Download presentation
Presentation is loading. Please wait.

1
Dawood Yusef, MD Assistant Professor Pediatric Infectious Disease, KAUH

2
Acute Otitis Media Tonsilitis Common Cold

3
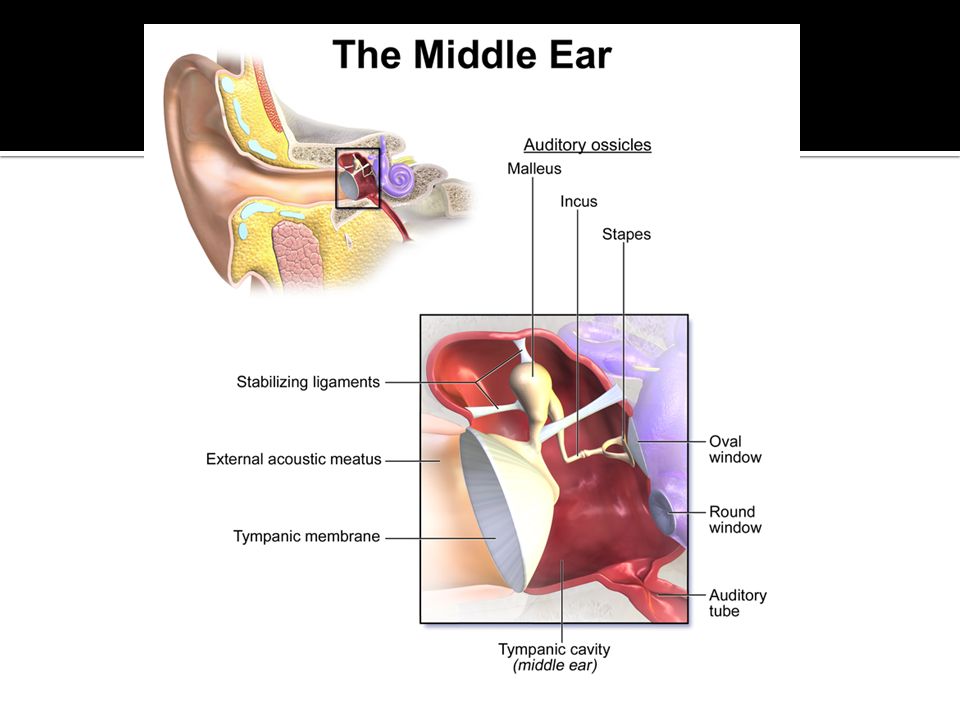
Acute otitis media (AOM): bulging of the tympanic membrane or new onset otorrhea with acute signs or symptoms of middle ear inflammation The most frequent diagnosis in sick children and most common reason for administration of antibiotics. Most prevalent in infancy: 90 % by two years.

5
Age: between 6 and 18 months of age Day care Lack of breastfeeding Tobacco smoke and air pollution Pacifier use

7
S. pneumoniae: greater severity and complications H. influenzae: often bilateral, associated with conjunctivitis. ½ produces b-lactamase M. catarrhalis: 10% of cases. 90% + betalactamase Viruses RSV, rhinovirus, enterovirus, coronavirus, influenza, adenovirus

8
Ear pain (otalgia) is the most common complaint Fever, irritability, vomiting, and diarrhea Otorrhea, hearing loss Vertigo, tinnitus, swelling of the ear, facial paralysis Otitis-conjunctivitis: Usually non-typeable H. flu

9
Clinical diagnosis Signs and symptoms of middle ear inflammation (bulging of the tympanic membrane, erythema of the tympanic membrane or otalgia, fever), and Middle ear effusion (eg, tympanic membrane opacity, decreased or absent tympanic membrane mobility, air-fluid level, or otorrhea)
, and Middle ear effusion (eg, tympanic membrane opacity, decreased or absent tympanic membrane mobility, air-fluid level, or otorrhea)")
10
Intratemporal complications (extracranial): Hearing loss (conductive, most common, or sensorineuronal) Balance and motor problems Tympanic membrane perforation, tympanosclerosis (asymptomatic whitish plaques) Cholesteatoma: abnormal growth of squamous epithelium in middle ear that may progressively enlarge to destroy ossicles Extension to adjacent structures (mastoiditis, labyrinthitis) Facial paralysis
: Hearing loss (conductive, most common, or sensorineuronal) Balance and motor problems Tympanic membrane perforation, tympanosclerosis (asymptomatic whitish plaques) Cholesteatoma: abnormal growth of squamous epithelium in middle ear that may progressively enlarge to destroy ossicles Extension to adjacent structures (mastoiditis, labyrinthitis) Facial paralysis")
11
Intracranial complications: Meningitis Epidural abscess Brain abscess Chronic suppurative otitis media (CSOM): perforation of the TM with chronic purulent drainage for more than 6 weeks
: perforation of the TM with chronic purulent drainage for more than 6 weeks")
13
SYMPTOMATIC THERAPY: Analgesics: Oral ibuprofen or acetaminophen Decongestants and antihistamines are not recommended The American Academy of Pediatrics recommends that over-the-counter cough and cold medications not be given to infants and children <4 years of age because of the risk of life-threatening side effects

