Download presentation
Presentation is loading. Please wait.

2
MENINGITIS By Dr Bashir Ahmed Dar By Dr Bashir Ahmed Dar Associate Professor Medicine Associate Professor Medicine Chinkipora Sopore Kashmir Chinkipora Sopore Kashmir Email- drbashir123@gmail.com Email- drbashir123@gmail.comdrbashir123@gmail.com

4
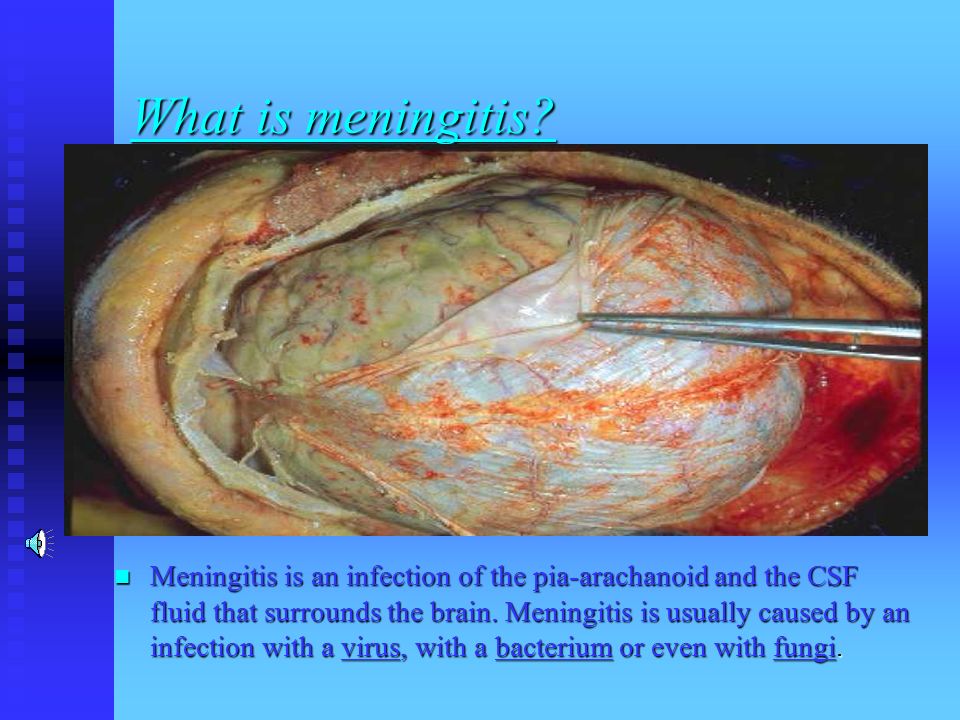
What is meningitis?. Meningitis is an infection of the pia-arachanoid and the CSF fluid that surrounds the brain. Meningitis is usually caused by an infection with a virus, with a bacterium or even with fungi.

5
How is Meningitis Caused Colonization of nasopharynx by bacteria or viruses Colonization of nasopharynx by bacteria or viruses Is an important way of spreading meningitis by way of cribriform fossa or viremia or bacteriaemia and can spread to others by coughing etc. Is an important way of spreading meningitis by way of cribriform fossa or viremia or bacteriaemia and can spread to others by coughing etc.

7
How is Meningitis Caused contagious, spread via tiny drops of fluid from the throat and nose of someone who is infected. The drops may become airborne when the person coughs, laughs, talks, or sneezes. They then can infect others when people breathe them in or touch the drops and then touch their own noses or mouths. contagious, spread via tiny drops of fluid from the throat and nose of someone who is infected. The drops may become airborne when the person coughs, laughs, talks, or sneezes. They then can infect others when people breathe them in or touch the drops and then touch their own noses or mouths.

8
How is Meningitis Caused Sharing food, drinking glasses, eating utensils, tissues, or towels. Sharing food, drinking glasses, eating utensils, tissues, or towels.

9
How is Meningitis Caused spread between people who are in close contact, such as those who live together or people who are exposed by kissing spread between people who are in close contact, such as those who live together or people who are exposed by kissing N. meningitidis cause epidemics of meningitis. In particular in a crowded day-care situation or a military recruit in a crowded training camp,schools,colleges has fallen ill with meningococcal meningitis N. meningitidis cause epidemics of meningitis. In particular in a crowded day-care situation or a military recruit in a crowded training camp,schools,colleges has fallen ill with meningococcal meningitis

10
How is Meningitis Caused Meningococcus is the bacteria that has caused outbreaks across North America over the last 8 - 10 years including most recently. Understandably the presence of a meningitis epidemic in a community is very scary to parents Meningococcus is the bacteria that has caused outbreaks across North America over the last 8 - 10 years including most recently. Understandably the presence of a meningitis epidemic in a community is very scary to parents

11
How is Meningitis Caused Most of the viruses that cause meningitis live in the intestines and tend to be passed on as a result of poor hygiene. Many different viruses can cause viral meningitis, most commonly enteroviruses that normally live harmlessly in people's bowels Most of the viruses that cause meningitis live in the intestines and tend to be passed on as a result of poor hygiene. Many different viruses can cause viral meningitis, most commonly enteroviruses that normally live harmlessly in people's bowels

12
How is Meningitis Caused L. monocytogenes has been associated with such foods as raw milk, pasteurized fluid milk,cheeses (particularly soft-ripened varieties), ice cream, raw vegetables, fermented raw-meat sausages, raw and cooked poultry, raw meats (of all types), and raw and smoked fish. Its ability to grow at temperatures as low as 0°C permits multiplication in refrigerated foods. In refrigeration temperature such as 4°C the amount of ferric iron promotes the growth of L. monocytogenes. L. monocytogenes has been associated with such foods as raw milk, pasteurized fluid milk,cheeses (particularly soft-ripened varieties), ice cream, raw vegetables, fermented raw-meat sausages, raw and cooked poultry, raw meats (of all types), and raw and smoked fish. Its ability to grow at temperatures as low as 0°C permits multiplication in refrigerated foods. In refrigeration temperature such as 4°C the amount of ferric iron promotes the growth of L. monocytogenes.
, ice cream, raw vegetables, fermented raw-meat sausages, raw and cooked poultry, raw meats (of all types), and raw and smoked fish. Its ability to grow at temperatures as low as 0°C permits multiplication in refrigerated foods. In refrigeration temperature such as 4°C the amount of ferric iron promotes the growth of L. monocytogenes. L. monocytogenes has been associated with such foods as raw milk, pasteurized fluid milk,cheeses (particularly soft-ripened varieties), ice cream, raw vegetables, fermented raw-meat sausages, raw and cooked poultry, raw meats (of all types), and raw and smoked fish. Its ability to grow at temperatures as low as 0°C permits multiplication in refrigerated foods. In refrigeration temperature such as 4°C the amount of ferric iron promotes the growth of L. monocytogenes..")
13
How is Meningitis Caused through a person's stool, and someone who comes in contact with the stool — such as a child in day care. through a person's stool, and someone who comes in contact with the stool — such as a child in day care.

14
How is Meningitis Caused Hematogenous Hematogenous Many of the bacteria and viruses that cause meningitis are fairly common and are typically associated with other routine illnesses. Many of the bacteria and viruses that cause meningitis are fairly common and are typically associated with other routine illnesses. infection of the skin, urinary system, gastrointestinal or respiratory tract can spread by the bloodstream infection of the skin, urinary system, gastrointestinal or respiratory tract can spread by the bloodstream

15
How is Meningitis Caused A person may have another type of infection (of the lungs, throat, or tissues of the heart) caused by an organism that can also cause meningitis A person may have another type of infection (of the lungs, throat, or tissues of the heart) caused by an organism that can also cause meningitis
 caused by an organism that can also cause meningitis A person may have another type of infection (of the lungs, throat, or tissues of the heart) caused by an organism that can also cause meningitis")
16
How is Meningitis Caused Direct infection Direct infection skull fractures possess abnormal openings to the sinuses, nasal passages, and middle ears. Organisms can pass through openings and cause infection. surgical procedures or who have had foreign bodies surgically placed within their skulls (such as tubes to drain abnormal amounts of accumulated CSF) have an increased risk of meningitis. skull fractures possess abnormal openings to the sinuses, nasal passages, and middle ears. Organisms can pass through openings and cause infection. surgical procedures or who have had foreign bodies surgically placed within their skulls (such as tubes to drain abnormal amounts of accumulated CSF) have an increased risk of meningitis.
 have an increased risk of meningitis. skull fractures possess abnormal openings to the sinuses, nasal passages, and middle ears. Organisms can pass through openings and cause infection. surgical procedures or who have had foreign bodies surgically placed within their skulls (such as tubes to drain abnormal amounts of accumulated CSF) have an increased risk of meningitis..")
17
How is Meningitis Caused otitis media otitis media mastoiditis mastoiditis Osteomyelitic foci in the skull Osteomyelitic foci in the skull sinusitis sinusitis Penetrating cranial injuries Penetrating cranial injuries Brain or spine surgery Brain or spine surgery Ventriculoperitoneal shun Ventriculoperitoneal shun lumbar puncture. lumbar puncture.

