Download presentation
Presentation is loading. Please wait.

1
Development of Pituitary, Adrenal, Thyroid and Parathyroid Glands Dr. Wai Wai Kyi March 2013 1

2
Objectives Discuss the formation of neural and oral ectoderm ( trilaminar germ disc. Describe the development and their developmental anomalies of: anterior and posterior pituitary gland. adrenal cortex and medulla. thyroid gland. parathyroid gland. 2

3
Introduction All three embryonic germ layers (endoderm, mesoderm, and ectoderm) contribute to the development of the endocrine glands. All secretory glands, whether exocrine or endocrine, develop from epithelia. Endocrine organs develop from the epithelia that cover the outside of the embryo, that lines the digestive tract, and that lines the coelomic cavity. The pituitary gland develop from ectoderm. The adrenal cortex develops from mesoderm where as the adrenal medulla develops from neural crest. The thyroid and parathyroid glands develop from endoderm. 3

4
Development of the pituitary gland 4

5
The pituitary gland develops as a fusion of two groups of cells,upgrowth of ectodermal cells from Rathke's pouch), and a down-growth of The pituitary gland develops as a fusion of two groups of cells,upgrowth of ectodermal cells from Rathke's pouch), and a down-growth of. Infundibulum Stalk of R’s pouch (Degenerating) Hypothalamus Intermediate lobe Ant. Lobe Infundibulum Residual lumen Neural lobe (Former site of R’s stalk) Rathke’s pouch Development of the pituitary gland (Hypophysis) From two different types of ectoderm ■ Oral ectoderm which forms Rathke's pouch. ■ Neural ectoderm which forms the infundibulum. 5
 Hypothalamus Intermediate lobe Ant. Lobe Infundibulum Residual lumen Neural lobe (Former site of R’s stalk) Rathke’s pouch Development of the pituitary gland (Hypophysis) From two different types of ectoderm ■ Oral ectoderm which forms Rathke s pouch. ■ Neural ectoderm which forms the infundibulum. 5.")
6
The pituitary gland ( L- hypophysis) develops from two sources of ectoderm. Pituitary gland is the neuroglandular body. Adenohypophysis (Ant. lobe), glandular part arises from oral ectoderm. An upgrowth of ectodermal roof of stomodeum, the hypophysial diverticulum/Rathke's pouch Neurohypophysis (Post. lobe), nervous part originates from neuroectoderm. A downgrowth from neuroectoderm of the hypothalamus, the neurohypophysial diverticulum 6
, glandular part arises from oral ectoderm. An upgrowth of ectodermal roof of stomodeum, the hypophysial diverticulum/Rathke s pouch Neurohypophysis (Post. lobe), nervous part originates from neuroectoderm. A downgrowth from neuroectoderm of the hypothalamus, the neurohypophysial diverticulum 6.")
7
Stomodeum - a depression between the brain and the pericardium in an embryo, and is the precursor of the mouth and the anterior lobe of the pituitary gland. Buccopharyngeal/ Oropharyngeal membrane The region where the ectoderm and endoderm come into direct contact with each other constitutes a thin membrane. It forms a septum between the primitive mouth and pharynx. 7

9
Pituitary gland (master gland) 9 (Adenohypophysis) (Neurohypophysis)
 9 (Adenohypophysis) (Neurohypophysis)")
10
Adenohypophysis (Ant. lobe) Develops from Rathke's pouch which is an ectodermal diverticulum of the primitive mouth cavity, stomodium. Anterior wall proliferates - pars distalis Posterior wall little growth – pars intermedia Rostral growth around infundibular stem – pars tuberalis Adenohypophysis is formed by development of pars distalis, pars tuberalis, and pars intermedia. 10 (Floor of Diencephalon) (Roof of the mouth)
 Develops from Rathke s pouch which is an ectodermal diverticulum of the primitive mouth cavity, stomodium. Anterior wall proliferates - pars distalis Posterior wall little growth – pars intermedia Rostral growth around infundibular stem – pars tuberalis Adenohypophysis is formed by development of pars distalis, pars tuberalis, and pars intermedia. 10 (Floor of Diencephalon) (Roof of the mouth).")
11
Neurohypophysis (Post. lobe) Neural ectoderm from the base of the diencephalon (hypothalamus) which forms the infundibulum. As development proceeds, the ectoderm of the infundibulum grows downward and wraps around Rathke's pouch. Neurohypophysis is formed by development of pars nervosa, infundibular stem, and median eminence. 11 (Floor of Diencephalon) (Roof of the mouth)
 Neural ectoderm from the base of the diencephalon (hypothalamus) which forms the infundibulum. As development proceeds, the ectoderm of the infundibulum grows downward and wraps around Rathke s pouch. Neurohypophysis is formed by development of pars nervosa, infundibular stem, and median eminence. 11 (Floor of Diencephalon) (Roof of the mouth).")
12
Human embryonic and fetal pituitary Week 4 - Rathke’s pouch/hypophysial pouch Week 5 - elongation, contacts infundibulum, diverticulum of diencephalon Week 6 - connecting stalk between pouch and oral cavity degenerates Week 10 - growth hormone and ACTH detectable Week 16 - adenohypophysis fully differentiated Week 20 to 24 - growth hormone levels peak, then decline 12

