Download presentation
Presentation is loading. Please wait.

1
Jenna Chiu August 2014

2
Background Study hypothesis Methods Results Analysis Future practice

3
Common presentation to ED National Asthma Council Australia ◦ Australian Asthma Handbook 2014 British Thoracic Society / Scottish Intercollegiate Guidelines Network ◦ British Guidelines on the Management of Asthma 2012

4
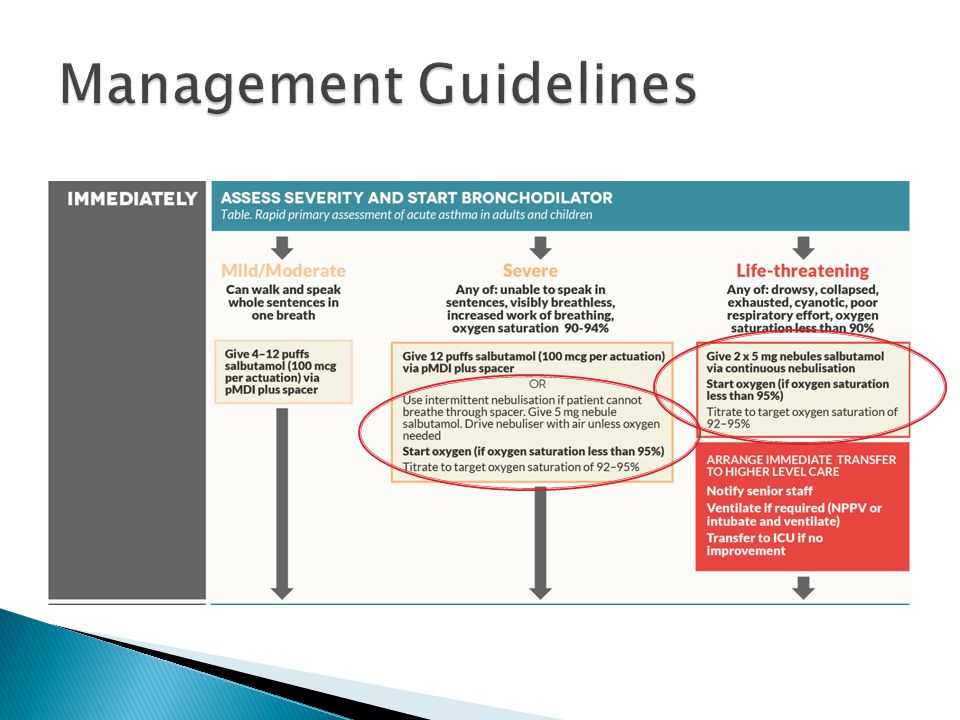
Australian guidelines Can walk and speak whole sentences in one breath British guidelines Increasing symptoms PEF > 50-75% best or predicted No features of acute severe asthma

5
Australian guidelines Unable to speak in sentences Visibly breathless Increased work of breathing Oxygen saturation 90-94 % British guidelines Inability to complete sentences in one breath PEF 33-50% best or predicted RR ≥ 25/min HR ≥ 110/min

