adequate patient training, exit-site care.")
37
Northshore-Wellbound
An outpatient training and management clinic for home dialysis Started Current PD population: 75 patients Peritonitis rates: 0.21 patient-years between

38
Peritonitis Rates in Patient-Years

39
Peritonitis Rates in Patient-Years

40
Peritonitis “A team approach for continuous quality improvement (CQI) is the key to a successful PD program”
 is the key to a successful PD program")
41
Treatment GOAL: rapid resolution of inflammation to preserve peritoneal membrane function Empiric antibiotic broad spectrum antibiotics to cover gram negative and gram positive organisms Bender FH, Bernardini J, Piraino B. Prevention of infectious complications in peritoneal dialysis: best demonstrated practices. Kidney Int Suppl. 2006;70:S44–S54. Campos RP, Chula DC, Riella MC. Complications of the peritoneal access and their management. Contrib Nephrol. 2009;163:183–197. Dalrymple LS, Johansen KL, Chertow GM, Cheng SC, Grimes B, Gold EB, Kaysen GA. Infection-related hospitalizations in older patients with ESRD. Am J Kidney Dis. 2010;56:522–530.

42
Current Guidelines Per ISPD 2016:
“IP antibiotics be the preferred route of administration unless the patient has features of systemic sepsis (1B).” “…empirical antibiotic therapy be initiated as soon as possible after appropriate microbiological specimens have been obtained (1C).” “…empirical antibiotic regimens be center-specific and cover both gram-positive and gram-negative organisms (1C).” “…gram-positive organisms be covered by vancomycin or a first generation cephalosporin (1B)” “…gram-negative organisms by a third-generation cephalosporin or an aminoglycoside(1B).” ISPD international society of peritoneal dialysis
. …empirical antibiotic therapy be initiated as soon as possible after appropriate microbiological specimens have been obtained (1C). …empirical antibiotic regimens be center-specific and cover both gram-positive and gram-negative organisms (1C). …gram-positive organisms be covered by vancomycin or a first generation cephalosporin (1B) …gram-negative organisms by a third-generation cephalosporin or an aminoglycoside(1B). ISPD international society of peritoneal dialysis.")
43
A study of treatment success of inpatient peritonitis was conducted
From a retrospective review of 71 inpatient peritonitis cases Primary outcome was to determine whether initial, empiric treatment with vancomycin or cefazolin in inpatient PD patients with peritonitis had effect on the rate of clinical resolution of infection caused by gram positive organisms

44
Vancomycin had statistical and clinically significant benefits over cefazolin
Compared outcomes when using vancomycin or cefazolin for gram + infection Excluded gram negative organisms, “no growth” Darya Kupershteyn, PharmD, Mira Suseno, PharmD, BCPS-ID, George Kim, MD, L Tammy Ho, MD, Kevin Nash, MD

45
Current empiric out patient treatment of PD associated peritonitis
Peritonitis empiric protocols: 1g cefazolin IP 1g ceftazidime IP Fluconazole +/- at physician discretion There is a disconnect between OP and IP treatment protocols The patient pool is the same as Wellbound

46
Clinical Questions of Current Study
What are the current rates of failure amongst patients being treated with empiric cefazolin and ceftazidime? Is our rationale for avoiding Vancomycin use reasonable? Concern for VRE rates

