Download presentation
Presentation is loading. Please wait.

1
Clinical Case Conference #5 Amaro - Aribon

2
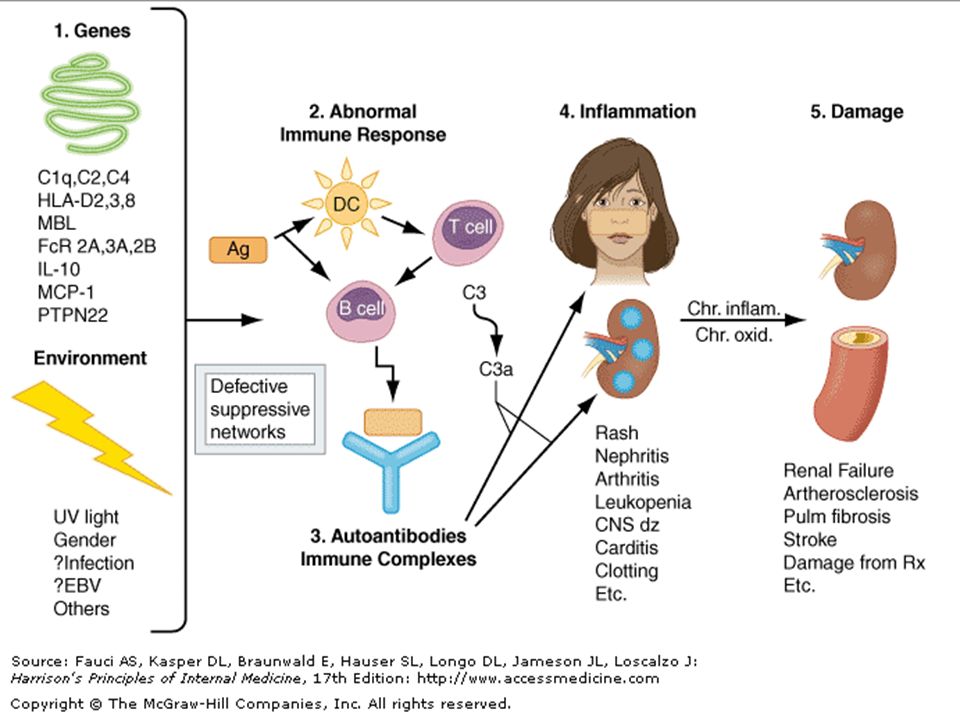
Pathomechanisms for Cytopenia in Active SLE

3
Cytopenia in SLE Most common hematologic manifestations of SLE: – Normochromic normocytic anemia due to autoimmune hemolysis, aplastic anemia, and pure red cell aplasia – Leukopenia (<4000/uL) which usually consists of Lymphopenia (<1500/uL) primarily due to a fall in absolute lymphocyte count – Thrombocytopenia (100,000/uL)
 which usually consists of Lymphopenia (<1500/uL) primarily due to a fall in absolute lymphocyte count – Thrombocytopenia (100,000/uL)")
5
Cytopenia in SLE Pathogenic auto-antibodies, and immune complexes bind to target tissues with activation of complement and phagocytic cells. Complement, and immune cells lead to release of chemotaxins, cytokines, chemokines, vasoactive peptides, and destructive enzymes.

6
Define Ferbrile Neutropenia

7
Febrile Neutropenia Refers to the clinical presentation of fever (one temperature ≥ 38.5 °C or three readings ≥38° C but ≤38.5 °C per 24 hrs) in a neutropenic patient with an uncontrolled neoplasm involving the bone marrow, or in a patient undergoing treatment with cytotoxic agents. Braunwald, et al. Harrison’s Principles of Internal Medicine 17 th ed.

8
Risk Factors for Candidiasis

9
Risk factors for Candidiasis General – Conditions causing a compromised host defense Neutropenia Glucocorticoid therapy Malnutrition Reference: http://www.harrisonspractice.com/practice /ub/view/Harrisons%20Practice/141100/0/ Candida

10
Risk factors for Candidiasis Oropharyngeal thrush – Diabetes mellitus – HIV infection Common in acute HIV infection Increasingly common late in disease as the CD4+ cell count falls – Dentures – Inhaled or oral glucocorticoids – Neonatal period – Iron deficiency Reference: http://www.harrisonspractice.com /practice/ub/view/Harrisons%20Pr actice/141100/0/Candida

11
Risk factors for Candidiasis Vulvovaginal candidiasis – Third trimester of pregnancy – Antibiotic use Reference: http://www.harrisonspractice.com/practice /ub/view/Harrisons%20Practice/141100/0/ Candida

12
Risk factors for Candidiasis Cutaneous candidiasis – Macerated skin Diapered area of infants Under pendulous breasts or pannus Hands constantly in water Hands covered by occlusive gloves Reference: http://www.harrisonspractice.com/practice /ub/view/Harrisons%20Practice/141100/0/ Candida

13
Risk factors for Candidiasis Esophageal candidiasis – HIV infection Uncommon until CD4+ counts fall below 50/μL Reference: http://www.harrisonspractice.com/practice /ub/view/Harrisons%20Practice/141100/0/ Candida

14
Risk factors for Candidiasis Invasive candidiasis – Use of broad-spectrum antibiotic therapy – Indwelling central venous catheter – Total parenteral nutrition – Perforation of the GI tract through trauma, surgery, or peptic ulceration – Mucosal damage due to cytotoxic agents used for cancer chemotherapy – Contamination of the hub or skin site of a catheter in an umbilical or central vein with secretions from the mouth, rectum, or vagina or with drainage from surgical wounds or tracheostomy sites – Intravenous drug abuse – Third-degree burns – Very low birth weight (in neonates) – Neutropenia – Glucocorticoid therapy Reference: http://www.harrisonspractice.com/practice /ub/view/Harrisons%20Practice/141100/0/ Candida
 – Neutropenia – Glucocorticoid therapy Reference: /ub/view/Harrisons%20Practice/141100/0/ Candida")
15
Antimicrobial treatment of systemic candidiasis

16
Disseminated candidiasis with end organ infection * after a demonstrated negative blood culture result or clinical signs of improvement.

17
Define sepsis and septic shock

18
Sepsis - is a serious medical condition that is characterized by a whole-body inflammatory state (called a systemic inflammatory response syndrome or SIRS) and the presence of a known or suspected infection.
 and the presence of a known or suspected infection.")
19
Septic Shock ● State of sepsis with refractory arterial hypotension or hypoperfusion abnormalities in spite of aggressive fluid resuscitation.(typically upwards of 6 liters or 40 ml/kg of crystalloid). ● Signs of systemic hypoperfusion may be either end- organ dysfunction or serum lactate greater than 4 mmol/dL.

Similar presentations


 that are needed to.>")










. Immune Deficiency Disorders Immunodeficiencies can be divided into primary immunodeficiency disorders, and secondary immunodeficiency.>")