6
Australian guidelines Drowsy Collapsed Exhausted Cyanotic Poor respiratory effort Oxygen saturation < 90% British guidelines Altered conscious level Exhaustion Arrhythmia Hypotension Cyanosis Silent chest Poor respiratory effort PEF < 33% best or predicted SpO 2 < 92% PaO2 < 8kPa “normal” PaCO 2 (4.6-6.0 kPa)
")
11
AGENTRECOMMENDED USE IN ACUTE ASTHMA Administration and dosage Notes IV magnesium sulphate Second-line bronchodilator in severe or life- threatening acute asthma, or when poor response to repeated maximal doses of other bronchodilators IV infusion over 20 minutes Adults: 2g (20 mmol) Children ≥ 2 years: 0.1-0.2 mmol/kg Avoid magnesium sulphate in children younger than 2 years
 Children ≥ 2 years: mmol/kg Avoid magnesium sulphate in children younger than 2 years")
13
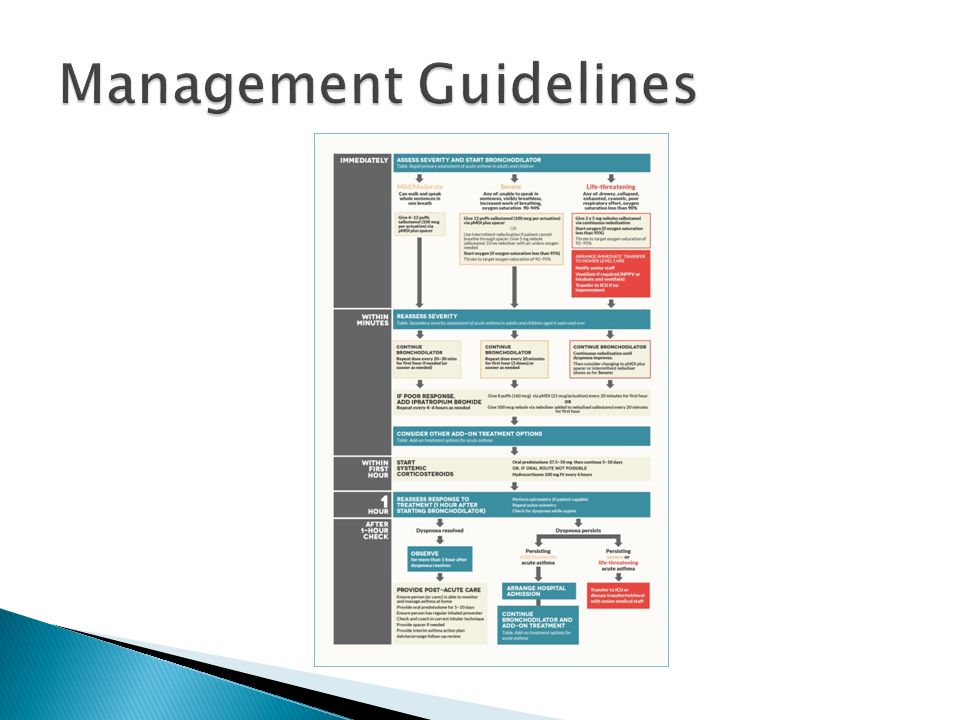
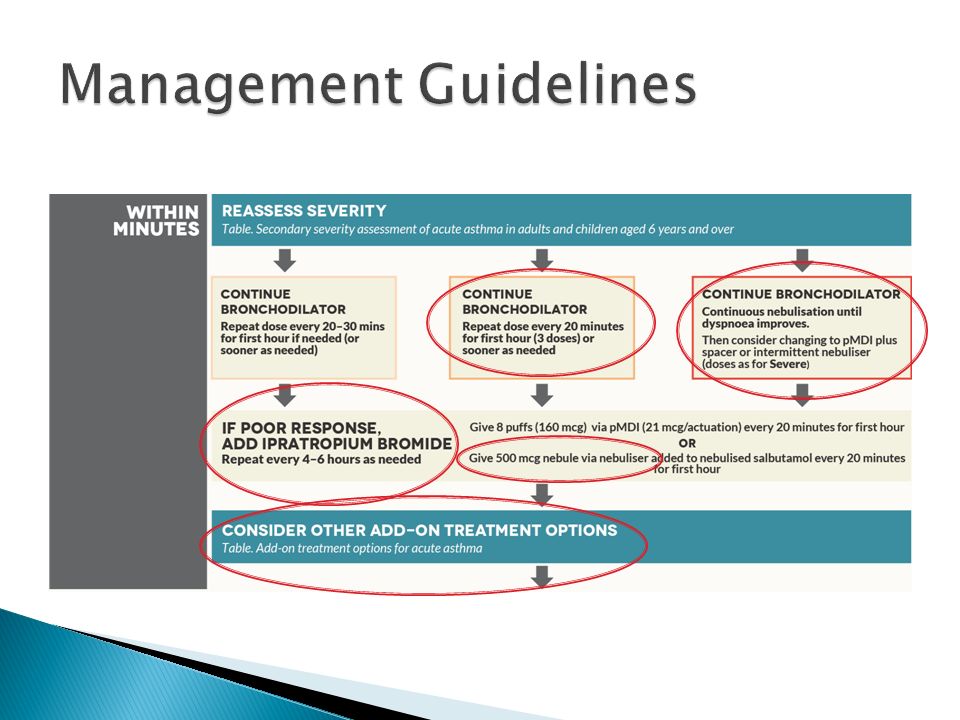
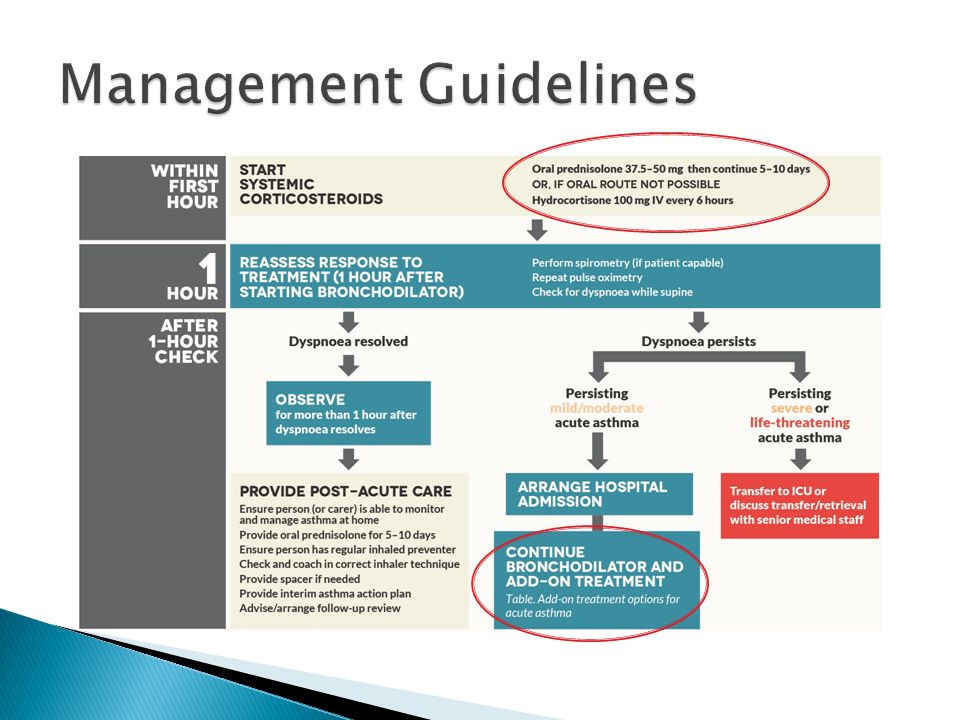
Stepwise approach to the management of acute asthma including oxygen, nebulisers and steroids Bronchodilators act within minutes whereas corticosteroids require hours to take effect