47
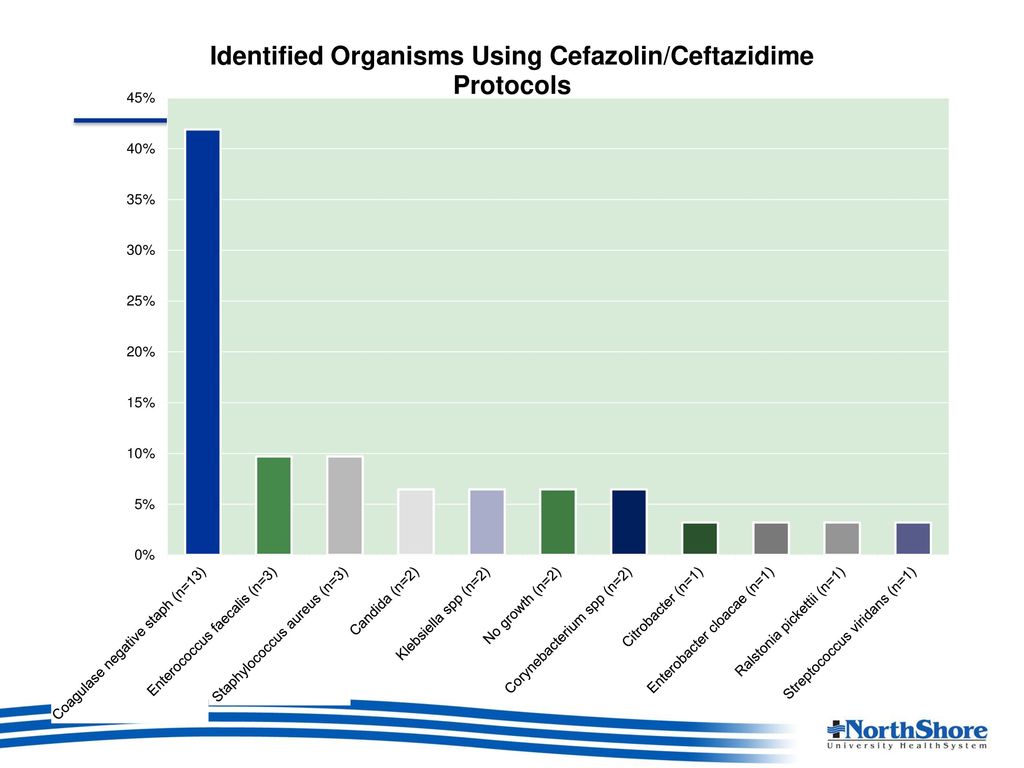
Objectives Primary objective Secondary objectives
To assess failure rates of current empiric treatments with cefazolin and ceftazidime Secondary objectives Identification of the most common outpatient organisms Assess rates of repeat, recurrent, relapsing or refractory peritonitis with current empiric treatments Assess peritonitis hospital admission rates

48
Methods Empiric Treatment failure defined as any of the following subsets: Hospitalization Switching antibiotics: for any reason including resistance, intolerance to medications Removal of peritoneal dialysis catheter Recurrence: episode that occurs within 4 weeks of completion of therapy of a prior episode but with a different organism Relapse: episode that occurs within 4 weeks of completion of therapy of a prior episode with the same organism or one sterile episode Refractory failure: failure of the effluent to clear after 5 days of appropriate antibiotics Hospitalization for peritonitis related complications

49
Methods Retrospective chart review of outpatient Wellbound/Northshore patients on peritoneal dialysis treated for peritonitis between 1/1/2010 and 6/1/2016 Multiple infections on the same patient are treated as independent events

50
Methods Inclusion Criteria Age >18
Receiving outpatient peritoneal dialysis at Wellbound Diagnosed peritonitis Defined as 2 or more of the following: Abdominal pain or cloudy peritoneal dialysis effluent (PDE) White blood cell count >100/mL in PDE Positive gram stain or culture from PDE peritoneal inflammation leading to hyperaemia and changes in peritoneal transport
 White blood cell count >100/mL in PDE. Positive gram stain or culture from PDE. peritoneal inflammation leading to hyperaemia and changes in peritoneal transport.")
51
Non-protocol treatment
Results Variable Protocol treatment Non-protocol treatment Patients [n(%)] 22 36 Cases [n(%)] 27 46 Sex [n(% men)] 17(63%) 33(62.3%) Mean age (range) 65.0 62.0 APD use 25 (92.6%) 42 (91.0%) Of the non-protocol: - 2 prior allergies to medications - (quantify ED treated cases) -
] Cases [n(%)] Sex [n(% men)] 17(63%) 33(62.3%) Mean age (range) APD use. 25 (92.6%) 42 (91.0%) Of the non-protocol: - 2 prior allergies to medications. - (quantify ED treated cases) -")
52
Non-protocol treatment
Results Variable Protocol treatment Non-protocol treatment Recurrence [n(%)] 2 (7.4%) 3 (6.5%) Relapse [n(%)] 2 (4.3%) PD catheter removal [n(%)] 4 (14.8%)
] 2 (7.4%) 3 (6.5%) Relapse [n(%)] 2 (4.3%) PD catheter removal [n(%)] 4 (14.8%)")
53
Li PK, Szeto CC, Piraino B, Bernardini J, Figueiredo AE, Gupta A, et al. Peritoneal dialysis-related infections recommendations: 2010 update. Perit Dial Int 2010; 30:393–423 [Erratum in: Perit Dial Int 2011; 31:512] [PubMed]