18
How is Meningitis Caused skull fractures skull fractures Extradural abscess Extradural abscess Subdural empyaema Subdural empyaema Spinal epidural abscess. Spinal epidural abscess. Pachymeningitis Pachymeningitis

19
How is Meningitis Caused Neurotropic Neurotropic also via an uncommon but interesting method called intraneural spread. This involves an organism invading the body at a considerable distance away from the head, spreading along a nerve, and using that nerve as a kind of ladder into the skull, where the organism can multiply and cause meningitis. Herpes simplex virus is known to use this type of spread, as is the rabies virus. also via an uncommon but interesting method called intraneural spread. This involves an organism invading the body at a considerable distance away from the head, spreading along a nerve, and using that nerve as a kind of ladder into the skull, where the organism can multiply and cause meningitis. Herpes simplex virus is known to use this type of spread, as is the rabies virus. Rabies Rabies HSV HSV

20
How is Meningitis Caused RISKS RISKS Asplenia Asplenia drugs that suppress immune system drugs that suppress immune system Immunocompromised Immunocompromised HIV, malignancy HIV, malignancy malignancy malignancy alcholism alcholism

21
How is Meningitis Caused Patients with cardiac and pulmonary anomalies may spread septic foci,bronchiectasis, occasionally pneumonia). Common with pulmonary AV fistulae and R to L cardiac defect Patients with cardiac and pulmonary anomalies may spread septic foci,bronchiectasis, occasionally pneumonia). Common with pulmonary AV fistulae and R to L cardiac defect T-cell defects (HIV) T-cell defects (HIV) Neural tube defects- Staph aureus, enteric organisms Neural tube defects- Staph aureus, enteric organisms Terminal compliment deficiency- Neisseria Terminal compliment deficiency- Neisseria septic foci from thrombophibitis septic foci from thrombophibitis iv drug abusers iv drug abusers
. Common with pulmonary AV fistulae and R to L cardiac defect T-cell defects (HIV) T-cell defects (HIV) Neural tube defects- Staph aureus, enteric organisms Neural tube defects- Staph aureus, enteric organisms Terminal compliment deficiency- Neisseria Terminal compliment deficiency- Neisseria septic foci from thrombophibitis septic foci from thrombophibitis iv drug abusers iv drug abusers.")
22
How is Meningitis Caused Immune-compromised Patients are also prone for fungal infections and the fungal infections that can result in meningitis are Immune-compromised Patients are also prone for fungal infections and the fungal infections that can result in meningitis are Aspergillus Aspergillus Candida Candida Mucor Mucor Protozoal,Ameba infections,Toxoplasma Protozoal,Ameba infections,Toxoplasma

23
Organisms Causing Meningitis Bacterial Bacterial Viral Viral Fungal Fungal Ricketsial Ricketsial Parasitic/Protozoal Parasitic/Protozoal

24
Organisms Causing Meningitis Purulent bacterial meningitis Purulent bacterial meningitis etiology etiology newborns Group B Strep,E. coli newborns Group B Strep,E. coli children - H. influenzae, Str. pneumoniae children - H. influenzae, Str. pneumoniae HIB vaccine has reduced incidence of H influnza infection HIB vaccine has reduced incidence of H influnza infection adults - meningococccal (small epidemies - army, holiday camps,school going students),pneumococcal adults - meningococccal (small epidemies - army, holiday camps,school going students),pneumococcal
,pneumococcal adults - meningococccal (small epidemies - army, holiday camps,school going students),pneumococcal.")
25
Organisms Causing Meningitis Streptococcus agalactiae (also known as Group B streptococcus) is a beta-hemolytic gram-positive streptococcus. Streptococcus agalactiae (also known as Group B streptococcus) is a beta-hemolytic gram-positive streptococcus. S. agalactiae is a species of the normal flora of the female urogenital tract and rectum. Its chief clinical importance is that it can be transferred to a neonate passing through the birth canal and can cause serious group B streptococcal infection. S. agalactiae is a species of the normal flora of the female urogenital tract and rectum. Its chief clinical importance is that it can be transferred to a neonate passing through the birth canal and can cause serious group B streptococcal infection.
 is a beta-hemolytic gram-positive streptococcus. S. agalactiae is a species of the normal flora of the female urogenital tract and rectum. Its chief clinical importance is that it can be transferred to a neonate passing through the birth canal and can cause serious group B streptococcal infection. S. agalactiae is a species of the normal flora of the female urogenital tract and rectum. Its chief clinical importance is that it can be transferred to a neonate passing through the birth canal and can cause serious group B streptococcal infection..")
26
Organisms Causing Meningitis In the western world, S. agalactiae is a major cause of bacterial septicemia of the newborn, which can lead to death or long- term sequelae such as hearing loss. S. agalactiae can also cause neonatal meningitis, which does not present with the hallmark sign of adult meningitis, a stiff neck In the western world, S. agalactiae is a major cause of bacterial septicemia of the newborn, which can lead to death or long- term sequelae such as hearing loss. S. agalactiae can also cause neonatal meningitis, which does not present with the hallmark sign of adult meningitis, a stiff neck

27
Organisms Causing Meningitis rather, it presents with nonspecific symptoms such as fever, vomiting and irritability and can consequently go undiagnosed until it is too late. Somewhat more rarely, S. agalactiae can also cause invasive group B streptococcal disease of the adult in the pregnant, elderly, or immunosuppressed. rather, it presents with nonspecific symptoms such as fever, vomiting and irritability and can consequently go undiagnosed until it is too late. Somewhat more rarely, S. agalactiae can also cause invasive group B streptococcal disease of the adult in the pregnant, elderly, or immunosuppressed.

28
Organisms Causing Meningitis Viral Viral HSV especially in infants Enterovirus (coxsackie, echovirus) HIV Lymphocytic choriomeningitis virus Arbovirus Mumps CMV EBV VZV Adenovirus Measles
 HIV Lymphocytic choriomeningitis virus Arbovirus Mumps CMV EBV VZV Adenovirus Measles")
29
Organisms Causing Meningitis Rubella Rotavirus Influenza and parainfluenza

30
Organisms Causing Meningitis Fungal Fungal Cryptococcus Coccidiodes Histoplasmosis Mucormycosis Aspergilosis Candidasis With a particular prone settings etc

31
Organisms Causing Meningitis Parasitic/protozoal Parasitic/protozoal Angiostrongylus Toxoplamosis Hydatid Amoeba Malaria Cysticercosis

32
Organisms Causing Meningitis Rickettsial Rickettsial Rocky mountain spotted fever Rocky mountain spotted fever

33
Organisms Causing Meningitis Others Others Tuberculosis Tuberculosis Borrelia burgdorferi Treponema pallidum Mycoplasma pneumoniae brucella Chlamydia

34
Organisms Causing Meningitis viral meningitis viral meningitis fairly common disease but rarely fatal fairly common disease but rarely fatal lymphocytic predominance ie mononuclear cells (but may see neutrophils if CSF sampled early in course - up to 48hrs lymphocytic predominance ie mononuclear cells (but may see neutrophils if CSF sampled early in course - up to 48hrs glucose not reduced glucose not reduced

35
Organisms Causing Meningitis may follow Temporary, flu-like symptoms with running nose sneezing etc., headache, low grade fever and stiff neck. may follow Temporary, flu-like symptoms with running nose sneezing etc., headache, low grade fever and stiff neck. Goes away on its own usually within three to 10 days Goes away on its own usually within three to 10 days Bed rest, paracetamol Bed rest, paracetamol Enteroviruses, the most common type of viral meningitis Enteroviruses, the most common type of viral meningitis Strict isolation is not necessary Strict isolation is not necessary

36
Organisms Causing Meningitis Since most cases are due to enteroviruses that may be passed in the stool, people diagnosed with viral meningitis should be instructed to thoroughly wash their hands after using the toilet. Since most cases are due to enteroviruses that may be passed in the stool, people diagnosed with viral meningitis should be instructed to thoroughly wash their hands after using the toilet.

37
Organisms Causing Meningitis The incidence of viral meningitis drops with age. The incidence of viral meningitis drops with age. Neonates are at greatest risk and have the most significant risk of morbidity and mortality. Neonates are at greatest risk and have the most significant risk of morbidity and mortality. The incidence during the first year of life is 20 times higher than in older children and adults. The incidence during the first year of life is 20 times higher than in older children and adults.

38
Organisms Causing Meningitis CRP much more elevated in bacterial than in viral meningitis (ie, 50-150 in bacterial meningitis group vs <20 in viral meningitis group). CRP much more elevated in bacterial than in viral meningitis (ie, 50-150 in bacterial meningitis group vs <20 in viral meningitis group). Treatment for viral meningitis is mostly supportive. Treatment for viral meningitis is mostly supportive.
. Treatment for viral meningitis is mostly supportive. Treatment for viral meningitis is mostly supportive..")
39
Neisseria meningitidis

40
Hemophilus influenza (H flu) Strep pneumoniae
 Strep pneumoniae")
41
CSF-Gram stain: Low power view showing many neutrophi ls. Low power view showing many neutrophi ls.

