Download presentation
Presentation is loading. Please wait.

1
Dr David Highton Anaesthetic Registrar UCL Hospitals Fluids An Introduction to Anaesthesia 2016

2
Blood

3
Outline Blood – Why? – How? – Who? – Risks – Haemmorrhage Gaius Plinius Secundus (AD 23 – AD 79)
")
4
A fit patient with a compound fracture of the tibia and a post operative Hb of 7.5 g/dl should be transfused?

5
A 70yr old woman with a history of angina and a pre-op Hb of 7.5 g/dl should be transfused?

6
Why? Blood is essential for life – carries O2 The body at rest uses approx 250ml O2/L blood Oxygen delivery to tissues (O2 Flux) = Cardiac Output x Oxygen content of blood Hb x Sa0 2 Organs most sensitive to hypoxia are Heart and Brain
 = Cardiac Output x Oxygen content of blood Hb x Sa0 2 Organs most sensitive to hypoxia are Heart and Brain.")
7
How? Patient Blood Management: “evidence-based, multidisciplinary approach to optimise the care of patients who might need transfusion…” Preoperative – Detection of anaemia, optimisation Hb Intraoperative – Blood conservation Tranexamic acid/ Cell salvage/ Surgical technique/ Warming – Transfusion triggers Patients ability to compensate for anaemia ( cardiorespiratory disease) Rate of ongoing blood loss Likelihood of further blood loss Balance of risks vs benefits of transfusion Postoperative – Single unit transfusion policy
 Rate of ongoing blood loss Likelihood of further blood loss Balance of risks vs benefits of transfusion Postoperative – Single unit transfusion policy.")
9
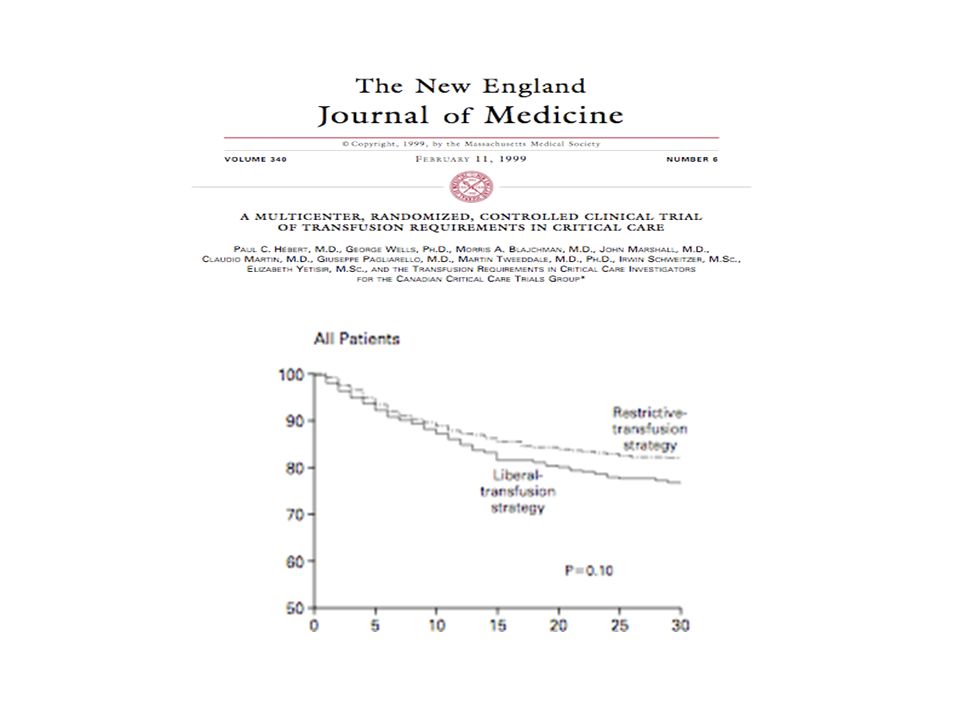
Transfusion Triggers Hb >10NO Hb < 7YES Hb 7-10 MAYBE – Cardiopulmonary reserve needs to be assessed. – Symptomatic patients should be transfused. (fatigue, dizziness, shortness of breath, new or worsening angina)
.")
10
Risks French physician Jean-Baptiste Denys