54
Clinical Questions of Current Study
What are the current rates of failure amongst patients being treated with empiric cefazolin and ceftazidime? Is our rationale for avoiding Vancomycin use reasonable? Concern for VRE rates

55
Results: Failure in those receiving empiric antibiotic protocol as OP
Variable Protocol treatment Cases [n(%)] 27 Treatment failure [n(%)] 13 (48%) Hospitalization 9 (33%) Recurrences 2 (7.4%) Relapse Medication change 10 (37%) Catheter removal 4 (14.8%) 2 recurrences – different patients one each. Both involved enterococcus candida or corynebacterium 2 relapses – from same patient. The relapses were MSSA Enterococcal and candida infections were automatic failures
] 27. Treatment failure [n(%)] 13 (48%) Hospitalization. 9 (33%) Recurrences. 2 (7.4%) Relapse. Medication change. 10 (37%) Catheter removal. 4 (14.8%) 2 recurrences – different patients one each. Both involved enterococcus candida or corynebacterium. 2 relapses – from same patient. The relapses were MSSA. Enterococcal and candida infections were automatic failures.")
57
Comparisons of susceptibilities
Cefazolin % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases 72% Streptococcus viridans (n=1) *All staph aureus cultures were MSSA
 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases. 72% Streptococcus viridans (n=1) *All staph aureus cultures were MSSA.")
58
Comparisons of susceptibilities
Cefazolin % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) - 35% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA
 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases. 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) - 35% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA.")
59
Comparisons of susceptibilities
Cefazolin Ceftazidime % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% - Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) 35% 98% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA
 83% 62% - Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases. 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) 35% 98% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA.")
60
Comparisons of susceptibilities
Cefazolin Ceftazidime % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% - Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) 35% 98% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA
 83% 62% - Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus* (n=3) 100% No cases. 72% Streptococcus viridans (n=1) Klebsiella spp (n=2) 35% 98% Citrobacter koseri (n=1) 88% *All staph aureus cultures were MSSA.")
61
Degree of Vancomycin susceptibility of organisms cultured in OP protocol treated peritonitis
Cefazolin % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus (n=3) 100% Streptococcus viridans (n=1) ND Nnt = 1.3? *adequately covered by ceftazidime
 83% 62% Enterococcus faecalis (n=3) 0% (IR) Staphylococcus aureus (n=3) 100% Streptococcus viridans (n=1) ND. Nnt = 1.3 *adequately covered by ceftazidime.")
62
Degree of Vancomycin susceptibility of organisms cultured in OP protocol treated peritonitis
Cefazolin Vancomycin % Susceptible in protocol treated % Susceptible NS antibiogram Coagulase-negative staphylococci (n=12) 83% 62% 100% MSSA Enterococcus faecalis (n=3) 0% (IR) 97% Staphylococcus aureus (n=3) Streptococcus viridans (n=1) ND Nnt = 1.3? *adequately covered by ceftazidime
 83% 62% 100% MSSA. Enterococcus faecalis (n=3) 0% (IR) 97% Staphylococcus aureus (n=3) Streptococcus viridans (n=1) ND. Nnt = 1.3 *adequately covered by ceftazidime.")
63
Clinical Questions of Current Study
What are the current rates of failure amongst patients being treated with empiric cefazolin and ceftazidime? Is our rationale for avoiding Vancomycin use reasonable? Concern for VRE rates