42
CSF-Gram stain: High power shows clusters of bacteria. High power shows clusters of bacteria. Neutrophil s Neutrophil s

43
CSF-Gram stain: High power shows clusters of bacteria. High power shows clusters of bacteria. Neutrophil Neutrophil

44
CSF-Gram stain: High power shows clusters of bacteria. High power shows clusters of bacteria. Neutrophil Neutrophil

45
CSF-Gram stain: Observe Paired rounded bacteria – (diplococci) staining pink (gram negative)
 staining pink (gram negative)")
46
Pathogenesis of Meningitis The virus or bacteria replicates in the initial organ system (ie, respiratory or gastrointestinal mucosa) and gains access to the bloodstream. Primary viremia or bacteremia introduces the virus or bacteria to the reticuloendothelial organs (liver, spleen, and lymph nodes.) The virus or bacteria replicates in the initial organ system (ie, respiratory or gastrointestinal mucosa) and gains access to the bloodstream. Primary viremia or bacteremia introduces the virus or bacteria to the reticuloendothelial organs (liver, spleen, and lymph nodes.)
 The virus or bacteria replicates in the initial organ system (ie, respiratory or gastrointestinal mucosa) and gains access to the bloodstream. Primary viremia or bacteremia introduces the virus or bacteria to the reticuloendothelial organs (liver, spleen, and lymph nodes.).")
47
Pathogenesis of Meningitis If the replication persists despite immunologic defenses, secondary bacteremia or viremia occurs, which is thought to be responsible for seeding of the CNS. Rapid viral replication likely plays a major role in overcoming the host defenses. If the replication persists despite immunologic defenses, secondary bacteremia or viremia occurs, which is thought to be responsible for seeding of the CNS. Rapid viral replication likely plays a major role in overcoming the host defenses.

48
Pathogenesis of Meningitis There occurs local immune response to bacteria or virus There occurs local immune response to bacteria or virus Increased vascular permeability Increased vascular permeability oozing of fluid exudate,inflammatory cells oozing of fluid exudate,inflammatory cells Neutrophils migrate from capillaries and release toxins Neutrophils migrate from capillaries and release toxins TNF-a and IL-B1 produced by activated macrophages and endothelial cells TNF-a and IL-B1 produced by activated macrophages and endothelial cells

49
Pathogenesis of Meningitis Ensuing inflammatory response increases blood-brain permeability Ensuing inflammatory response increases blood-brain permeability Cerebral edema Cerebral edema Increased ICP Increased ICP

50
Pathogenesis of Meningitis cellular damage and loss of cellular homeostasis and worsen cerebral edema cellular damage and loss of cellular homeostasis and worsen cerebral edema damage to vessels lead to vasculitis and bleed or thrombose leading to infaraction or haemorrahage damage to vessels lead to vasculitis and bleed or thrombose leading to infaraction or haemorrahage exudate formation etc can obstruct CSF flow and lead to hydrocephalous exudate formation etc can obstruct CSF flow and lead to hydrocephalous ICP lead to herniation ICP lead to herniation

51
Pathogenesis of Meningitis exudative pus of dead cells,fluid,fibrin and leucocytes (pus) cause thick whitish grey layer that covers the leptomeninges over the surface of brain and filling sulci and basal cisterns with swollen edematous brain. exudative pus of dead cells,fluid,fibrin and leucocytes (pus) cause thick whitish grey layer that covers the leptomeninges over the surface of brain and filling sulci and basal cisterns with swollen edematous brain. damage to neurons can take place if extending to brain cells resulting in their degeneration. damage to neurons can take place if extending to brain cells resulting in their degeneration.
 cause thick whitish grey layer that covers the leptomeninges over the surface of brain and filling sulci and basal cisterns with swollen edematous brain. damage to neurons can take place if extending to brain cells resulting in their degeneration. damage to neurons can take place if extending to brain cells resulting in their degeneration..")
52
The white appearance of this calf brain is caused by neutrophils within the meninges – a condition known as meningitis. This is usually due to a bacterial infection.

53
This calf brain shows similar pathology. If a glass slide is pressed to the surface of the brain and stained it would show high numbers of neutrophils.

54
Bovine This brain shows irregular red spots which are areas of hemorrhage and necrosis caused by the bacteria, Histophilus somni.

55
Brain: meningitis.

56
Pathogenesis of Meningitis if infection becomes localised in brain then can lead to abcess formation especially in case of direct infections. if infection becomes localised in brain then can lead to abcess formation especially in case of direct infections. immune system tries to confine this localised infection therefore may develop fibrous wall around it with perivascular chronic inflamatory cells around it,leading to brain abcess with central suppuration and liqufication due to death of cells.healing may occur with fibrous scar. immune system tries to confine this localised infection therefore may develop fibrous wall around it with perivascular chronic inflamatory cells around it,leading to brain abcess with central suppuration and liqufication due to death of cells.healing may occur with fibrous scar.

57
The Evolution of the Abscess is as follows An area of cerebritis begins, in which Polymorphonuclear leukocytes are attracted to the invading bacteria. An area of cerebritis begins, in which Polymorphonuclear leukocytes are attracted to the invading bacteria. Liquefaction of brain tissue rapidly ensues, and at the periphery, a thin rim of granulation tissue composed of new capillaries and fibroblasts is formed. Liquefaction of brain tissue rapidly ensues, and at the periphery, a thin rim of granulation tissue composed of new capillaries and fibroblasts is formed.

58
Evolution of the Abscess With time, a connective tissue capsule is formed by collagen laid down by infiltrating fibroblasts. Often this is more perfectly formed on the outer aspect of the abscess, presumably due to the contribution of the reservoir of potential in the adjacent meninges. With time, a connective tissue capsule is formed by collagen laid down by infiltrating fibroblasts. Often this is more perfectly formed on the outer aspect of the abscess, presumably due to the contribution of the reservoir of potential in the adjacent meninges.

59
Evolution of the Abscess Due to the poor encapsulation of the medial aspect of an abscess, which abuts upon or is located within the cerebral white matter, the infection tends to form daughter or satellite abscesses medially which may eventually rupture into the ventricular system Due to the poor encapsulation of the medial aspect of an abscess, which abuts upon or is located within the cerebral white matter, the infection tends to form daughter or satellite abscesses medially which may eventually rupture into the ventricular system

60
Evolution of the Abscess Such rupture may lead to rapid death, and in any event, is usually followed by severe ventriculitis and massive meningitis as infected CSF pours into the subarachnoid space. Such rupture may lead to rapid death, and in any event, is usually followed by severe ventriculitis and massive meningitis as infected CSF pours into the subarachnoid space. Antibiotic therapy greatly decelerates the growth of an abscess, and may allow time for a complete capsule to form after which the abscess may be removed surgically. Antibiotic therapy greatly decelerates the growth of an abscess, and may allow time for a complete capsule to form after which the abscess may be removed surgically.

61
Evolution of the Abscess

62
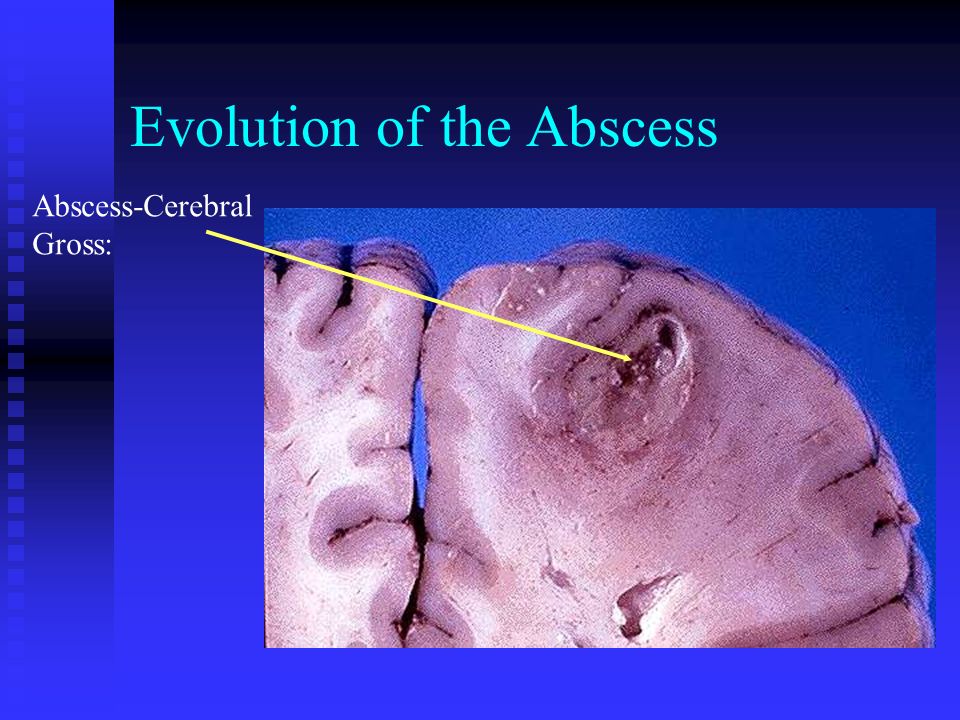
The image above shows a large abscess in the brain. The purulent center is surrounded by a capsule. Often a zone of hyperemia is present adjacent to the wall and there is marked swelling of the adjacent brain tissue The image above shows a large abscess in the brain. The purulent center is surrounded by a capsule. Often a zone of hyperemia is present adjacent to the wall and there is marked swelling of the adjacent brain tissue