14
Potential role for magnesium sulphate (MgSO 4 ) as an additional treatment option in the therapeutic gap between nebulised bronchodilators and corticosteroids
 as an additional treatment option in the therapeutic gap between nebulised bronchodilators and corticosteroids")
15
Advantages Quick onset of action Reduced incidence of side-effects Disadvantages Reduced dose of drug delivered compared with the intravenous form Respiratory effort on the part of the patient to increase its effectiveness

16
Advantages Provides direct access to the venous system allowing delivery of high drug concentrations Disadvantages Need for intravenous access Drug administration by infusion lasting 20 mins

17
Differing conclusions regarding the effectiveness of treatment Previous primary outcome- PEFR No trials have directly compared intravenous MgSO 4 with nebulised MgSO 4 No recommendations are made regarding nebulised MgSO 4

18
Multicentre double-blind randomised placebo-controlled trial across 34 emergency departments in the UK July 2008 – June 2012

19
Adults (aged ≥ 16 years) attending an ED with severe acute asthma ◦ Acute asthma with either a PEFR < 50% of best or predicted, RR ≥ 25/min, HR ≥ 110/min, or inability to complete sentences in one breath Written or verbal consent obtained
 attending an ED with severe acute asthma ◦ Acute asthma with either a PEFR < 50% of best or predicted, RR ≥ 25/min, HR ≥ 110/min, or inability to complete sentences in one breath Written or verbal consent obtained")
20
Exclusion criteria ◦ Life-threatening features (oxygen saturation < 92%, silent chest, cyanosis, poor respiratory effort, bradycardia, arrhythmia, hypotension, exhaustion, coma, or confusion) ◦ Contraindication to either nebulised or intravenous MgSO 4 (pregnancy, hepatic or renal failure, heart block, or known hypermagnesaemia) ◦ Individuals who were unable to provide written or verbal consent ◦ Individuals who had received MgSO 4 in the 24 h prior to recruitment
 ◦ Contraindication to either nebulised or intravenous MgSO 4 (pregnancy, hepatic or renal failure, heart block, or known hypermagnesaemia) ◦ Individuals who were unable to provide written or verbal consent ◦ Individuals who had received MgSO 4 in the 24 h prior to recruitment")
21
Randomly allocated with either a telephone or internet randomisation sequence Given numbered treatment packs Each treatment pack contained an intravenous infusion and three nebuliser solutions, either which could be active treatment or placebo Participants, hospital staff, and research staff were masked to allocated treatment