64
Trend of Enterococci Susceptibility 2002-2016

65
Trend of Enterococci Susceptibility 2002-2016

66
Discussion Current outpatient protocol for empiric treatment is associated with failure in 48% patients Again defined as hospitalization and antibiotic changes This is despite that the susceptibilities to cefazolin of OP cultured coagulase negative Staph is better than seen on the in patient level Trend of VRE has not increased in the last 14 years The majority of patients with OP peritonitis are sent to the ED for initial evaluation and are admitted

67
Discussion No one died from a peritonitis event Limitations
We could obtain other quantifiable morbidity data aside from hospitalizations, catheter removal or antibiotic changes Limitations Tiny sample size (far fewer cases of peritonitis in general) Single center No population data No adequate comparison
 Single center. No population data. No adequate comparison.")
68
Conclusions This was a quality assurance study looking at whether current out patient empiric antibiotic protocols effectively treated outpatient PD-associated peritonitis Do the very low rates of peritonitis in general lead to a sicker sub-group of patients on presentation? Do nurses feel less comfortable with more ill patients and send to ED for evaluation GI hx and peritonitis - Yip T, Tse KC, Lam MF, Cheng SW, Lui SL, Tang S, et al. Colonic diverticulosis as a risk factor for peritonitis in Chinese peritoneal dialysis patients. Perit Dial Int 2010; 30(2):187–91.
:187–91.")
69
References Ballinger AE Treatment for peritoneal dialysis-associated peritonitis. Cochrane Database Syst Rev 2014; 4:CD Li PKT, Szeto CC, Piraino B, Bernardini J, Figueiredo A, Gupta A, Johnson DW, Kuijper EJ, Lye WC, Salzer W, Schaefer F, Struijk DG PDI 2010; 30: (for epidemiology) Bender FH, Bernardini J, Piraino B. Prevention of infectious complications in peritoneal dialysis: best demonstrated practices. Kidney Int Suppl. 2006;70:S44–S54. Macchini F, Valadè A, Ardissino G, Testa S, Edefonti A, Torricelli M, Luzzani S. Chronic peritoneal dialysis in children: catheter related complications. A single centre experience. Pediatr Surg Int. 2006;22:524–528. Campos RP, Chula DC, Riella MC. Complications of the peritoneal access and their management. Contrib Nephrol. 2009;163:183–197. Dalrymple LS, Johansen KL, Chertow GM, Cheng SC, Grimes B, Gold EB, Kaysen GA. Infection-related hospitalizations in older patients with ESRD. Am J Kidney Dis. 2010;56:522–530. Beth Piraino, Perit Dial Int November-December 2011 31: ; published ahead of print August 31, 2011, doi: /pdi Keane WF, Bailie GR, Boeschoten E, Gokal R, Golper TA, Holmes CJ, Kawaguchi Y, Piraino B, Riella M, Vas S, International Society for Peritoneal Dialysis SOPerit Dial Int. 2000;20(4):396. Bianchi P, Buoncristiani E, Buoncristiani U. Antisepsis. Contrib Nephrol. 2007;154:1–6. Brook NR, White SA, Waller JR, Nicholson ML. The surgical management of peritoneal dialysis catheters. Ann R Coll Surg Engl. 2004;86:190–195. Renaud CJ, Subramanian S, Tambyah PA, Lee EJ. The clinical course of rapidly growing nontuberculous mycobacterial peritoneal dialysis infections in Asians: A case series and literature review. Nephrology (Carlton) 2011;16:174–179. Gupta S, Muralidharan S, Gokulnath H. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in southern India using an automated blood culture system to culture peritoneal dialysate. Nephrology (Carlton) 2011;16:63–67. Davies S. Clinical practice guidelines module 3b: peritoneal dialysis, UK Renal Association Third Edition, 2006. Akoh JA. Peritoneal dialysis associated infections: An update on diagnosis and management. World Journal of Nephrology. 2012;1(4): doi: /wjn.v1.i4.106.
 Bender FH, Bernardini J, Piraino B. Prevention of infectious complications in peritoneal dialysis: best demonstrated practices. Kidney Int Suppl. 2006;70:S44–S54. Macchini F, Valadè A, Ardissino G, Testa S, Edefonti A, Torricelli M, Luzzani S. Chronic peritoneal dialysis in children: catheter related complications. A single centre experience. Pediatr Surg Int. 2006;22:524–528. Campos RP, Chula DC, Riella MC. Complications of the peritoneal access and their management. Contrib Nephrol. 2009;163:183–197. Dalrymple LS, Johansen KL, Chertow GM, Cheng SC, Grimes B, Gold EB, Kaysen GA. Infection-related hospitalizations in older patients with ESRD. Am J Kidney Dis. 2010;56:522–530. Beth Piraino, Perit Dial Int November-December : ; published ahead of print August 31, 2011, doi: /pdi Keane WF, Bailie GR, Boeschoten E, Gokal R, Golper TA, Holmes CJ, Kawaguchi Y, Piraino B, Riella M, Vas S, International Society for Peritoneal Dialysis SOPerit Dial Int. 2000;20(4):396. Bianchi P, Buoncristiani E, Buoncristiani U. Antisepsis. Contrib Nephrol. 2007;154:1–6. Brook NR, White SA, Waller JR, Nicholson ML. The surgical management of peritoneal dialysis catheters. Ann R Coll Surg Engl. 2004;86:190–195. Renaud CJ, Subramanian S, Tambyah PA, Lee EJ. The clinical course of rapidly growing nontuberculous mycobacterial peritoneal dialysis infections in Asians: A case series and literature review. Nephrology (Carlton) 2011;16:174–179. Gupta S, Muralidharan S, Gokulnath H. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in southern India using an automated blood culture system to culture peritoneal dialysate. Nephrology (Carlton) 2011;16:63–67. Davies S. Clinical practice guidelines module 3b: peritoneal dialysis, UK Renal Association Third Edition, Akoh JA. Peritoneal dialysis associated infections: An update on diagnosis and management. World Journal of Nephrology. 2012;1(4): doi: /wjn.v1.i")
70
misc Attrition rate Chicago PD epidemiology
Davita/fresinius information Prophylactic antibiotics - people who undergo dental procedures and colonoscopy Adequacy after infection Northshore empiric protocol