11
A fit patient with a compound fracture of the tibia and a post operative Hb of 7.5 g/dl should be transfused? T F

12
A fit patient with a compound fracture of the tibia and a post operative Hb of 7.5 g/dl should be transfused? T F ✔

13
A 70yr old woman with a history of angina and a pre-op Hb of 7.5 g/dl should be transfused? T F

14
A 70yr old woman with a history of angina and a pre-op Hb of 7.5 g/dl should be transfused? T ✔ F

15
Summary Minimise blood loss Think before you transfuse! Does your patient really need blood? Weigh up the benefits vs risks of transfusion.

16
Massive Transfusion

17
Settings – Obstetric – Trauma – Surgical – Medical

18
Definitions Replacement of one blood volume in a 24 hour period Transfusion of >10 units in 24 hours Transfusion of 4 or more units within 1 hour when ongoing need is foreseeable Replacement of >50% of the total blood volume within 3 hours Obstetrics – >2000mls – >150mls/min – Uncontrolled/ ongoing

19
Get some Help…. CODE RED/ CODE BLUE Senior anaesthetist/ surgeon/ obstetrician Blood Bank Haematologist Porter Get someone to coordinate to communicate and document

20
CODE RED Code Red Pack A: – 6 units RBC – 4 units FFP Code Red Pack B: – 6 units RBC – 4 units FFP – 1 pool platelets – 2 pools cryoprecipitate

21
The Massively Bleeding Patient… Stop the bleeding Restore Circulating Volume: – Two 14G IV cannulae – Resuscitate with warmed crystalloid/colloid – Warm patient – Consider invasive monitoring: arterial line + central venous access

22
Request Lab investigations FBC, ABG Coagulation screen X- match Repeat after products/4hourly May need to give blood products before results are available

23
The Perfect Clot! Red blood Cells Platelets Clotting factors Fibrinogen

24
“Bloody Vicious Cycle”

25
Effect of Hypothermia on coagulation factor activity

26
Request PRC Uncrossmatched Group O Rh neg Uncrossmatched ABO group specific Fully X match Use a blood warmer/ rapid infusion device Tranexamic acid Consider cell salvage

27
Clotting products Platelets – Target plt count>100 x10 9 /l for multiple/CNS trauma, > 50 in other situations FFP – Aim for PT/ APTT < 1.5 x control Cryoprecipitate – Aim for fibrinogen >1g/L

28
Summary Recognise! Communicate! Code call! Get help! Beware hypothermia/acidosis/ haemodilution and coagulopathy

29
Other IV Fluids IV Fluids

30
Normal Adult Fluid Composition 60% composed of water 70 kg person= 42 L 2/3 ICF = 28L 1/3 ECF = 14L Total Body Water = ECF + ICF ECF = Plasma 3 L + IF 10-11 L

31
Daily Requirements Paediatrics: 4 ml/kg/h for the first 10 kg 2 ml/kg/h for the next 10 kg 1 ml/kg/h for every kg over 20 kg Adult: 25-30ml/kg/day 1 mmol/kg/day Na, K +, Cl- 50-100 g/day glucose (5% glucose contains 5 g/100ml)
")
33
Algorithm 1: Assessment – ABCDE Algorithm 2: Resuscitation – 500ml crystolloid bolus over 15 mins up to 2L – Call for help

34
Algorithm 1: further assessment – History – Clinical examination – Clinical monitoring – Lab – Can the patient meet needs orally/ enterally? – Complex replacement or distribution issues?

35
– Algorithm 3: Routine maintenance Algorithm 4: Replacement and Redistribution – Fluid/ electrolyte deficits or excesses? – Abnormal fluid/ electrolyte losses?