22
Intravenous MgSO 4 group IV MgSO 4 (8 mmol [2 g] in 100 mL normal saline provided over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals Nebulised MgSO 4 group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 2 mmol (500mg) MgSO 4 nebulised at 20 min intervals Placebo group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals
![Intravenous MgSO 4 group IV MgSO 4 (8 mmol [2 g] in 100 mL normal saline provided over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals Nebulised MgSO 4 group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 2 mmol (500mg) MgSO 4 nebulised at 20 min intervals Placebo group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals](http://images.slideplayer.com/41/11194753/slides/slide_22.jpg "Intravenous MgSO 4 group IV MgSO 4 (8 mmol [2 g] in 100 mL normal saline provided over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals Nebulised MgSO 4 group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 2 mmol (500mg) MgSO 4 nebulised at 20 min intervals Placebo group IV normal saline (100 mL given over 20 min) + three 7.5 mL vials of 0.9% saline nebulised at 20 min intervals")
23
Standard therapy ◦ Oxygen ◦ Nebulised salbutamol (5 mg) ◦ Nebulised ipratropium (500 g) ◦ Oral prednisolone ◦ Additional – nebulised salbutamol (5 mg) added to each trial nebuliser
 ◦ Nebulised ipratropium (500 g) ◦ Oral prednisolone ◦ Additional – nebulised salbutamol (5 mg) added to each trial nebuliser")
24
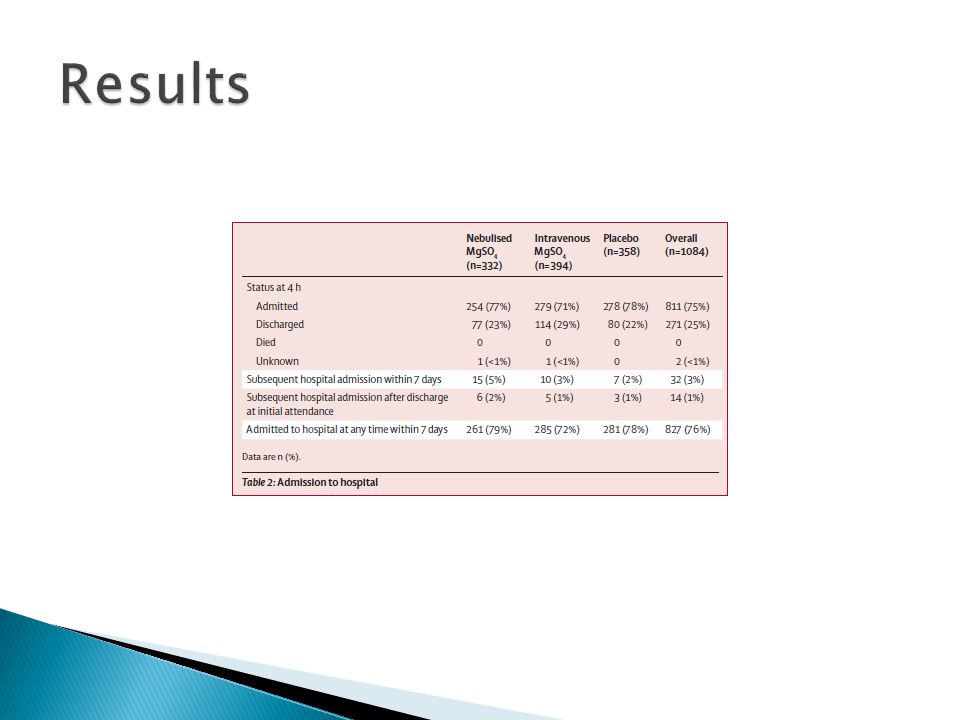
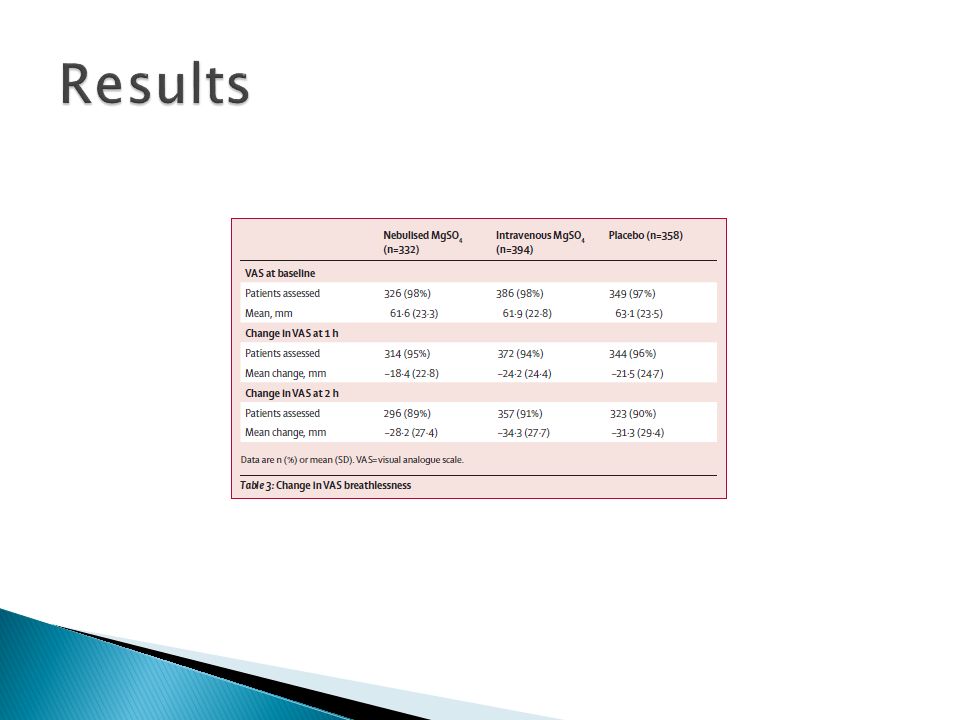
Primary outcome measures 1) Proportion of patients admitted to hospital within 7 days 2) Patient’s visual analogue scale (VAS) for breathlessness in the 2 h after initiation of treatment
 Proportion of patients admitted to hospital within 7 days 2) Patient’s visual analogue scale (VAS) for breathlessness in the 2 h after initiation of treatment")
25
Power calculation ◦ For 90% power to detect a 10% change in admission rate would require 1200 patients, i.e. 400 patients in each group ◦ Assuming 80% of participants had a VAS measurement, this would provide a 90% power to detect an 8 mm difference in a 100 mm VAS at 2 h after treatment initiation