71
misc A lack of adequate physician training
Provider infrastructure-related issues Unanticipated financial incentives that had favored use of in-center HD.

72
misc Yip T, Tse KC, Lam MF, Cheng SW, Lui SL, Tang S, et al. Colonic diverticulosis as a risk factor for peritonitis in Chinese peritoneal dialysis patients. Perit Dial Int 2010; 30(2):187–91. (gut in older patients with PD)
:187–91. (gut in older patients with PD)")
73
misc PD function A single, isolated episode of peritonitis (n = 86) had no significant effect on longitudinal peritoneal function, whereas recurrences or clusters of infection (n = 70) caused increases in dialysate/plasma ratio of creatinine and reductions in ultrafiltration, the significance of which increased with the number of episodes. Davies et al[115] demonstrated that solute transfer increases and ultrafiltration declines with time on PD. This process is exacerbated and accelerated by peritonitis, and appears to be proportional to the degree of associated inflammation and number of infections in close proximity.
 had no significant effect on longitudinal peritoneal function, whereas recurrences or clusters of infection (n = 70) caused increases in dialysate/plasma ratio of creatinine and reductions in ultrafiltration, the significance of which increased with the number of episodes. Davies et al[115] demonstrated that solute transfer increases and ultrafiltration declines with time on PD. This process is exacerbated and accelerated by peritonitis, and appears to be proportional to the degree of associated inflammation and number of infections in close proximity.")
74
Comparison of Arterial and Venous Blood Gases: Correlation in a General Patient Population
Paul Chung, DO Anthony Scavone, DO, Asrar Ahmed, DO, Kristine Kuchta, MS, Shashi Bellam, MD Research Grand Rounds

