Download presentation
Presentation is loading. Please wait.

1
Dr Irfan Elahi Assistant Professor Nephrology 21-3-2016 (1hr) 12:30-1:30 pm
 12:30-1:30 pm")
4
Water 60% of Man’s body weight 50% of a woman’s body weight Distributed in to 1. Extracellular fluid compartment 35-45% (1/3) 2. Intracellular fluid compartment 55-65% (2/3)
 2. Intracellular fluid compartment 55-65% (2/3).")
6
The interstitial space ¾ of ECF 75% The intravascular space ¼ of ECF 25% Total body water diffuses freely between ICF & ECF in response to solute concentration gradient. Amount of water in different compartments depends entirely on the quantity of solute in that compartment.

7
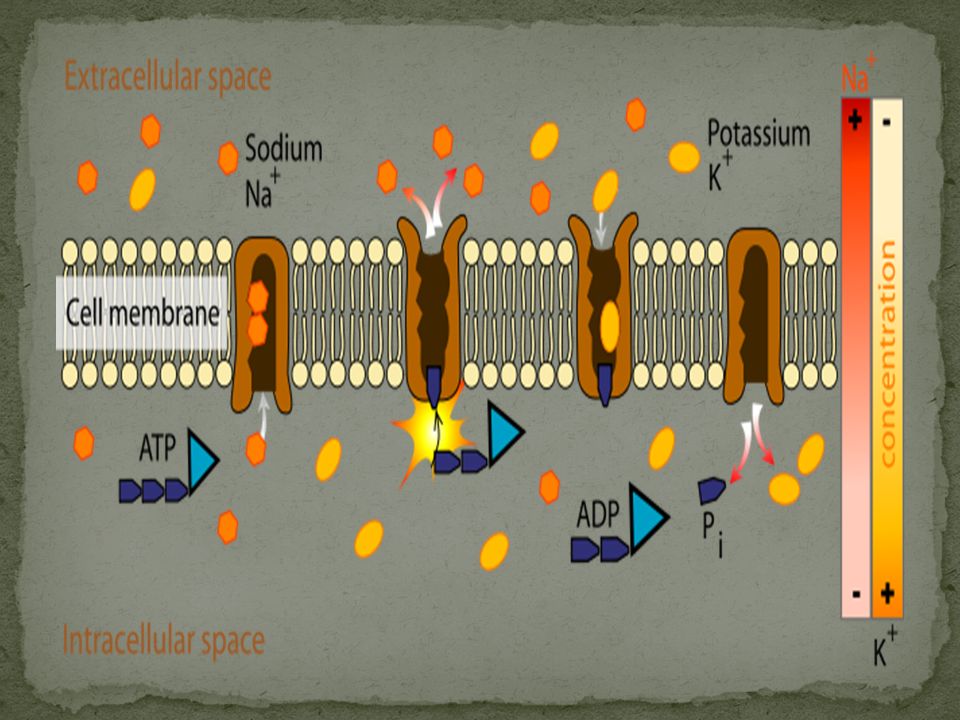
Major solute in the ECF is Sodium Major solute in the ICF is Potassium. This distribution is fulfilled by active transport through Na/K ATPase pump on the cell membrane. ECF is determined by the Na content of the body & mechanisms responsible for its maintenance.

11
Governed by Starling forces: 1. Capillary hydrostatic pressure 2. Colloid osmotic pressure 3. Interstitial hydrostatic pressure 4. Interstitial osmotic pressure Transcapillary hydrostatic pressure gradient exceeds the oncotic pressure gradient favors movement of plasma ultrafiltrate into extravascular compartment.

13
Adequacy of delivery of oxygen, nutrients, and other substances needed for organ function. Removal of waste products. This is done by maintaining ECF volume despite day to day variation in the in-take of sodium and water. ECF homeostasis is maintained by Afferent sensing limb and efferent effector limb.