26
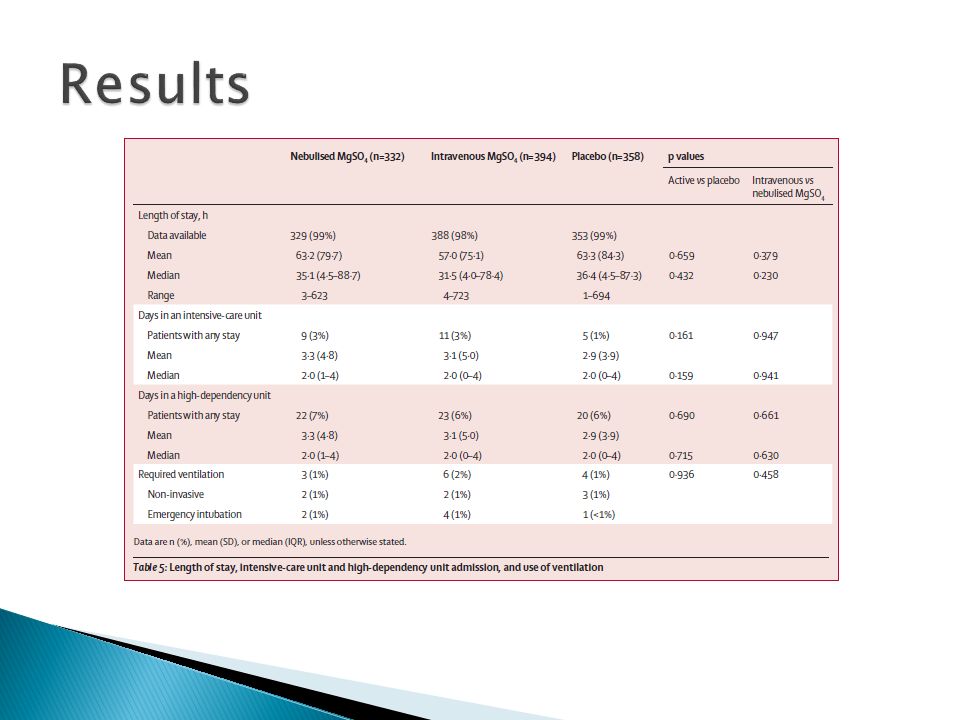
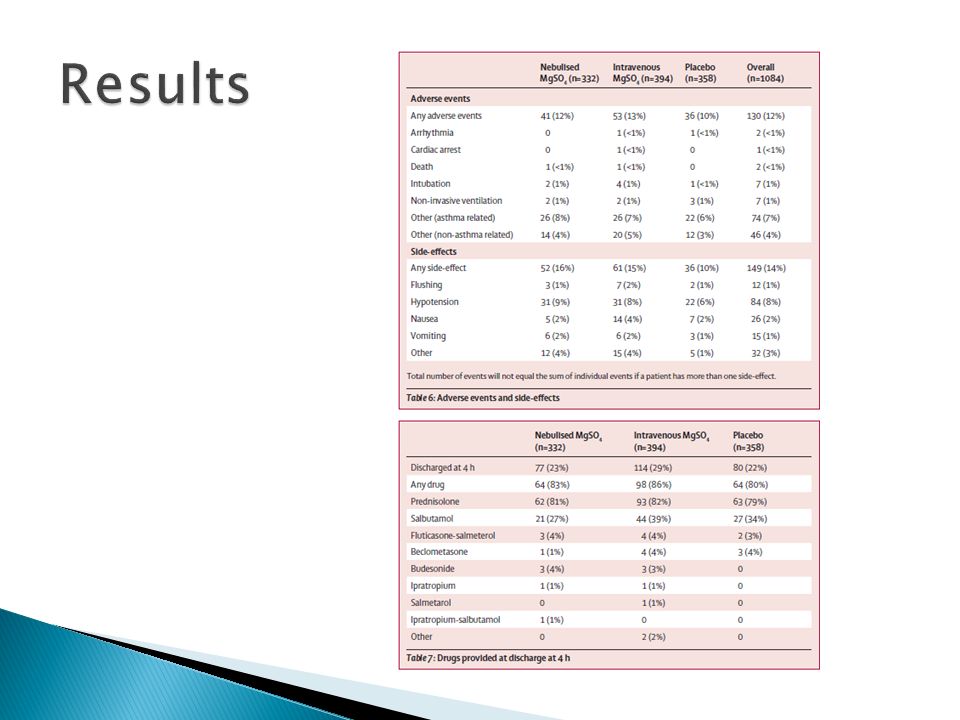
Secondary outcomes ◦ Mortality ◦ Adverse events ◦ Use of ventilation or respiratory support ◦ Length of hospital stay ◦ Admission to a HDU or ICU ◦ Change in peak expiratory flow rate ◦ Physiological variables (oxygen saturation, heart rate, respiratory rate, blood pressure) over 2 h ◦ Change in quality of life between baseline and 1 month ◦ Number of unscheduled health-care contacts over the subsequent month ◦ Satisfaction with care
 over 2 h ◦ Change in quality of life between baseline and 1 month ◦ Number of unscheduled health-care contacts over the subsequent month ◦ Satisfaction with care")
33
Our findings suggest nebulised MgSO 4 has no role in the management of severe acute asthma in adults and at best suggest only a limited role of intravenous MgSO 4 in this setting