13
Congenital malformations ♦ Craniopharyngiomas (Rathke pouch tumors, hypophyseal duct tumors) Arise from remnants of the craniopharyngeal duct/canal or Rathke's pouch Occur in sella, suprasellar region (usually) & along the pituitary stalk They may cause hydrocephalus, pituitary dysfunction ie. diabetes insipidus, growth failure. Tendency to become adherent to structures in and around the pituitary gland and pituitary stalk, including the optic nerves, optic chiasm, intracranial arteries and the brain itself. ♦ Agenesis of pituitary 13

14
♦ Rathke's cleft cyst The lumen of the Rathke's pouch normally closes in fetal development, but a remnant often persists as a cleft that lies between the anterior and posterior lobes of the pituitary gland. Occasionally, this remnant enlarges to form a cyst. RCCs can cause pituitary failure, headaches and in some instances, vision loss. ♦ Pharyngeal hypophysis A small amount of Rathke's pouch persist in the roof of the pharynx Craniopharyngiomas 14

15
Development of thyroid gland 15

16
Branchial/ Pharyngeal arch Gill = Branchial Branchial apparatus ▪ Paired structures associated with the pharynx; a four- week-old embryo consists of the: Bran. arches Bran.pouches (internally) Bran. grooves/cleft(externally) Bran. membranes ▪ Contribute greately to the formation of head & neck ▪ Branchial arch (1, 2, 3, 4 & 6) Neural crest cells migrate into future head and neck Each branchial arch is composed of: 1. Core of lateral mesoderm and neural crest cells 2.Ectoderm externally & 3.Endoderm internally and each is associated with a cranial nerve and an aortic arch. 16
 Bran. grooves/cleft(externally) Bran. membranes ▪ Contribute greately to the formation of head & neck ▪ Branchial arch (1, 2, 3, 4 & 6) Neural crest cells migrate into future head and neck Each branchial arch is composed of: 1. Core of lateral mesoderm and neural crest cells 2.Ectoderm externally & 3.Endoderm internally and each is associated with a cranial nerve and an aortic arch. 16.")
17
Components of branchial/pharyngeal apparatus: Pharyngeal arches (1,2,3 & 4) - mesenchymal tissue surrounded by ectoderm and endoderm Pharyngeal pouches (1,2,3 & 4) - outpouching of endoderm from rostral foregut between adjacent arches. Pharyngeal clefts/grooves (1,2,3 & 4) - ectodermal cleft between adjacent arches. 17
 - ectodermal cleft between adjacent arches. 17.")
18
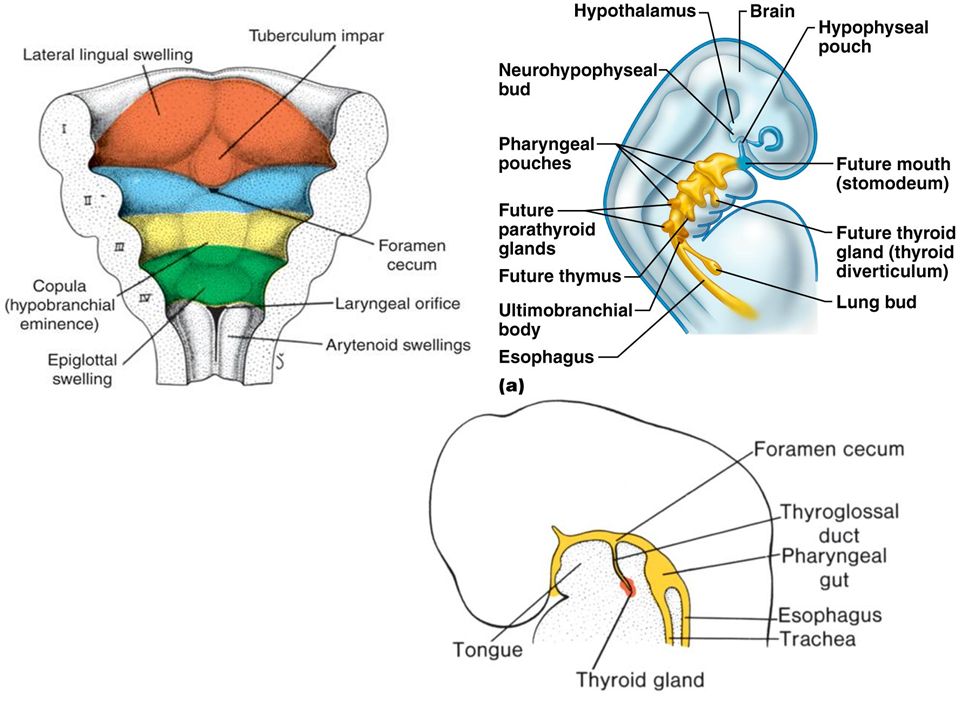
Development of thyroid gland First endocrine gland to develop in the embryo; begin to form 24 days after fertilisation. Thyroid primordium derives from an endodermal thickening that forms a diverticulum in the midline floor of the primitive pharynx between the first and second pharyngeal pouches. The site of this initial development lies between the tuberculum impar and the copula known as the foramen cecum. Migrate caudally along the thyroglossal duct anterior to hyoid and thyroid cartilage. Connected to the tongue by thyroglossal duct Thyroid primordium is hollow becomes solid & divides into rt & lt lobes connected by isthmus which lies ventral to the tracheal rings. 18