75
Disclosures No financial disclosures
Poster presented at: International ATS Conference 2016, San Francisco, CA

76
Objectives Review previous literature
Review correlation of arterial and venous blood gases Review data on using venous blood gas as a screening tool

77
Background Blood gas analysis is an important part of the assessment of severe respiratory and metabolic derangements Acid-base Ventilation Oxygen

78
Background Arterial blood gas is gold standard
Problems with obtaining an ABG: Technically difficult Increase patient discomfort (additional needle stick) Arterial injury, hemorrhage and hematoma Thrombosis and ischemic injury to digits Infection Median nerve injury Reflex sympathetic dystrophy Can venous blood gas replace arterial blood gas analysis?
 Arterial injury, hemorrhage and hematoma. Thrombosis and ischemic injury to digits. Infection. Median nerve injury. Reflex sympathetic dystrophy. Can venous blood gas replace arterial blood gas analysis")
79
Background Previous studies have shown mixed results
Specific patient populations Trauma Lumbar surgery DKA COPD Specific locations Emergency Room ICU

80
Background Meta-analyses comparing VBG to ABG Zeserson et al. 2016.
Byrne et al pH compared well pCO2 sufficiently different Bloom et al pH and –HCO3 agree reasonably well pCO2 agree poorly Zeserson et al VBG plus SpO2 accurate for undifferentiated critically ill patients

81
Purpose What is the correlation of arterial and venous blood gases in a general population? Does the correlation change at extremes of pH and pCO2? Can venous blood gas analysis replace arterial blood gas analysis? Can venous blood gases be used as a screening tool?

82
Methods Retrospective, observational study
January 1, 2006 to May 1, 2017 Inclusion criteria: Arterial and venous blood gases in the same patient obtained within 30 min of each other Deidentified data

83
Results Mean time between ABG and VBG: 2713 paired pH results
± min 2713 paired pH results 2817 paired pCO2 results 2864 paired -HCO3 results 0.7 to 1.0 – strong 0.5 to 0.7 – moderate 0.3 to 0.5 – weak 0.1 to 0.3 – poor/none Evans (1996) 0.0 to 0.19 – very weak 0.2 to 0.39 – weak 0.4 to 0.59 – moderate 0.6 to 0.79 – strong 0.8 to 1.0 – very strong
 0.0 to 0.19 – very weak. 0.2 to 0.39 – weak. 0.4 to 0.59 – moderate. 0.6 to 0.79 – strong. 0.8 to 1.0 – very strong.")
84
pH Pearson Correlation (p<0.001)
")
85
pH Mean Difference: (95% CI: , )
")
86
pH pH N Pearson Correlation p-value VBG<7.35 1652 0.7682 <0.0001
925 0.7599 VBG<7.20 277 0.7804 ABG <7.35 >=7.35 VBG 1185 467 171 890 Sensitivity 87.4% Specificity 65.6% Negative Predictive Value 83.9% Positive Predictive Value 71.7%

87
pCO2 Pearson Correlation (p<0.001)
")
88
pCO2 Mean Difference: (95% CI: , )
")
89
pCO2 pCO2 N Pearson Correlation P-value VBG>45 1161 0.6848
<0.0001 VBG>50 640 0.7153 VBG>60 205 0.6929 ABG <45 >=45 VBG 1380 249 561 627 Sensitivity 71.1% Specificity 71.6% Negative Predictive Value 52.8% Positive Predictive Value 84.7% ABG <45 >=45 VBG <30 182 2 >=30 1759 874 Sensitivity 9.4% Specificity 99.8% Negative Predictive Value 33.2% Positive Predictive Value 98.9%