14
First-line therapy: Amoxicillin Amoxicillin-clavulanate: children received a beta-lactam antibiotic in the past month or purulent conjunctivitis or treatment failure. For PCN allergy (type 1): Macrolides (eg, azithromycin, erythromycin) and lincosamides (eg, clindamycin) Duration: usually 10 days
: Macrolides (eg, azithromycin, erythromycin) and lincosamides (eg, clindamycin) Duration: usually 10 days.")
15
Streptococcus pyogenes (group A Streptococcus, GAS) is the most common cause of bacterial pharyngitis. Age usually between 5 and 15 years (school-age ) Abrupt onset of Fever, sore throat. Headache, abdominal pain, nausea, and vomiting may be present. Additional features: exudative pharyngitis, enlarged tender anterior cervical lymph nodes, palatal petechiae, and scarlatiniform rash.
 Abrupt onset of Fever, sore throat. Headache, abdominal pain, nausea, and vomiting may be present. Additional features: exudative pharyngitis, enlarged tender anterior cervical lymph nodes, palatal petechiae, and scarlatiniform rash..")
17
Viruses : The most common cause of acute pharyngitis Epstein-Barr (EBV), cytomegalovirus (CMV), adenovirus, herpes simplex (HSV), influenza and enterovirus. Clinical features: concurrent conjunctivitis, cough, hoarseness, anterior stomatitis, discrete ulcerative lesions, viral exanthems, and/or diarrhea

18
The major concern is to determine if group A Streptococcus (GAS) is the cause to: Prevention of suppurative complications and acute rheumatic fever Prevention of overuse use of antibiotics Reduction in duration and severity of symptoms Prevention of disease transmission Throat culture Rapid antigen detection test
 is the cause to: Prevention of suppurative complications and acute rheumatic fever Prevention of overuse use of antibiotics Reduction in duration and severity of symptoms Prevention of disease transmission Throat culture Rapid antigen detection test")
19
PCN or amino-PCN Resistance!? Allergy to PCN

20
Acute, self-limiting viral infection of the upper respiratory tract, involving, to variable degrees, sneezing, nasal congestion and discharge (rhinorrhea), sore throat, cough, low grade fever, headache, and malaise. The most frequent human illness. 30% of doctor visits result in a prescription for antibiotics Infants and children are affected more often and experience more prolonged symptoms than adults.

21
Rhinoviruses, include more than 100 serotypes, 50 % RSV, influenza, parainfluenza, adenoviruses, enteroviruses, coronaviruses

22
Occur any time of the year, high prevalence during fall and winter Transmission: Hand contact Droplets that are expelled during sneezing and land on nasal or conjunctival mucosa

23
Toys in a pediatric office waiting room contaminated with picornavirus RNA (rhinovirus or enterovirus). Viral shedding peaks on the third day. Incubation period 24 to 72 hours A change in nasal discharge from clear to yellow or green correlates with the increase in PMNs, but not with an increase in positive bacterial cultures

24
Children <6 years have an average of 6-8 colds per year with typical duration of 14 days. Young children in daycare appear to have more colds than children cared for at home. However, when they enter primary school, children who attended daycare are less vulnerable to colds than those who did not. Older children and adults have an average of two to four colds per year, with a typical symptom duration of five to seven days

25
Clinical, based upon history and examination findings, Including exposure. Management: mild and self-limiting illness. Anticipatory guidance and supportive care No antibiotics Cough and cold medications have no proven efficacy and potential for serious adverse effects No definitive evidence to indicate that treatment with zinc or vitamin C is beneficial in the treatment of the common cold in children.

26
Anticipatory guidance: Expected course peak on day two to three and improve over 10 to 14 days. In a minority of children the cough may linger, but should resolve over 4 weeks. Supportive interventions: adequate fluid intake; ingestion of warm liquids (eg, chicken soup, tea); suctioning the nose and upright positioning (for infants); saline nasal irrigation or sprays (for older children); and the use of cool mist humidifiers or vaporizers
; suctioning the nose and upright positioning (for infants); saline nasal irrigation or sprays (for older children); and the use of cool mist humidifiers or vaporizers.")
27
Over-the-counter medications Medications for the common cold in children younger than six years of age should not be used (FDA and AAP). Medications for the common cold in children 6 to 12 years is not recommended. OTC cough and cold medications have been associated with fatal overdose in children younger than two years

28
Cough: ● Lozenges or hard candy: no evidence of effectiveness. ● Honey: modest beneficial effect on nocturnal cough and is unlikely to be harmful in children older than one year of age

29
Hand hygiene frequent handwashing and avoiding touching mouth, nose, and eyes Disinfectants Immunizations Zinc Herbal products and vitamins

Similar presentations













>")
. >")
 is inflammation.>")






, which is an infection.>")