63
Evolution of the Abscess

65
Abscess-Cerebral Gross:

66
Abscess-Cerebral MRI

68
Meningial enhancement Meningial enhancement in a Bacterial meningitis - CT Scan Image

69
Meningial enhancement

70
Signs & symptoms of Meningitis Acute (<1 day)- common with S. pneumoniae and N. meningitides Subacute (2-3 days)- preceding URI like symptoms, more common with H. flu and other pathogens.
- preceding URI like symptoms, more common with H. flu and other pathogens..")
71
Signs & symptoms of Meningitis Non-specific complaints Non-specific complaints Fever Headache Nausea and vomiting --Nuchal rigidity --Nuchal rigidity Lethargy Irritability Restlessness Poor feeding Back pain Altered mental status (seizure, coma)
")
73
Signs & symptoms of Meningitis Febrile stiff neck causing may causearched position Opisthotonos Focal neurologic signs Petechia/purpura- DIC with N. menigitidis Positive Kernig’s and Brudniski’s i.e., Meningismus (stiff neck + Brudzinski + Kernig signs) Shock Shock Disseminated intravascular coagulation (DIC) Disseminated intravascular coagulation (DIC) Cerebral edema Cerebral edema
 Shock Shock Disseminated intravascular coagulation (DIC) Disseminated intravascular coagulation (DIC) Cerebral edema Cerebral edema.")
74
Kernig’s Sign Patient placed supine with hips flexed 90 degrees. Examiner attempts to extend the leg at the knee Patient placed supine with hips flexed 90 degrees. Examiner attempts to extend the leg at the knee Positive test elicited when there is resistance to knee extension, or pain in the lower back or thigh with knee extension Positive test elicited when there is resistance to knee extension, or pain in the lower back or thigh with knee extension

75
Signs & symptoms of Meningitis

76
Brudzinski’s Sign Patient placed in supine position and neck is passively flexed towards the chest Patient placed in supine position and neck is passively flexed towards the chest Positive test is elicited when flexion of neck causes flexion at knees and/or hips of the patient Positive test is elicited when flexion of neck causes flexion at knees and/or hips of the patient

78
Normal fundus

79
Increased intracranial pressure (ICP) Papilledema Cushing’s triad Bradycardia Hypertension Irregular respiration Severe headache herniation vomitting ICP monitor (not routine) Changes in pupils
 Papilledema Cushing’s triad Bradycardia Hypertension Irregular respiration Severe headache herniation vomitting ICP monitor (not routine) Changes in pupils")
80
Meningococcemia - Petechiae

81
Signs & symptoms of Meningitis Is due to small skin bleed Is due to small skin bleed All parts of the body are affeced All parts of the body are affeced The rashes do not fade under pressure The rashes do not fade under pressure Pathogenesis: Pathogenesis: a. Septicemia a. Septicemia b. wide spread endothelial damage b. wide spread endothelial damage c. activation of coagulation c. activation of coagulation d. thrombosis and platelets aggregation d. thrombosis and platelets aggregation

82
Signs & symptoms of Meningitis e. reduction of platelets (cosumption ) e. reduction of platelets (cosumption ) f. BLEEDING 1.skin rashes f. BLEEDING 1.skin rashes 2.adrenal hemorrhage 2.adrenal hemorrhage Arenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal Arenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal
 f. BLEEDING 1.skin rashes f. BLEEDING 1.skin rashes 2.adrenal hemorrhage 2.adrenal hemorrhage Arenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal Arenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal.")
83
Meningococcemia - Purpura fulminans

84
Signs & symptoms of Meningitis May also look like bruises,echymosis. May also look like bruises,echymosis.

85
Complications and Outcome of Meningitis Infection can spreading to Infection can spreading to Dura – pachymeningitis Dura – pachymeningitis Leptomeninges - leptomeningitis Leptomeninges - leptomeningitis Brain – encephalitis Brain – encephalitis Spinal cord – myelitis Spinal cord – myelitis Ventricles - ventriculitis Ventricles - ventriculitis

86
Complications and Outcome of Meningitis Disseminated intravascular coagulation (DIC) Cerebral edema Disseminated intravascular coagulation (DIC) Cerebral edema Adrenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal Adrenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal septicaemia and infection spreading to other organs septicaemia and infection spreading to other organs motor and neurological deficits motor and neurological deficits
 Cerebral edema Disseminated intravascular coagulation (DIC) Cerebral edema Adrenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal Adrenal hemorrhage is called Waterhouse- Friderichsen Syndrome.It cause acute adrenal insufficiency and is uaually fatal septicaemia and infection spreading to other organs septicaemia and infection spreading to other organs motor and neurological deficits motor and neurological deficits")
87
Complications and Outcome of Meningitis Seizures Seizures SIADH SIADH Subdural effusions & empyema Subdural effusions & empyema Septic sinus or cortical vein thrombosis Septic sinus or cortical vein thrombosis Arterial ischemia / infarction (inflammatory vasculitis) Arterial ischemia / infarction (inflammatory vasculitis) CNs Palsies (esp deafness) CNs Palsies (esp deafness) Septic shock / multi-organ failure from bacteremia (esp meningococcus & pneumococcus) Septic shock / multi-organ failure from bacteremia (esp meningococcus & pneumococcus)
 Arterial ischemia / infarction (inflammatory vasculitis) CNs Palsies (esp deafness) CNs Palsies (esp deafness) Septic shock / multi-organ failure from bacteremia (esp meningococcus & pneumococcus) Septic shock / multi-organ failure from bacteremia (esp meningococcus & pneumococcus)")
88
Complications and Outcome of Meningitis risk of adrenal hemorrhage with hypo- adrenalism (Waterhouse-Friderichsen syndrome) risk of adrenal hemorrhage with hypo- adrenalism (Waterhouse-Friderichsen syndrome) Serum sodium level may be abnormal because of dehydration or the rare occurrence of syndrome of inappropriate antidiuretic hormone secretion (SIADH). Serum sodium level may be abnormal because of dehydration or the rare occurrence of syndrome of inappropriate antidiuretic hormone secretion (SIADH).
..")
89
Complications and Outcome of Meningitis Serum amylase level may be elevated in cases caused by mumps even in the absence of parotitis. Serum amylase level may be elevated in cases caused by mumps even in the absence of parotitis. Focal infarctions/microinfarcts due to endarteritis oblitrerans Focal infarctions/microinfarcts due to endarteritis oblitrerans Formation of intracranial mass Formation of intracranial mass Cranial nerve palsies Cranial nerve palsies

90
Increased intracranial pressure HeadacheVomiting Decreased Level of Consciousness PapilledemaHerniation

91
TYPES OF HERNIATION 1. Subfalcine (cingulate) 2. Transtentorial (uncal) 3. Tonsillar (foramen magnum) 4. Extracranial
 4. Extracranial.")
92
TRANSTENTORIAL (UNCAL) HERNIATION SHIFT OF THE BRAIN FROM THE MIDDLE TO THE POSTERIOR FOSSA THROUGH THE TENTORIAL INCISURA MAY BE UNILATERAL OR “CENTRAL” SECONDARY EFFECTS INCLUDE: Compression of the third cranial nerve(s) Duret hemorrhages in midline rostral brainstem Compression of the contralateral cerebral peduncle (Kernohan’s notch) Compression of the posterior cerebral artery with infarction of the medial occipital lobe
 HERNIATION SHIFT OF THE BRAIN FROM THE MIDDLE TO THE POSTERIOR FOSSA THROUGH THE TENTORIAL INCISURA MAY BE UNILATERAL OR CENTRAL SECONDARY EFFECTS INCLUDE: Compression of the third cranial nerve(s) Duret hemorrhages in midline rostral brainstem Compression of the contralateral cerebral peduncle (Kernohan’s notch) Compression of the posterior cerebral artery with infarction of the medial occipital lobe")
93
HYDROCEPHALUS DILATATION OF THE VENTRICULAR SYSTEM NONCOMMUNICATING: Due to obstruction within the ventricular system, e.g., tumor, aqueductal stenosis COMMUNICATING: Due to obstruction of CSF flow in the subarachnoid space with decreased reabsorption

94
Complications and Outcome of Meningitis Consequences of meningitis can be mild, moderate or severe, Consequences of meningitis can be mild, moderate or severe, with many survivors being left with permanent disability with many survivors being left with permanent disability Septicaemia and shock can lead to skin grafting Septicaemia and shock can lead to skin grafting and scarring, amputations and in severe cases neurological deficits and scarring, amputations and in severe cases neurological deficits Meningitis can lead to damage in various areas of the brain resulting in loss of sight, hearing and neurodevelopmental deficits Meningitis can lead to damage in various areas of the brain resulting in loss of sight, hearing and neurodevelopmental deficits

95
Complications and Outcome of Meningitis Scarring Scarring amputation of digits and limbs amputation of digits and limbs Neurological damage Neurological damage

96
Complications and Outcome of Meningitis Visual impairment and blindness Visual impairment and blindness Auditory impairment and deafness Auditory impairment and deafness Neuromotor disabilities Neuromotor disabilities Seizure disorders Seizure disorders Behaviour problems Behaviour problems Learning difficulties Learning difficulties

97
Complications and Outcome of Meningitis The complications associated with septic shock can result in irreversible tissue damage and gangrene The complications associated with septic shock can result in irreversible tissue damage and gangrene Tissue damage occurs as a result of inadequate tissue perfusion and oxygenation from hypotension and coagulopathy Tissue damage occurs as a result of inadequate tissue perfusion and oxygenation from hypotension and coagulopathy Skin grafting and amputation may be necessary Skin grafting and amputation may be necessary

98
Complications and Outcome of Meningitis Damage to various areas of the brain as a consequence of inflammation in the subarachnoid space Damage to various areas of the brain as a consequence of inflammation in the subarachnoid space This appears as exudate covering the surface of the brain This appears as exudate covering the surface of the brain Many complications are due to cranial nerve damage Many complications are due to cranial nerve damage