90
-HCO3 Pearson Correlation (p<0.001)
")
91
-HCO3 Mean Difference: (95% CI: , )
")
92
Discussion Venous pH Good correlation when all values included
Correlation decreases for pH<7.35 (acidemia) Confidence interval large enough to affect management Useful for screening VBG pH>7.35: no need for confirmatory ABG VBG pH<7.35: confirm with ABG
 Confidence interval large enough to affect management. Useful for screening. VBG pH>7.35: no need for confirmatory ABG. VBG pH<7.35: confirm with ABG.")
93
Discussion Venous pCO2 Good correlation when all values included
Moderate correlation with pCO2>45mmHg Confidence intervals markedly large and cannot accurately replace an ABG Useful for screening pCO2<45mmHg: 71.0% sensitive pCO2<30mmHg: 98.9% ppv for arterial pCO2<45mmHg

94
Discussion -HCO3 Excellent correlation No other testing done
Calculated value Accurate measurement of –HCO3 with basic labs

95
Limitations Retrospective, observational study
Central versus peripheral VBG not differentiated Deidentified data – no sub-population analysis

96
Conclusions VBGs can be used as a screening tool
A venous pH < 7.35 or pCO2 > 30mmHg cannot reliably replace arterial blood measurements

97
References Kelly AM, Mcalpine R, Kyle E. Venous pH can safely replace arterial pH in the initial evaluation of patients in the emergency department. Emerg Med J. 2001;18(5):340-2. Malatesha et al. Comparison of arterial and venous pH, bicarbonate, PCO2, and PO2 in initial emergency department assessment. Emerg Med J. 2007;24(8): Malinoski DJ, Todd SR, Slone S, Mullins RJ, Schreiber MA. Correlation of central venous and arterial blood gas measurements in mechanically ventilated trauma patients. Arch Surg. 2005;140(11): Rudkin SE, Kahn CA, Oman JA, et al. Prospective correlation of arterial vs venous blood gas measurements in trauma patients. Am J Emerg Med. 2012;30(8): Khan ZH, Samadi S, Sadeghi M, et al. Prospective study to determine possible correlation between arterial and venous blood gas values. Acta Anaesthesiol Taiwan. 2010;48(3):136-9. Brandenburg MA, Dire DJ. Comparison of arterial and venous blood gas values in the initial emergency department eevaluation of patients with diabetic ketoacidosis. Ann Emerg Med. 1998;31(4): Kelly AM. The case for venous rather than arterial blood gases in diabetic ketoacidosis. Emerg Med Australas. 2006;18(1):64-67. Gokel Y, Paydas S, Koseoglu Z, Alparslan N, Seydaoglu G.Comparison of blood gas and acid-base measurements in arterial and venous blood samples in patients with uremic acidosis and diabetic ketoacidosis in the emergency room. Am J Nephrol. 2000;20(4): McCanny P, Bennett K, Staunton P, McMahon G. Venous vs arterial blood gases in the assessment of patients presenting with an exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2012;30(6): McKeever TM, Hearson G, Housley G, et al. Using venous blood gas analysis in the assessment of COPD exacerbations: a prospective cohort study. Thorax. 2016;71(3):210-5. Zeserson E, Goodgame B, Hess JD, et al. Correlation of venous blood gas and pulse oximetry with arterial blood gas in the undifferentiated critically ill patient. J Intensive Care Med doi: / Treger et al. Agreement between central venous and arterial blood gas measurements in the intensive care unit. Clin J Am Soc Nephrol. 2010;5(3):390-4. Byrne AL, Bennett M, Chatterji R, Symons R, Pace NL, Thomas PS. Peripheral venous and arterial blood gas analysis in adults: are they comparable? A systematic review and meta-analysis. Respirology. 2014;19(2): Bloom BM, Grundlingh J, Bestwick JP, Harris T. The role of venous blood gas in the emergency department: a systematic review and meta-analysis. Eur J Emerg Med. 2014;21(2):81-8. Kelly AM, Kyle E, McAlpine R. Venous pCO2 and pH can be used to screen for significant hypercarbia in emergency patients with acute respiratory disease. J Emerg Med. 2002;22(1):15-19. Kelly AM, Kerr D, Middleton P. Validation of pCO2 to screen for arterial hypercarbia in patients with chronic obstructive airways disease. J Emerg Med. 2005;28(4): Ibrahim I, Ooi SB, Yiong Huak C, Sethi S. Point-of-care bedside gas analyzer: limited use of venous pCO2 in emergency patients. J Emerg Med. 2011;41(2):