20
Development of thyroid gland (Cont.) Week 7: Thyroid reaches final position in front of the trachea; thyroglossal duct has degenerated. Pyramidal lobe: Persistence of distal end of thyroglossal duct, present in 50% of people. Follicular Cells: Secrete T4 and T3, arise from a downward growth of endodermal epithelium. By 11th week contain colloid. Thyroid begin to function at the end of the 3 rd month. Parafollicular Cells (C cells) Secrete calcitonin, arise from ultimobranchial body. The ultimobranchial body arises from ventral swellings of the 4th pharyngeal pouch & 5 th pouch if develops. 20
 Secrete calcitonin, arise from ultimobranchial body. The ultimobranchial body arises from ventral swellings of the 4th pharyngeal pouch & 5 th pouch if develops. 20.")
21
21

22
22

23
Congenital malformations - Ectopic thyroid gland Usually located along its route of descent from tongue. Lingual thyroid (the most common)- failure to descent. - Accessory thyroid arising from remnants of the thyroglossal duct it is generally insufficient for normal function. -Thyroglossal duct cyst Remnant of the duct form cyst. It is the mucous filled sac.Can occur along the path of thyroglossal duct. Located in the midline of the neck; associated with hyoid bone; moves with swallowing. If the cyst ruptures, may form a sinus or fistula It is clinically impt. to differentiate an ectopic thyroid gland from thyroglossal duct cyst or accessory thyroid. Ectopic thyroid may represent only functional thyroid tissue. 23 Thyroglossal duct
- failure to descent. - Accessory thyroid arising from remnants of the thyroglossal duct it is generally insufficient for normal function. -Thyroglossal duct cyst Remnant of the duct form cyst. It is the mucous filled sac.Can occur along the path of thyroglossal duct. Located in the midline of the neck; associated with hyoid bone; moves with swallowing. If the cyst ruptures, may form a sinus or fistula It is clinically impt. to differentiate an ectopic thyroid gland from thyroglossal duct cyst or accessory thyroid. Ectopic thyroid may represent only functional thyroid tissue. 23 Thyroglossal duct.")
24
24 Congenital malformations (Cont.) - Levator glandulae thyroideae muscle may be present along the course of the thyroglossal duct.
 - Levator glandulae thyroideae muscle may be present along the course of the thyroglossal duct.")
25
Ectopic Thyroid TissueThyroglossal cyst Positions of thyroglossal cysts 25 Thyroglossal cyst

26
Development of parathyroid gland 26

27
Development of the parathyoid glands Two dorsal thickenings of the epithelium of the ■ 3rd pharyngeal pouches Inferior parathyroid ■ 4th pharyngeal pouches Superior parathyroid Pharyngeal pouches adult derivatives and descent of the thyroid 27

28
Inferior parathyroid embryology (gestational weeks 5-6) Third pharyngeal pouch ■ Dorsal expansion /wing Inferior parathyroid ■ Ventral expansion /wing thymus ▪ The thymus and parathyroids both lose their connections to the pharynx at gestational week 7. ▪ Initially descends with thymus; therefore inf. parathyroid are further inferior than the sup. parathyroid. ▪The inf. parathyroid glands loses its connection with the thymus and rest on the dorsal surface of the thyroid gland, outside of the fibrous capsule of the gland itself. 28