34
Relevance Value ◦ Largest trial of MgSO 4 undertaken in acute asthma ◦ Directly compares intravenous treatment with nebulised treatment Study Design ◦ Multicentre, double-blind, placebo-controlled, randomised trial ◦ Involved 34 emergency departments across UK

35
Comparison with previous studies ◦ Differing results Limitations ◦ Underpowered ◦ Primary outcomes and their relevance ◦ Exclusion of life-threatening asthma ◦ Unable to power study to detect differences in serious adverse outcomes (including death) ◦ Co-morbidities not evaluated
 ◦ Co-morbidities not evaluated")
36
Unlikely to change our current practice using intravenous MgSO 4 Unlikely to commence using nebulised MgSO 4 in adults Further studies in the future with different treatment endpoints

37
National Asthma Council Australia. http://http://www.asthmahandbook.org.au/ (accessed Aug 3, 2014) http://http://www.asthmahandbook.org.au/ British Thoracic Society/Scottish Guidelines Intercollegiate Network. https://www.brit- thoracic.org.uk/document-library/clinical- information/asthma/btssign-guideline-on-the- management-of-asthma/ (accessed Aug 3, 2014)https://www.brit- thoracic.org.uk/document-library/clinical- information/asthma/btssign-guideline-on-the- management-of-asthma/ Mohammed S, Goodacre S. Intravenous and nebulised magnesium sulphate for acute asthma: systematic review and meta-analysis. Emerg Med J 2007; 24:823-30
 British Thoracic Society/Scottish Guidelines Intercollegiate Network. thoracic.org.uk/document-library/clinical- information/asthma/btssign-guideline-on-the- management-of-asthma/ (accessed Aug 3, 2014) thoracic.org.uk/document-library/clinical- information/asthma/btssign-guideline-on-the- management-of-asthma/ Mohammed S, Goodacre S. Intravenous and nebulised magnesium sulphate for acute asthma: systematic review and meta-analysis. Emerg Med J 2007; 24:")
Similar presentations
>")


 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")


:>")
 trial.>")



>")
: i1-i92.>")