36
Pre-operative protocols Starvation Protocol: – Starved for 6 hours – Can take clear fluids up to 2 hrs before surgery – Carbohydrate rich drink up to 2 hrs before

37
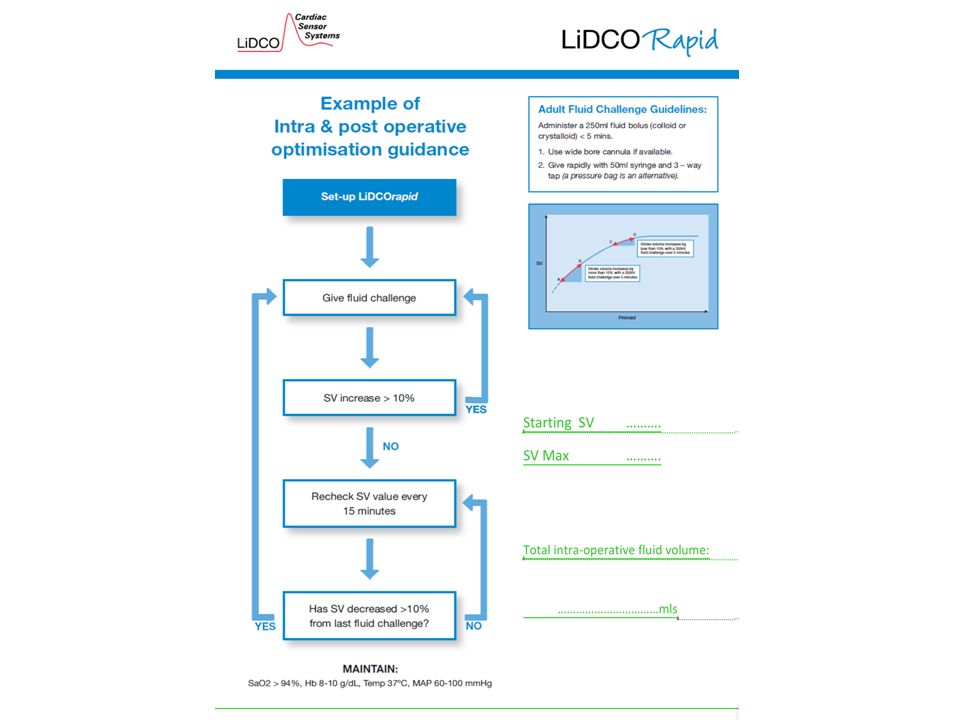
Intra-operatively Estimate requirements Goal directed fluid therapy? – Cardiac output monitoring or surrogates

39
Post- operatively Provide maintenance requirements Stop iv fluids when no longer needed NG fluids or enteral feeding is preferable if >3 days.

40
Crystalloids Contain water and dissolved electrolytes Pass freely through a semipermeable membrane Need larger volumes Cheap

41
Colloids Contain large molecules suspended in a carrier solution Large molecules stay in the plasma, keeping infused fluid largely in circulation. Smaller volumes needed Small risk of anaphylaxis No starches in UK now

42
Elective, well patient Q: Fit, young 60kg pt having elective superficial surgery, what fluid losses do you expect before and during surgery of less than an hour?

43
Do you need to give fluid? Starved 6 hrs Deficit: 30ml/kg/day, 6 hrs = 450ml Intra op losses 1 ml/kg/hr = 60ml 510ml total Probably doesn’t need fluid Feel better? Less PONV? Put up a bag! Much easier to flush through drugs and check your drip is working.

44
Emergency Laparotomy Pt Q: Patient needing urgent laparotomy, history of vomiting for several days. Do they need fluid? Yes lots! Resuscitate Water and electrolytes – H+, Cl- loss – K+ replacement Check serum electrolytes before and after fluid resuscitation

45
Summary Think about why you are giving fluids Work out how much fluid to give Select what type of fluid to give Monitor

Similar presentations











 and received 20ml/kg of red cells or 40ml/kg of any.>")