29
Superior parathyroid embryology (gestational weeks 5-6) Fourth pharyngeal pouch, ■ Dorsal expansion /wing Superior parathyroid ■ Ventral expansion/ wing Ultimobranchial body At gestational week 7, the glands lose connections with the pharynx and attach themselves to the thyroid gland, which is migrating caudally. Because of the lesser length of migration, the sup. parathyroid glands are in a more constant location than the inf. parathyroids. Finally it attach on the dorsal surface of the thyroid gland, outside the fibrous capsule of the thyroid gland. Start producing PT hormone by 7th week (when bones start ossifying); oxyphil cells appear a few years before puberty The fetal parathyroids appear functional. 29
; oxyphil cells appear a few years before puberty The fetal parathyroids appear functional. 29.")
30
30

31
Congenital malformations ▪ Accessory or supernumerary parathyroid glands From tissue fragmentation occurring during the migration of the glands. ▪ Absence of parathyroid Failure of the primordia to differentiate into the parathyroid glands or may be the result of parathyroid gland atrophy early in development. ▪ Ectopic parathyroid glands. The glands may be located anywhere near or even within the thyroid or thymus. ▪ Intrathyroidal parathyroid gland. ▪ DiGeorge syndrome manifests as congenital thymic aplasia and absent parathyroid glands. This syndrome results from failure of the third and fourth brachial pouches to differentiate. It is also associated with facial abnormalities from abnormal development within first arch structures. Teratogens are the assumed mechanism. Symptoms include neonatal tetany and impaired cellular immunity with normal humoral immunity. 31

32
Development of adrenal gland 32

33
Development of the adrenal glands (5th-6th week) The 2 main parts of the adrenals have different embryonic origins. ■ Adrenal medulla is derived from neural crest, ectoderm. ■ Adrenal cortex is derived from mesothelium, mesoderm 33

34
Development of adrenal gland (Cont.) Cortex (Mesodermal) Fetal cortex Adult cortex ▪ Fetal cortex - Develops from coelomic epithelium (mesothelium) that lies between the upper end of mesonephros & root of dorsal mesentery. -Mesothelium proliferate & penetrate the underlying mesenchymal cells & form the fetal adrenal cortex. 34

35
▪ Adult cortex - Formed as fetal cortex - Fetal cortex is replaced by adult cortex; mesothelium mesenchyme encloses fetal cortex. ▪ Fetal cortex functions during fetal period but degenerates soon after birth. ▪ Late fetal period - differentiates to form cortical zones. ▪ Birth - zona glomerulosa, zona fasiculata present. ▪ Year 3 - zona reticularis present. ▪ During fetal development, adrenal hormones are involved with the maturation of the lung and other developing systems. 35

36
Medulla (Neuroectodermal) Cells from the neural crest cells (receiving sympathetic fibers) invade medial aspect of cortex and form the medulla. These chromaffin cells are named because of their staining (yellow) with chromium salts. Peritoneal cavity Sympathetic ganglia 36
 with chromium salts. Peritoneal cavity Sympathetic ganglia 36.")
37
37 Neural crest cells Developing suprarenal Mesonephros Gonad

38
A. The chromaffin (sympathetic) cells penetrating the total cortex of the suprarenal gland. B. At a late stage of development, the definitive cortex surrounds the medulla almost complete. 38

39
Schematic diagram showing the changes in the adrenal gland during development. 39

40
Congenital malformations Adrenogenital syndrome (congenital adrenal hyperplasia) Autosomal recessive syndromes resulting from mutations of genes for enzymes deficiencies in biosynthesis of adrenal steroid hormone. The reduced hormone output results in an increase release of ACTH which causes adrenocortical hyperplasia and overproduction of androgen. An autosomal recessive trait - that it is not manifested unless the trait is inherited from both parents. Symptoms depend on specific defect; include salt wasting (aldosterone cannot be synthetized), musculinization of a female fetus ie. female intersexuality, precocious puberty in boys Female pseudohermaphrodite - premature pubic hair, hypertrophied clitoris and fused labia with the opening of the urethra at the base of the clitoris. 40
, musculinization of a female fetus ie. female intersexuality, precocious puberty in boys Female pseudohermaphrodite - premature pubic hair, hypertrophied clitoris and fused labia with the opening of the urethra at the base of the clitoris. 40.")
41
41 Any Questions ?

Similar presentations








 Glands Anatomy & Embryology>")









 Glands Anatomy & Embryology>")
 Glands Anatomy & Embryology Dr. Zeenat Zaidi & Dr. Essam Eldin Salama.>")