99
Complications and Outcome of Meningitis Psychosocial and emotional problems - low self esteem and difficulties coping Psychosocial and emotional problems - low self esteem and difficulties coping Subtle complications - poor concentration, clumsiness and mood swings Subtle complications - poor concentration, clumsiness and mood swings May be age-specific May be age-specific

100
Complications and Outcome of Meningitis Tiredness Tiredness Recurring headaches Recurring headaches Memory loss, which may be severe Memory loss, which may be severe Difficulties in concentration Difficulties in concentration Anger outbursts Anger outbursts Clumsiness Clumsiness

101
Differential Diagnosis of Meningitis Brain abscess Brain abscess Encephalitis Encephalitis Tumor like ASTROCYTOMAS,OLIGODENDROGLIOMAS,EPENDYMOMAS Tumor like ASTROCYTOMAS,OLIGODENDROGLIOMAS,EPENDYMOMAS MIXED GLIOMAS MIXED GLIOMAS Metastatic tumor Metastatic tumor Subdural and epidural empyema Subdural and epidural empyema subdural subdural subarachnoid subarachnoid

102
Differential Diagnosis of Meningitis Chemical meningitis: Rupture of tumor Chemical meningitis: Rupture of tumor intracranial haemorrage like intracranial haemorrage like Epidural Epidural subdural subdural Subarachnoid Subarachnoid intraparenchymal intraparenchymal

103
Differential Diagnosis of Meningitis metabolic encephalopathy metabolic encephalopathy hyperglycaemic coma hyperglycaemic coma uremia uremia hepatic encephalopathy hepatic encephalopathy vit B deficiencies vit B deficiencies vascular diseases (amyloid angiopathy, vasculitis, berry aneurysms, A-V malformations vascular diseases (amyloid angiopathy, vasculitis, berry aneurysms, A-V malformations

104
CSF & LUMBER PUNCTURE It is produced in the brain by modified ependymal cells in the choroid plexus (approx. 50-70%), and the remainder is formed around blood vessels and along ventricular walls. It circulates from the choroid plexus through the interventricular foramina (foramen of Monro) into the third ventricle, and then through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle, where it exits through two lateral apertures (foramina of Luschka) and one median aperture (foramen of Magendie). It is produced in the brain by modified ependymal cells in the choroid plexus (approx. 50-70%), and the remainder is formed around blood vessels and along ventricular walls. It circulates from the choroid plexus through the interventricular foramina (foramen of Monro) into the third ventricle, and then through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle, where it exits through two lateral apertures (foramina of Luschka) and one median aperture (foramen of Magendie).
, and the remainder is formed around blood vessels and along ventricular walls. It circulates from the choroid plexus through the interventricular foramina (foramen of Monro) into the third ventricle, and then through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle, where it exits through two lateral apertures (foramina of Luschka) and one median aperture (foramen of Magendie). It is produced in the brain by modified ependymal cells in the choroid plexus (approx %), and the remainder is formed around blood vessels and along ventricular walls. It circulates from the choroid plexus through the interventricular foramina (foramen of Monro) into the third ventricle, and then through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle, where it exits through two lateral apertures (foramina of Luschka) and one median aperture (foramen of Magendie)..")
105
CSF & LUMBER PUNCTURE It then flows through the cerebellomedullary cistern down the spinal cord and over the cerebral hemispheres. It then flows through the cerebellomedullary cistern down the spinal cord and over the cerebral hemispheres.

106
CSF & LUMBER PUNCTURE The cerebrospinal fluid is produced at a rate of 500 ml/day. Since the brain can only contain from 135-150 ml, large amounts are drained primarily into the blood through arachnoid granulations in the superior sagittal sinus. Thus the CSF turns over about 3.7 times a day. The cerebrospinal fluid is produced at a rate of 500 ml/day. Since the brain can only contain from 135-150 ml, large amounts are drained primarily into the blood through arachnoid granulations in the superior sagittal sinus. Thus the CSF turns over about 3.7 times a day.

107
CSF & LUMBER PUNCTURE Direct cranial measurement of ICP. Direct cranial measurement of ICP. ICP monitoring requires admission to the hospital. A small pressure monitor is inserted through the skull into the brain or ventricles to measure the ICP. pressure monitoring (either by lumbar catheter or the intracranial method) can detect an abnormal pattern of pressure waves. ICP monitoring requires admission to the hospital. A small pressure monitor is inserted through the skull into the brain or ventricles to measure the ICP. pressure monitoring (either by lumbar catheter or the intracranial method) can detect an abnormal pattern of pressure waves.
 can detect an abnormal pattern of pressure waves. ICP monitoring requires admission to the hospital. A small pressure monitor is inserted through the skull into the brain or ventricles to measure the ICP. pressure monitoring (either by lumbar catheter or the intracranial method) can detect an abnormal pattern of pressure waves..")
108
CSF & LUMBER PUNCTURE Ventricular puncture for the relief of increased ICP is one of the oldest practices in neurosurgery. Ventricular puncture for the relief of increased ICP is one of the oldest practices in neurosurgery.

109
CSF & LUMBER PUNCTURE The "gold standard" technique for ICP monitoring is a catheter inserted into the lateral ventricle, usually via a small right frontal burr hole. This can be connected to a standard pressure transducer via a fluid- filled catheter in neurosurgery. The "gold standard" technique for ICP monitoring is a catheter inserted into the lateral ventricle, usually via a small right frontal burr hole. This can be connected to a standard pressure transducer via a fluid- filled catheter in neurosurgery.

110
CSF & LUMBER PUNCTURE Indirect measurement of ICP by lumber puncture. Indirect measurement of ICP by lumber puncture. The two principal objections to lumbar puncture in the diagnosis of intracranial hypertension have been the danger of inducing brain-stem compression through tentorial or tonsillar herniation and the contention that spinal fluid pressure is not always an accurate reflection of ICP. The two principal objections to lumbar puncture in the diagnosis of intracranial hypertension have been the danger of inducing brain-stem compression through tentorial or tonsillar herniation and the contention that spinal fluid pressure is not always an accurate reflection of ICP.

111
CSF & LUMBER PUNCTURE Indications Indications 1. Diagnostic aid 1. Diagnostic aid 2. Therapy for idiopathic intracranial hypertension 2. Therapy for idiopathic intracranial hypertension 3. Infusion of anaesthetic (“spinal”), chemotherapy, or contrast agents (myelography) 3. Infusion of anaesthetic (“spinal”), chemotherapy, or contrast agents (myelography)
, chemotherapy, or contrast agents (myelography) 3. Infusion of anaesthetic ( spinal ), chemotherapy, or contrast agents (myelography).")
112
CSF & LUMBER PUNCTURE Contraindications Contraindications - INR > 1.4 or other coagulopathy - INR > 1.4 or other coagulopathy - platelets < 50 - platelets < 50 - infection at desired puncture site - infection at desired puncture site - obstructive / non-communicating hydrocephalus - obstructive / non-communicating hydrocephalus - intracranial mass - intracranial mass - high intracranial pressure (ICP) / papilloedema - high intracranial pressure (ICP) / papilloedema
 / papilloedema - high intracranial pressure (ICP) / papilloedema")
113
CSF & LUMBER PUNCTURE An LP may safely be performed without first doing a CT head in a young previously healthy patient with no history of seizures, a normal level of consciousness and a normal neurological exam. An LP may safely be performed without first doing a CT head in a young previously healthy patient with no history of seizures, a normal level of consciousness and a normal neurological exam.

114
CSF & LUMBER PUNCTURE Anatomy Anatomy Intercristal line is an imaginary line that connects the superior border of the iliac crests Intercristal line is an imaginary line that connects the superior border of the iliac crests - L4/5 interspace is the first interspace caudal to the intercristal line - L4/5 interspace is the first interspace caudal to the intercristal line

115
CSF & LUMBER PUNCTURE Materials Materials sterile gloves and mask sterile gloves and mask LP kit (contains: syringe, 25 and 22G needles, 1% lidocaine, sterile drapes, sponges and gauze, 22G LP needle, stopcock and manometer, 4 collection tubes and band-aid) LP kit (contains: syringe, 25 and 22G needles, 1% lidocaine, sterile drapes, sponges and gauze, 22G LP needle, stopcock and manometer, 4 collection tubes and band-aid) - sterilization solution (chlorhexidine or proviodine) - sterilization solution (chlorhexidine or proviodine)
 LP kit (contains: syringe, 25 and 22G needles, 1% lidocaine, sterile drapes, sponges and gauze, 22G LP needle, stopcock and manometer, 4 collection tubes and band-aid) - sterilization solution (chlorhexidine or proviodine) - sterilization solution (chlorhexidine or proviodine)")
116
CSF & LUMBER PUNCTURE Technique Technique 1. Obtain patient consent 1. Obtain patient consent 2. Position the patient,close to edge of bed as possible 2. Position the patient,close to edge of bed as possible 3.Pillow under head and between legs 3.Pillow under head and between legs 4.Head flexed and legs curled up towards chest,ask patient to bulge out lumbosacral spine 4.Head flexed and legs curled up towards chest,ask patient to bulge out lumbosacral spine 5.Carefully open LP kit and put cleaning solution in reservoir. 5.Carefully open LP kit and put cleaning solution in reservoir.