14
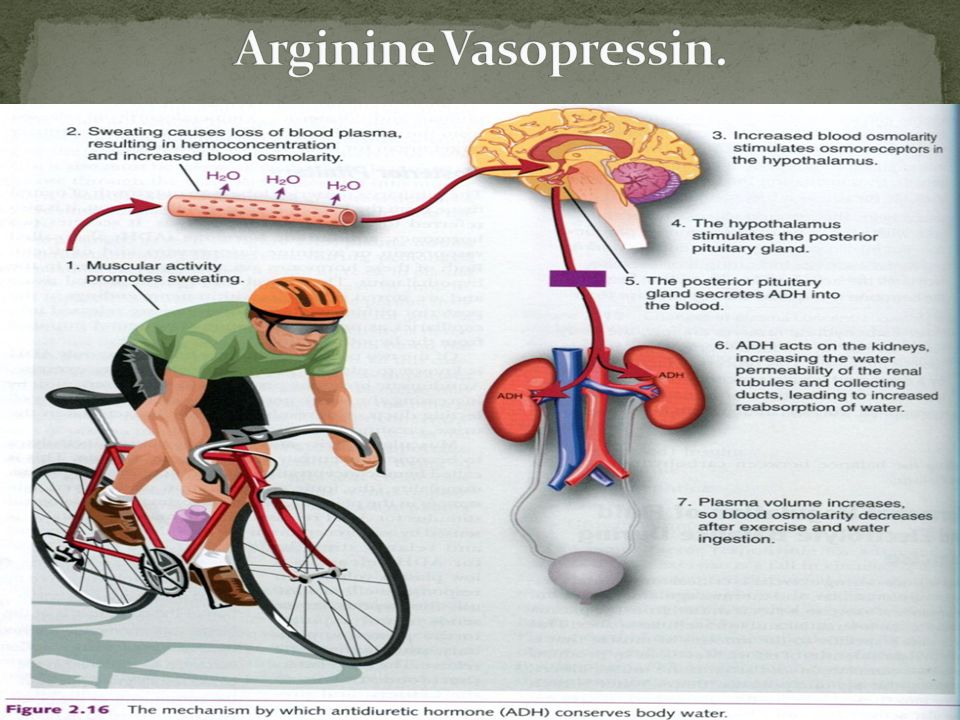
Afferent (Sensor) Limb Low-pressure cardiopulmonary receptors.(atrial, ventricular, & pulmonary) High-pressure arterial baroreceptors.(carotid, aortic arch, and renal) Osmoreceptors in hypothalamus Efferent (Effector) Limb Sympathetic Nervous sys RAAS Thirst Arginine vasopressin Natriuretic Peptides
 Limb Low-pressure cardiopulmonary receptors.(atrial, ventricular, & pulmonary) High-pressure arterial baroreceptors.(carotid, aortic arch, and renal) Osmoreceptors in hypothalamus Efferent (Effector) Limb Sympathetic Nervous sys RAAS Thirst Arginine vasopressin Natriuretic Peptides")
15
An increase in left atrial pressure suppresses release of ADH. Atrial distension and sodium load causes release of Atrial natriuretic peptide.ANP BNP brain natriuretic peptide is stored in ventricular myocardium, released when ventricular diastolic pressure rises. These all mechanisms enhance renal salt and water excretion.

16
Arterial stretch receptors in carotid artery, aortic arch and glomerular afferent arteriole respond to a decrease in arterial pressure. Nerve impulses are carried by vagal & glossopharyngeal nerves to vasomotor centers in medulla and brainstem. Normal impulses exert a tonic inhibitory effect on sympathetic outflow and increase parasympathetic activity. Also influence ADH and RAAS systems

17
Sympathetic Nervous System. Renin-Angiotensin-Aldosterone System. Thirst Arginine Vasopressin. Natriuretic Peptides.

26
Expansion of ECF refers to accumulation of fluid in ECF due to salt and fluid retention by kidneys. Generalize Edema results from increase in interstitial fluid volume. Causes are: Cardiac failure Cirrhosis with ascites Nephrotic Syndrome

27
Capillary hemodynamic Disturbances Exchange of fluid between plasma and interstitium is determined by the hydrostatic and oncotic pressures in each compartment Edema results from Decrease in plasma oncotic pressure. Increase in capillary hydrostatic pressure. Decrease rate of removal by lymphatics

29
Insensitive to alteration in arterial pressure. This pressure is result of variation in the precapillary sphincter, which controls amount of pressure transmitted to capillary bed by autoregulation. Impaired by Calcium channel blockers (Amlodipine)
.")
30
The venous end is not regulated by sphincter so edema results in volume expansion in renal failure and CCF. Venous obstruction in Cirrhosis of liver causes ascites and sudden acute pulmonary edema after sudden impairment in cardic function (MI).
..")
31
Hepatic cirrhosis (decreased production of albumin) Nephrotic syndrome (increase loss of albumin)
 Nephrotic syndrome (increase loss of albumin)")
32
Primary Sodium Retension due to reduced GFR Acute renal failure Chronic renal failure Glomerulonephritis Secondary Renal Retention Cardic failure Cirrhosis Nephrotic Syndrome Drug induced edema Pregnancy

33
85% of blood circulates on the low pressure venous side of circulation. 15% of blood circulates in the high-pressure arterial circulation.

34
Increase in total body water due to under-filling 0f arterial circulation even when venous circulation is over-loaded. Cardiac failure causes under-filling of arterial circulation Early cirrhosis results in decreased systemic vascular resistance in splanchnic circulation

Similar presentations

























 intracellular. (1/3)extracellular (interstitial fluid) 5% blood plasma. edema = an accumulation of interstitial.>")








. Other excretory.>")




