Download presentation
Presentation is loading. Please wait.

3
Presented by Mehrzad Bahtouee, MD Internist, Pulmonologist Assistant Professor of Internal Medicine Boushehr University of Medical sciences

4
A common diseases Worldwide prevalence of 7 to 10% A common reason for urgent care and emergency department visits Children > Adults, Black > whites, Hispanics > Non-Hispanics, Women > Men (twice)
")
5
10% → hospitalization Difference in responsiveness to treatment ( Degree of airway inflammation, Presence or absence of mucus plugging, Individual responsiveness to β 2 -adrenergic and corticosteroid medications) Which patients can be discharged quickly and which need to be hospitalized
 Which patients can be discharged quickly and which need to be hospitalized")
6
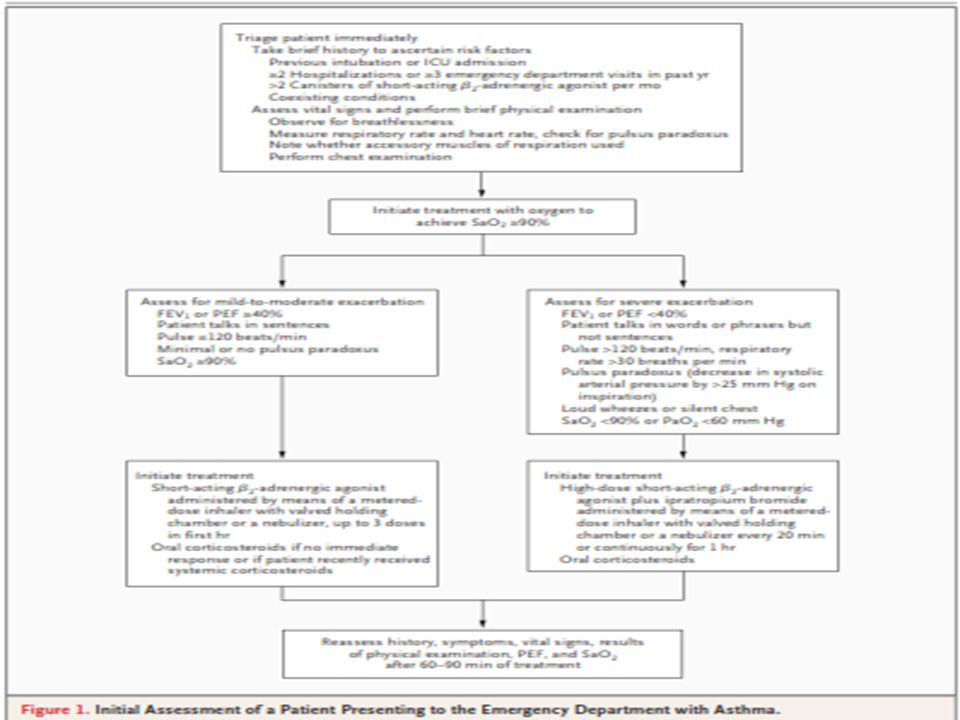
Quick evaluation and triage to assess the severity of the exacerbation and the need for urgent intervention A brief history and a limited physical examination, not delaying treatment Search for signs of life threatening asthma (e.g., altered mental status, paradoxical chest or abdominal movement, absence of wheezing) Factors associated with an increased risk of death from asthma: previous intubation or admission to an ICU, two or more hospitalizations for asthma during the past year, low socioeconomic status, coexisting illnesses
 Factors associated with an increased risk of death from asthma: previous intubation or admission to an ICU, two or more hospitalizations for asthma during the past year, low socioeconomic status, coexisting illnesses")
7
Measurement of lung function (FEV1, PEF) → Severity, response to treatment Laboratory and imaging studies selectively, (e.g., partial pressure of arterial carbon dioxide [PaCO 2 ]), complete blood count or a chest radiograph, electrocardiogram)
![ Measurement of lung function (FEV1, PEF) → Severity, response to treatment Laboratory and imaging studies selectively, (e.g., partial pressure of arterial carbon dioxide [PaCO 2 ]), complete blood count or a chest radiograph, electrocardiogram)](http://images.slideplayer.com/13/3898395/slides/slide_7.jpg " Measurement of lung function (FEV1, PEF) → Severity, response to treatment Laboratory and imaging studies selectively, (e.g., partial pressure of arterial carbon dioxide [PaCO 2 ]), complete blood count or a chest radiograph, electrocardiogram)")
16
All patients → a) supplementary oxygen to achieve an arterial oxygen saturation of 90% or greater b) inhaled short-acting β 2 - adrenergic agonists c) systemic corticosteroids
 supplementary oxygen to achieve an arterial oxygen saturation of 90% or greater b) inhaled short-acting β 2 - adrenergic agonists c) systemic corticosteroids")
18
Administered immediately on presentation Repeated up to three times within the first hour after presentation Use of a metered-dose inhaler with a valved holding chamber as effective as the use of a pressurized nebulizer in randomized trials Use of nebulizers for patients with severe exacerbations

19
Metered dose inhalers with holding chambers in mild to moderate exacerbations, Albuterol: four to eight puffs of albuterol can be administered every 20 minutes for up to 4 hours and then every 1 to 4 hours as needed Oral or parenteral administration of β 2 - adrenergic agonists is not recommended