117
Positioning INCORRECT CORRECT

118
CSF & LUMBER PUNCTURE 6.Put on mask and sterile gloves. 6.Put on mask and sterile gloves. 7.Sterilize the field using the sterilizing solution and sponges provided. Clean a 6 inch area around the desired entry site, proceeding outward in concentric circles. Do this 3 separate times. Place sterile drape over the field. 7.Sterilize the field using the sterilizing solution and sponges provided. Clean a 6 inch area around the desired entry site, proceeding outward in concentric circles. Do this 3 separate times. Place sterile drape over the field.

119
Skin Preparation Overlying skin cleaned with povidone-iodine Overlying skin cleaned with povidone-iodine Sterile drape placed with an opening over the LS Sterile drape placed with an opening over the LS

121
Spinal Needle Insertion Local anesthesia infiltrated Local anesthesia infiltrated 20 or 22 gauge spinal needle with stylet 20 or 22 gauge spinal needle with stylet Advance spinal needle slowly, angling slightly toward the head Advance spinal needle slowly, angling slightly toward the head Flat surface of bevel of needle positioned to face patient ’ s flanks Flat surface of bevel of needle positioned to face patient ’ s flanks

122
CSF & LUMBER PUNCTURE 8. Ensure all items in LP tray are ready for use. E.g.. 1% or 2% lidocaine loaded into syringe, collection tubes open, test to see that the stylet slides in/out of LP needle easily, stopcock and manometer for opening pressure measurement ready 8. Ensure all items in LP tray are ready for use. E.g.. 1% or 2% lidocaine loaded into syringe, collection tubes open, test to see that the stylet slides in/out of LP needle easily, stopcock and manometer for opening pressure measurement ready

123
CSF & LUMBER PUNCTURE 9.Local anaesthesia. Using a 25G needle, inject 1% or 2% lidocaine under the skin at the desired entry site. A small bleb under the skin is sufficient. Switch the needle tip to the 22G needle and anaesthetize deeper structures by inserting the needle further, injecting lidocaine while proceeding forward. 9.Local anaesthesia. Using a 25G needle, inject 1% or 2% lidocaine under the skin at the desired entry site. A small bleb under the skin is sufficient. Switch the needle tip to the 22G needle and anaesthetize deeper structures by inserting the needle further, injecting lidocaine while proceeding forward.

124
CSF & LUMBER PUNCTURE 10.Insert LP needle. The bevel should be parallel to the spinal column. Always advance the needle with the stylet in place. Aim needle in the midline, slightly cephalad, towards the patient’s umbilicus. Advance needle slowly until it is inserted 2-3 cm, then withdraw the stylet to check for CSF return. Continue to advance the needle, periodically checking for CSF return. Often a "pop'' is appreciated as the needle pierces the dural membrane. 10.Insert LP needle. The bevel should be parallel to the spinal column. Always advance the needle with the stylet in place. Aim needle in the midline, slightly cephalad, towards the patient’s umbilicus. Advance needle slowly until it is inserted 2-3 cm, then withdraw the stylet to check for CSF return. Continue to advance the needle, periodically checking for CSF return. Often a "pop'' is appreciated as the needle pierces the dural membrane.

125
CSF & LUMBER PUNCTURE If the needle meets bone or if blood returns (hitting the venous plexus anterior or posterior to the spinal canal), withdraw the needle to the skin and redirect the needle If the needle meets bone or if blood returns (hitting the venous plexus anterior or posterior to the spinal canal), withdraw the needle to the skin and redirect the needle
, withdraw the needle to the skin and redirect the needle If the needle meets bone or if blood returns (hitting the venous plexus anterior or posterior to the spinal canal), withdraw the needle to the skin and redirect the needle")
126
CSF & LUMBER PUNCTURE 11.Once CSF flow is obtained, measure the opening pressure by attaching first the stopcock to the LP needle and then the manometer to the stopcock. 11.Once CSF flow is obtained, measure the opening pressure by attaching first the stopcock to the LP needle and then the manometer to the stopcock.

127
CSF & LUMBER PUNCTURE 12.Collect CSF fluid into sequential tubes. about 2 ml in each tube is sufficient for basic investigations. More fluid will need to be collected for special tests e.g. viral PCR, cytology etc 12.Collect CSF fluid into sequential tubes. about 2 ml in each tube is sufficient for basic investigations. More fluid will need to be collected for special tests e.g. viral PCR, cytology etc 13.Reinsert stylet. Withdraw needle. Place band-aid over insertion site. 13.Reinsert stylet. Withdraw needle. Place band-aid over insertion site.

128
CSF & LUMBER PUNCTURE What to order What to order The basics The basics Tube #1 Cell count and differential Tube #1 Cell count and differential Tube #2 Chemistry (protein, glucose) Tube #2 Chemistry (protein, glucose) Tube #3 Culture and Gram stain Tube #3 Culture and Gram stain Tube #4 reserve with csf in it Tube #4 reserve with csf in it
 Tube #2 Chemistry (protein, glucose) Tube #3 Culture and Gram stain Tube #3 Culture and Gram stain Tube #4 reserve with csf in it Tube #4 reserve with csf in it")
129
CSF & LUMBER PUNCTURE Other tests to consider Other tests to consider - Will need to collect extra fluid for these tests in tube #3 or #4. - Will need to collect extra fluid for these tests in tube #3 or #4. India ink and / or Cryptococcal Ag (for Cryptococcus neoformans) India ink and / or Cryptococcal Ag (for Cryptococcus neoformans) AFB and / or PCR for TB AFB and / or PCR for TB Viral PCR (includes HSV, CMV, EBV) Viral PCR (includes HSV, CMV, EBV) arbovirus / WNV, echovirus arbovirus / WNV, echovirus
 India ink and / or Cryptococcal Ag (for Cryptococcus neoformans) AFB and / or PCR for TB AFB and / or PCR for TB Viral PCR (includes HSV, CMV, EBV) Viral PCR (includes HSV, CMV, EBV) arbovirus / WNV, echovirus arbovirus / WNV, echovirus.")
130
CSF & LUMBER PUNCTURE VDRL VDRL fungal culture fungal culture viral culture viral culture PCR and /or antibody titers for Lyme ds. PCR and /or antibody titers for Lyme ds.

131
CSF & LUMBER PUNCTURE oligoclonal banding (3-4 ml) oligoclonal banding (3-4 ml) IgG index, IgG :albumin ratio IgG index, IgG :albumin ratio cytology (must be collected in cytology fixative) (8-10ml) cytology (must be collected in cytology fixative) (8-10ml) flow cytometry (3-4 ml) (NOT in fixative) flow cytometry (3-4 ml) (NOT in fixative)
 oligoclonal banding (3-4 ml) IgG index, IgG :albumin ratio IgG index, IgG :albumin ratio cytology (must be collected in cytology fixative) (8-10ml) cytology (must be collected in cytology fixative) (8-10ml) flow cytometry (3-4 ml) (NOT in fixative) flow cytometry (3-4 ml) (NOT in fixative)")
132
CSF & LUMBER PUNCTURE How much CSF to withdraw? How much CSF to withdraw? - CSF is produced at a rate of 0.3 ml/min in adults or 450 ml/24h - CSF is produced at a rate of 0.3 ml/min in adults or 450 ml/24h - CSF volume is approximately 150 ml in an adult - CSF volume is approximately 150 ml in an adult

133
CSF & LUMBER PUNCTURE - For basic investigations, only require 4-8 ml - For basic investigations, only require 4-8 ml - May require more volume for special tests. Maximum to be removed at one time should probably not exceed 20 ml. - May require more volume for special tests. Maximum to be removed at one time should probably not exceed 20 ml.

134
CSF & LUMBER PUNCTURE Normal opening pressure ranges 50 to 200 mm H20 in adults and up to 250 mm H20 in obese women patients or 5-20 cm of H20. Normal opening pressure ranges 50 to 200 mm H20 in adults and up to 250 mm H20 in obese women patients or 5-20 cm of H20. 2 Intracranial hypotension is defined as an opening pressure of less than 50 mm H20. 2 Intracranial hypotension is defined as an opening pressure of less than 50 mm H20.

135
CSF & LUMBER PUNCTURE Normal CSF is crystal clear. However, as few as 200 white blood cells (WBCs) per mm3 or 400 red blood cells (RBCs) per mm3 will cause CSF to appear turbid. Normal CSF is crystal clear. However, as few as 200 white blood cells (WBCs) per mm3 or 400 red blood cells (RBCs) per mm3 will cause CSF to appear turbid.
 per mm3 or 400 red blood cells (RBCs) per mm3 will cause CSF to appear turbid. Normal CSF is crystal clear. However, as few as 200 white blood cells (WBCs) per mm3 or 400 red blood cells (RBCs) per mm3 will cause CSF to appear turbid..")
136
CSF & LUMBER PUNCTURE Glucose: 2/3rd or < 40% of concurrent serum glucose or less than 2/3 rd of serum glucose (often absolute CSF glucose < 2.2, (normal is 2.2 mmol to 4 mmol/l) Glucose: 2/3rd or < 40% of concurrent serum glucose or less than 2/3 rd of serum glucose (often absolute CSF glucose < 2.2, (normal is 2.2 mmol to 4 mmol/l) cells <5/cmm mostly lymphocyte cells <5/cmm mostly lymphocyte
 Glucose: 2/3rd or < 40% of concurrent serum glucose or less than 2/3 rd of serum glucose (often absolute CSF glucose < 2.2, (normal is 2.2 mmol to 4 mmol/l) cells <5/cmm mostly lymphocyte cells <5/cmm mostly lymphocyte")
137
CSF & LUMBER PUNCTURE Xanthochromia is a yellow, orange, or pink discoloration of the CSF, most often caused by the lysis of RBCs resulting in hemoglobin breakdown to oxyhemoglobin, Xanthochromia is a yellow, orange, or pink discoloration of the CSF, most often caused by the lysis of RBCs resulting in hemoglobin breakdown to oxyhemoglobin, methemoglobin, and bilirubin. methemoglobin, and bilirubin.