: Malatesha et al. Comparison of arterial and venous pH, bicarbonate, PCO2, and PO2 in initial emergency department assessment. Emerg Med J. 2007;24(8): Malinoski DJ, Todd SR, Slone S, Mullins RJ, Schreiber MA. Correlation of central venous and arterial blood gas measurements in mechanically ventilated trauma patients. Arch Surg. 2005;140(11): Rudkin SE, Kahn CA, Oman JA, et al. Prospective correlation of arterial vs venous blood gas measurements in trauma patients. Am J Emerg Med. 2012;30(8): Khan ZH, Samadi S, Sadeghi M, et al. Prospective study to determine possible correlation between arterial and venous blood gas values. Acta Anaesthesiol Taiwan. 2010;48(3): Brandenburg MA, Dire DJ. Comparison of arterial and venous blood gas values in the initial emergency department eevaluation of patients with diabetic ketoacidosis. Ann Emerg Med. 1998;31(4): Kelly AM. The case for venous rather than arterial blood gases in diabetic ketoacidosis. Emerg Med Australas. 2006;18(1): Gokel Y, Paydas S, Koseoglu Z, Alparslan N, Seydaoglu G.Comparison of blood gas and acid-base measurements in arterial and venous blood samples in patients with uremic acidosis and diabetic ketoacidosis in the emergency room. Am J Nephrol. 2000;20(4): McCanny P, Bennett K, Staunton P, McMahon G. Venous vs arterial blood gases in the assessment of patients presenting with an exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2012;30(6): McKeever TM, Hearson G, Housley G, et al. Using venous blood gas analysis in the assessment of COPD exacerbations: a prospective cohort study. Thorax. 2016;71(3): Zeserson E, Goodgame B, Hess JD, et al. Correlation of venous blood gas and pulse oximetry with arterial blood gas in the undifferentiated critically ill patient. J Intensive Care Med doi: / Treger et al. Agreement between central venous and arterial blood gas measurements in the intensive care unit. Clin J Am Soc Nephrol. 2010;5(3): Byrne AL, Bennett M, Chatterji R, Symons R, Pace NL, Thomas PS. Peripheral venous and arterial blood gas analysis in adults: are they comparable A systematic review and meta-analysis. Respirology. 2014;19(2): Bloom BM, Grundlingh J, Bestwick JP, Harris T. The role of venous blood gas in the emergency department: a systematic review and meta-analysis. Eur J Emerg Med. 2014;21(2):81-8. Kelly AM, Kyle E, McAlpine R. Venous pCO2 and pH can be used to screen for significant hypercarbia in emergency patients with acute respiratory disease. J Emerg Med. 2002;22(1): Kelly AM, Kerr D, Middleton P. Validation of pCO2 to screen for arterial hypercarbia in patients with chronic obstructive airways disease. J Emerg Med. 2005;28(4): Ibrahim I, Ooi SB, Yiong Huak C, Sethi S. Point-of-care bedside gas analyzer: limited use of venous pCO2 in emergency patients. J Emerg Med. 2011;41(2):")
Similar presentations

>")



, ranging in severity: Acute bronchitis - an acute respiratory tract infection in.>")







 criteria A single center cohort study Figure 2 The acute kidney injury network (AKIN) criteria.>")


 26: 537–543 2.J Support Oncol 2011;9:149–155 3.N Engl J Med. 2009; 361:1627–1638.>")