20
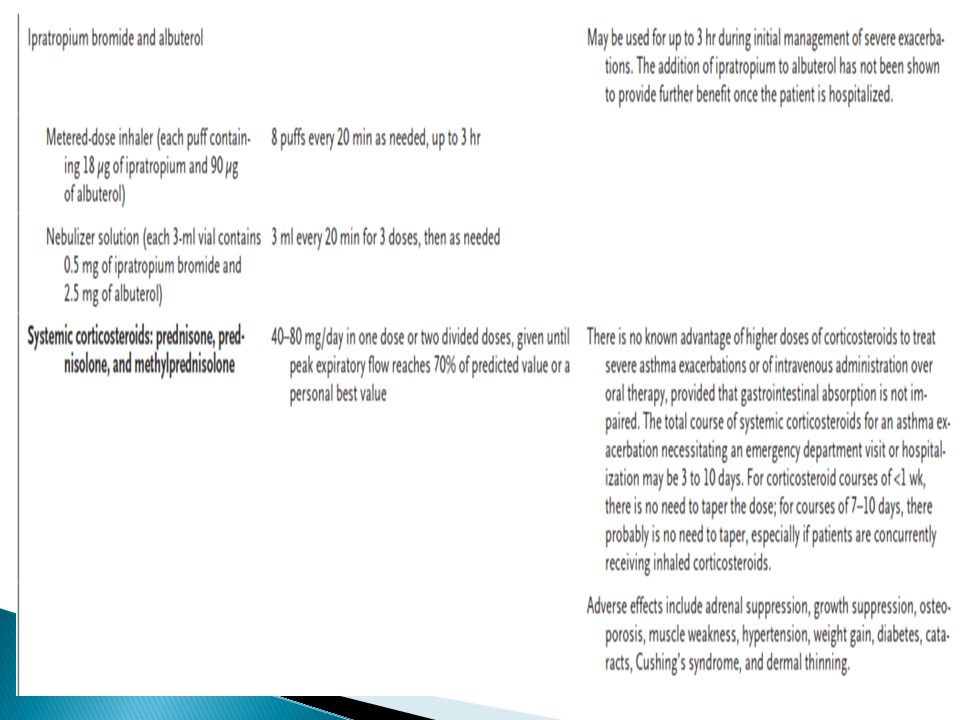
Slow onset of action, inhaled ipratropium Not recommended as monotherapy in the emergency department Added to a short acting β 2 -adrenergic agonist for a greater and longer lasting bronchodilator effect in exacerbations Reduces rates of hospitalization by approximately 25%

21
Needed in most patients with exacerbations that necessitate treatment in the emergency department More rapid improvement in lung function, fewer hospitalizations, and a lower rate of relapse after discharge from the emergency department No differences in the rate of improvement of lung function or in the length of the hospital stay between oral and parenteral steroid

22
Oral route is preferred for patients with normal mental status and without conditions expected to interfere with gastrointestinal absorption 40 to 80 mg per day in one dose or two divided doses

25
Not suitable as a substitute for systemic corticosteroids in the emergency department Preferred for long-term asthma control Addition at the time of discharge of inhaled steroid → reduction in the rate of relapse, as compared with oral corticosteroids alone

26
Methylxanthines: increasing the risk of adverse events without improving outcomes Antibiotics: except for bacterial infections (e.g., pneumonia or sinusitis) Aggressive hydration and mucolytic agents
 Aggressive hydration and mucolytic agents")
28
After the first treatment with an inhaled bronchodilator and again at 60 to 90 minutes (i.e., after three treatments) Survey of symptoms, a physical examination, and measurement of FEV 1 or PEF Measurement of ABG in most severe exacerbations Need for hospital admission as well as site of admission is better predicted by the assessment of asthma severity after 1 hour of treatment Admit or discharge according to subjective and objective improvement after one hour of initial treatment
 Survey of symptoms, a physical examination, and measurement of FEV 1 or PEF Measurement of ABG in most severe exacerbations Need for hospital admission as well as site of admission is better predicted by the assessment of asthma severity after 1 hour of treatment Admit or discharge according to subjective and objective improvement after one hour of initial treatment")
29
FEV 1 of less than 40% Persistent moderate to severe symptoms Drowsiness Confusion PaCO 2 of 42 mm Hg or greater FEV 1 of 40 to 69% and mild symptoms → assess individually for risk factors for death, ability to adhere to a prescribed regimen, and the presence of asthma triggers in the home

30
Immediate intubation and ventilatory support in patients with altered mental status, exhaustion, or hypercapnia Risk of hypotension and barotraumas during positive pressure ventilation due to high positive intrathoracic pressures Ventilation using permissive hypercapnia strategy → decreased mortality among patients with status asthmaticus

31
Intubation in a semi elective and controlled conditions (vs. performed as an emergency procedure by the first available staff) Noninvasive positive pressure ventilation: recommended for acute exacerbations of COPD but ?? for Asthma
 Noninvasive positive pressure ventilation: recommended for acute exacerbations of COPD but . for Asthma.")
32
FEV 1 or PEF after treatment is 70% or more of the personal best or predicted value Improvements in lung function and symptoms sustained for at least 60 minutes Use of short acting β 2 -adrenergic agonists inhalers as needed Oral corticosteroids for 3 to 10 days Corticosteroid inhaler to reduce the risk of relapse

34
Educate patients about medications, inhaler technique, and steps that can reduce exposure to household triggers of allergic reaction

35
Use of IV magnesium sulfate in severe exacerbations and also FEV 1 or PEF less than 40% of the personal best or predicted value after initial treatments Heliox: density about one third that of air, reduction of airflow resistance within and work of breathing and improvement in delivery of aerosolized medication Antileukoterines ??

39
N Engl J Med 2010;363:755-64 Emergency Treatment of Asthma. Stephen C. Lazarus, M.D NIH guidline

Similar presentations















>")

 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")














 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")