138
CSF & LUMBER PUNCTURE Discoloration begins after RBCs have been in spinal fluid for about two hours, and remains for two to four weeks. Discoloration begins after RBCs have been in spinal fluid for about two hours, and remains for two to four weeks. Xanthochromia is present in more than 90 percent of patients within 12 hours of subarachnoid hemorrhage Xanthochromia is present in more than 90 percent of patients within 12 hours of subarachnoid hemorrhage

139
CSF & LUMBER PUNCTURE CSF protein levels (normal 15 to 45 mg/dL ) or < 1.5 g per L. CSF protein levels (normal 15 to 45 mg/dL ) or < 1.5 g per L.
 or < 1.5 g per L..")
140
CSF & LUMBER PUNCTURE Culture provides definitive diagnosis as well as identificaiton of pathogenic organism and antibiotic susceptibilities Culture provides definitive diagnosis as well as identificaiton of pathogenic organism and antibiotic susceptibilities blood culture positive in 50% cases blood culture positive in 50% cases

141
CSF & LUMBER PUNCTURE The Xpert EV test, approved for use in March 2007, can rapidly test for enteroviral meningitis. The test uses a reverse-transcription PCR disposable cartridge on which CSF is applied, and enteroviral genetic material is identified if present. Results are ready in 2.5 hours, as opposed to days to weeks in traditional PCR studies. The Xpert EV test, approved for use in March 2007, can rapidly test for enteroviral meningitis. The test uses a reverse-transcription PCR disposable cartridge on which CSF is applied, and enteroviral genetic material is identified if present. Results are ready in 2.5 hours, as opposed to days to weeks in traditional PCR studies.

142
CSF & LUMBER PUNCTURE CT scan with contrast helps in ruling out intracranial pathology. Contrasted scans should be obtained to evaluate for any enhancement along the meninges. CT scan with contrast helps in ruling out intracranial pathology. Contrasted scans should be obtained to evaluate for any enhancement along the meninges. ct scan also excludes intracranial abscess, subdural empyema, or other lesions. Alternatively, and if readily available, an MRI of the brain should be done. ct scan also excludes intracranial abscess, subdural empyema, or other lesions. Alternatively, and if readily available, an MRI of the brain should be done.

143
CSF & LUMBER PUNCTURE MRI with contrast is the criterion standard in visualizing intracranial pathology in viral encephalitis HSV-1 commonly affects basal frontal and temporal lobes with a typical picture of diffusely enhancing bilateral lesions. MRI with contrast is the criterion standard in visualizing intracranial pathology in viral encephalitis HSV-1 commonly affects basal frontal and temporal lobes with a typical picture of diffusely enhancing bilateral lesions.

144
CSF & LUMBER PUNCTURE All patients whose condition is not improving clinically within 24-48 hours should have more extensive work-up to discern the cause of meningitis. All patients whose condition is not improving clinically within 24-48 hours should have more extensive work-up to discern the cause of meningitis. Blood, feces, and throat swabs may be sent for viral serology and cultures. Blood, feces, and throat swabs may be sent for viral serology and cultures.

145
CSF & LUMBER PUNCTURE Acid-fast staining of CSF should be performed and the remaining fluid should be sent for PCR testing for HIV and CMV. Acid-fast staining of CSF should be performed and the remaining fluid should be sent for PCR testing for HIV and CMV. Serum titers of antibodies against HIV and toxoplasma should be obtained. Serum titers of antibodies against HIV and toxoplasma should be obtained.

146
CSF & LUMBER PUNCTURE EEG may be performed if encephalitis or subclinical seizures are suspected in the altered patient. Periodic lateralized epileptiform discharges (PLEDs) are often seen in herpetic encephalitis. EEG may be performed if encephalitis or subclinical seizures are suspected in the altered patient. Periodic lateralized epileptiform discharges (PLEDs) are often seen in herpetic encephalitis.
 are often seen in herpetic encephalitis. EEG may be performed if encephalitis or subclinical seizures are suspected in the altered patient. Periodic lateralized epileptiform discharges (PLEDs) are often seen in herpetic encephalitis..")
147
CSF & LUMBER PUNCTURE CSF Lactate Concentration CSF Lactate Concentration normally 14 mg/dl normally 14 mg/dl in bacterial meningitis is usually <25 mg/dl in bacterial meningitis is usually <25 mg/dl PCR for microbial DNA may become sensitive and specific method for bacterial identification PCR for microbial DNA may become sensitive and specific method for bacterial identification

148
CSF & LUMBER PUNCTURE CT Scanning sould be done and preferred choice before Lumbar Puncture in Suspected Meningitis CT Scanning sould be done and preferred choice before Lumbar Puncture in Suspected Meningitis Acid-fast staining of CSF should be performed and the remaining fluid should be sent for PCR testing for HIV and CMV. Acid-fast staining of CSF should be performed and the remaining fluid should be sent for PCR testing for HIV and CMV. Serum titers of antibodies against HIV and toxoplasma should be obtained. Serum titers of antibodies against HIV and toxoplasma should be obtained.

149
CSF & LUMBER PUNCTURE Additional serum collection 10-21 days later may aid in discerning rising titers in the antibodies against specific viral pathogens; a 4-fold increase in viral antibodies confirms the diagnosis. This is particularly useful for arboviral and LCMV cases, but also is helpful in ruling out toxoplasmosis, leptospirosis, borreliosis, and rickettsial infections. Although some of these studies do not yield an immediate result for clinical decision making, they may be useful for prognostication. Additional serum collection 10-21 days later may aid in discerning rising titers in the antibodies against specific viral pathogens; a 4-fold increase in viral antibodies confirms the diagnosis. This is particularly useful for arboviral and LCMV cases, but also is helpful in ruling out toxoplasmosis, leptospirosis, borreliosis, and rickettsial infections. Although some of these studies do not yield an immediate result for clinical decision making, they may be useful for prognostication.

150
CSF PRESSURE Opening pressure: 5-20 cm water (only valid in lateral decubitus position) or 50- 200 mm of H20. Opening pressure: 5-20 cm water (only valid in lateral decubitus position) or 50- 200 mm of H20.
 or mm of H20..")
151
CSF PRESSURE ICP is measured in millimeters of mercury (mmHg) and, at rest, is normally 5–20 mmHg for a supine adult, and becomes negative (averaging -10 mmHg) in the vertical position. ICP is measured in millimeters of mercury (mmHg) and, at rest, is normally 5–20 mmHg for a supine adult, and becomes negative (averaging -10 mmHg) in the vertical position.
 and, at rest, is normally 5–20 mmHg for a supine adult, and becomes negative (averaging -10 mmHg) in the vertical position..")
152
CSF PRESSURE Normal CSF pressure in the lower back is between 50-200 mm water. Normal CSF pressure in the lower back is between 50-200 mm water. Normal Intracranial pressure(within the cranium) however is between 5-20 mmHg or 50-200 mm H2O in adults. Normal Intracranial pressure(within the cranium) however is between 5-20 mmHg or 50-200 mm H2O in adults.
 however is between 5-20 mmHg or mm H2O in adults. Normal Intracranial pressure(within the cranium) however is between 5-20 mmHg or mm H2O in adults..")
153
Investigations & Diagnosis of Meningitis Repeat CSF analysis 24 to 36 hours (minimum of 24 hours) after initiation of therapy Repeat CSF analysis 24 to 36 hours (minimum of 24 hours) after initiation of therapy Changes in therapy/concomitant therapy as needed Changes in therapy/concomitant therapy as needed Evaluation of drug concentrations in CSF Evaluation of drug concentrations in CSF
 after initiation of therapy Repeat CSF analysis 24 to 36 hours (minimum of 24 hours) after initiation of therapy Changes in therapy/concomitant therapy as needed Changes in therapy/concomitant therapy as needed Evaluation of drug concentrations in CSF Evaluation of drug concentrations in CSF")
154
Investigations & Diagnosis of Meningitis 5-7 weeks after completion of all therapy 5-7 weeks after completion of all therapy Lumbar puncture repeated only if clinically indicated Lumbar puncture repeated only if clinically indicated

155
Investigations & Diagnosis of Meningitis LATE POST-THERAPY VISIT LATE POST-THERAPY VISIT 5-6 months after completion of therapy 5-6 months after completion of therapy Emphasis on hearing/ development/ neurological findings Emphasis on hearing/ development/ neurological findings Behavioral difficulties should be documented as well Behavioral difficulties should be documented as well

156
Investigations & Diagnosis of Meningitis Persistence of pathogen at 24-36 hr. tap leading to additional therapy or change in therapy. Persistence of pathogen at 24-36 hr. tap leading to additional therapy or change in therapy.

157
CSF evaluation ConditionWBC Protein (mg/dL) Glucose (mg/dL) Normal <5, lymphocytes mainly 5-45 >50 (2.2 mmol to 4 mmol/l) Bacterial, acute >1000K PMN’s 100-500 or >1.5gm/l <2.2 m mol/l Viral<1000increased Low to normal TB<500increaseddecreased Fungal < 500 increaseddecreased
 Glucose (mg/dL) Normal <5, lymphocytes mainly 5-45 >50 (2.2 mmol to 4 mmol/l) Bacterial, acute >1000K PMN’s or >1.5gm/l <2.2 m mol/l Viral<1000increased Low to normal TB<500increaseddecreased Fungal < 500 increaseddecreased")
158
CSF Diagnosis WBCGlucoseProtein Normal <5 (lymphocytes) <5 (lymphocytes) 2/3 rd of serum glucose 15 to 45 mg/dl Bacterial Meningitis >1000 PMN’s predominate Low Elevated (>100 mg) Aseptic Meningitis Elevated (PMN’s early, lymphocytes late) Normal to low Normal or slightly elevated TB Meningitis Elevated (PMN’s early, lymphs late Low Elevated (>100 mg)
 <5 (lymphocytes) 2/3 rd of serum glucose 15 to 45 mg/dl Bacterial Meningitis >1000 PMN’s predominate Low Elevated (>100 mg) Aseptic Meningitis Elevated (PMN’s early, lymphocytes late) Normal to low Normal or slightly elevated TB Meningitis Elevated (PMN’s early, lymphs late Low Elevated (>100 mg)")
159
CSF evaluation ConditionWBC Protein (mg/dL) Glucose (mg/dL) Normal <5, lymph's mainly 5-45>50 Bacterial, acute >1000 PMN’s Increased> more than 100 mg/d Low TB<500 Increased upto 500 mg/dl low Fungal<500 Upto 500 low Viral<1000 Upto 100 Normal
 Glucose (mg/dL) Normal <5, lymph s mainly 5-45>50 Bacterial, acute >1000 PMN’s Increased> more than 100 mg/d Low TB<500 Increased upto 500 mg/dl low Fungal<500 Upto 500 low Viral<1000 Upto 100 Normal")
160
Summary of Typical CSF Findings NormalBacterialViralTB Cells 0-5 0-5>1000<1000<500 Polymorphs 0PredominateEarly +/- increased Lymphocytes 5LatePredominateIncreased Glucose60-80DecreasedNormalDecreased CSF plasma: Glucose ratio 66%<40%Normal < 30% Protein5-40Increased +/- Increased Increased CultureNegativePositiveNegative+TB

161
TREATMENT of MENINGITIS Empiric Antibiotics: Empiric Antibiotics: Cefotaxime 2g IV 6 hrly Cefotaxime 2g IV 6 hrly add Vancomycin 1-2 g IV 8-12 hrly in all patients (till possibility of Penicillin-resistant Strep pneumoniae has been ruled out) add Vancomycin 1-2 g IV 8-12 hrly in all patients (till possibility of Penicillin-resistant Strep pneumoniae has been ruled out) add Ampicllin 2g IV 6 hrly in elderly or immunocompromised patients (for Listeria infections) add Ampicllin 2g IV 6 hrly in elderly or immunocompromised patients (for Listeria infections)
 add Vancomycin 1-2 g IV 8-12 hrly in all patients (till possibility of Penicillin-resistant Strep pneumoniae has been ruled out) add Ampicllin 2g IV 6 hrly in elderly or immunocompromised patients (for Listeria infections) add Ampicllin 2g IV 6 hrly in elderly or immunocompromised patients (for Listeria infections)")
162
TREATMENT of MENINGITIS for patients with serious penicillin allergies, Meropenem 1-2g IV 8hrly as alternative for patients with serious penicillin allergies, Meropenem 1-2g IV 8hrly as alternative Ceftazidime (2g IV 8 hrly or BD) + Vancomycin for neurosurgical patients, those with shunts or CSF leaks Ceftazidime (2g IV 8 hrly or BD) + Vancomycin for neurosurgical patients, those with shunts or CSF leaks May consider adjunctive Acyclovir (10 mg/kg IV 8 hrly if normal renal function) in case of viral infection. May consider adjunctive Acyclovir (10 mg/kg IV 8 hrly if normal renal function) in case of viral infection.
 in case of viral infection..")
163
TREATMENT of MENINGITIS Therapy can be modified as the results of Gram stain, cultures, and PCR testing become available. Patients in unstable condition need critical care unit admission for airway protection, neurologic checks, and prevention of secondary complications. Therapy can be modified as the results of Gram stain, cultures, and PCR testing become available. Patients in unstable condition need critical care unit admission for airway protection, neurologic checks, and prevention of secondary complications.

164
TREATMENT of MENINGITIS since SIADH has been reported. Fluid restriction, diuretics, and rarely hypertonic saline infusion may be used to correct the hyponatremia since SIADH has been reported. Fluid restriction, diuretics, and rarely hypertonic saline infusion may be used to correct the hyponatremia

165
TREATMENT of MENINGITIS Cerebral edema does occur in cases of severe encephalitis and may require intracranial pressure control by infusion of mannitol (1 g/kg initial dose followed by 0.25-0.5 g/kg 6 hrly), IV dexamethasone, or intubation and mild hyperventilation, with arterial PCO2 around 28-30 mm Hg Cerebral edema does occur in cases of severe encephalitis and may require intracranial pressure control by infusion of mannitol (1 g/kg initial dose followed by 0.25-0.5 g/kg 6 hrly), IV dexamethasone, or intubation and mild hyperventilation, with arterial PCO2 around 28-30 mm Hg
, IV dexamethasone, or intubation and mild hyperventilation, with arterial PCO2 around mm Hg Cerebral edema does occur in cases of severe encephalitis and may require intracranial pressure control by infusion of mannitol (1 g/kg initial dose followed by g/kg 6 hrly), IV dexamethasone, or intubation and mild hyperventilation, with arterial PCO2 around mm Hg")
166
TREATMENT of MENINGITIS Use of adjunctive corticosteroids: Use of adjunctive corticosteroids: - prior to or along with initial antibiotics, administer Dexamethasone 10 mg IV for suspected bacterial meningitis (based on cloudy CSF, CSF WBC counts > 1000 or + Gram stain) - prior to or along with initial antibiotics, administer Dexamethasone 10 mg IV for suspected bacterial meningitis (based on cloudy CSF, CSF WBC counts > 1000 or + Gram stain) - continue 10 mg IV 8 hrly x 4 days - continue 10 mg IV 8 hrly x 4 days
 - prior to or along with initial antibiotics, administer Dexamethasone 10 mg IV for suspected bacterial meningitis (based on cloudy CSF, CSF WBC counts > 1000 or + Gram stain) - continue 10 mg IV 8 hrly x 4 days - continue 10 mg IV 8 hrly x 4 days")
167
TREATMENT of MENINGITIS Isolation & Contact Prophylaxis: Isolation & Contact Prophylaxis: - Generally isolate cases of bacterial meningitis for up to 48 hours of appropriate antibiotics - Generally isolate cases of bacterial meningitis for up to 48 hours of appropriate antibiotics - Concern is to reduce transmission of meningococcal infections - Concern is to reduce transmission of meningococcal infections

168
TREATMENT of MENINGITIS can be taken out of isolation after this time or if alternative pathogen identified can be taken out of isolation after this time or if alternative pathogen identified - department of health should be notified of pathogens in pyogenic meningitis - department of health should be notified of pathogens in pyogenic meningitis

169
TREATMENT of MENINGITIS Close contacts (family members, partners, co-workers or school children) should receive prophylaxis if meningococcal or haemophilus influenzae type B (if not vaccinated): Close contacts (family members, partners, co-workers or school children) should receive prophylaxis if meningococcal or haemophilus influenzae type B (if not vaccinated): - rifampin 600 mg PO bid x 2d - rifampin 600 mg PO bid x 2d - ciprofloxacin 500 mg PO single dose - ciprofloxacin 500 mg PO single dose
 should receive prophylaxis if meningococcal or haemophilus influenzae type B (if not vaccinated): Close contacts (family members, partners, co-workers or school children) should receive prophylaxis if meningococcal or haemophilus influenzae type B (if not vaccinated): - rifampin 600 mg PO bid x 2d - rifampin 600 mg PO bid x 2d - ciprofloxacin 500 mg PO single dose - ciprofloxacin 500 mg PO single dose")
170
TREATMENT of MENINGITIS dexamethasone 0.6 mg/kg/day IV 6-8 hrly for 4 days dexamethasone 0.6 mg/kg/day IV 6-8 hrly for 4 days reduces incidence of neurologic sequelae, i.e., hearing loss reduces incidence of neurologic sequelae, i.e., hearing loss electrolyte abnormalities - SIADH electrolyte abnormalities - SIADH

171
Prognostic Factors 1. Age 1. Age 2. Level of Consciousness (50% mortality if unresponsive or minimally responsive on admission) 2. Level of Consciousness (50% mortality if unresponsive or minimally responsive on admission) 3. Seizures early in course 3. Seizures early in course 4. Strep. pneumoniae meningitis 4. Strep. pneumoniae meningitis 5. CSF results (lower glucose & WBC counts, higher protein) 5. CSF results (lower glucose & WBC counts, higher protein)
 2. Level of Consciousness (50% mortality if unresponsive or minimally responsive on admission) 3. Seizures early in course 3. Seizures early in course 4. Strep. pneumoniae meningitis 4. Strep. pneumoniae meningitis 5. CSF results (lower glucose & WBC counts, higher protein) 5. CSF results (lower glucose & WBC counts, higher protein).")
Similar presentations
















. >")







