Download presentation
Presentation is loading. Please wait.

1
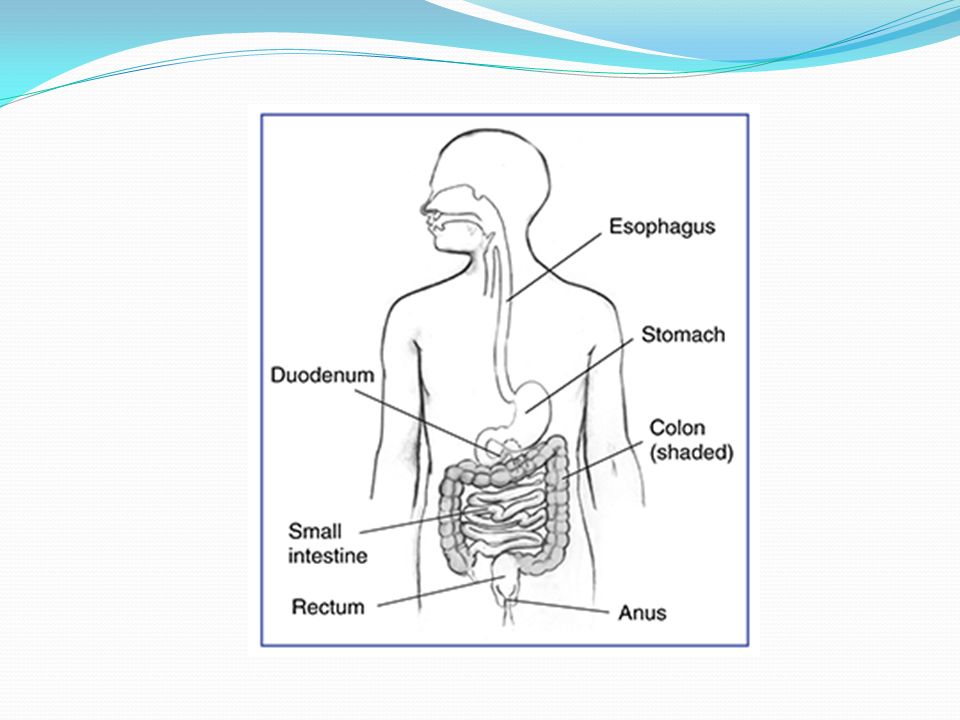
Abdominal Sonography I Lecture 8 Gastrointestinal Tract
HHoldorf

3
Outline Bowel Wall Gastro esophageal Junction Acute Appendicitis
Hypertrophic Pyloric Stenosis Laboratory values Diverticulitis Bowel Obstruction Duodenal Atresia Intussusception

4
Bowel Wall The normal intestinal wall is between 3 and 5 mm thick, depending on distention of the bowel. Five sonographic interfaces can be seen when imaging the intestinal wall. Intestinal pathology creates a sonographic pattern known as the TARGET or PSEUDOKIDNEY sign. This appears as a hypoechoic external rim corresponding to thickened intestinal wall and a hyperechoic center relating to a residual gut lumen or mucosal ulceration. . Be able to identify an image of the pseudokidney sign

6
Normal Bowel wall

7
The wall is divided into four layers as follows:
Mucosa : The innermost layer of the digestive tract Submucosa Muscularis externa Serosa/mesentery The outer layer of the gut is formed by fat and another layer of epithelial cells called mesothelium.

8
Causes of Wall Thickening of the Small Bowel
Wall edema Malignancy Postoperative Lymphoma Cirrhosis/ascites Peritoneal carcinomatosis Hypoproteinemia

9
Causes of Wall Thickening of the Small Bowel
Inflammatory bowel disease Crohn’s disease Acute ileitis Extraintestinal inflammatory conditions Pancreatitis Endometriosis Homework: Define Crohn’s Disease

10
Causes of Wall Thickening of the Small Bowel
Mesenteric ischemia/infarction Thrombosis of mesenteric veins Thrombosis of mesenteric arteries Small bowel disease/malabsorption Celiac disease Whipple’s disease : Define Whipple’s Disease for homework Benign intestinal tumors adenoma, lipoma

11
Benign Gastric Wall Thickening
Benign Gastric Wall Thickening. The wall of the gastric antrum (arrow) as seen in short axis view is diffusely and symmetrically thickened by adjacent acute pancreatitis
 as seen in short axis view is diffusely and symmetrically thickened by adjacent acute pancreatitis.")
12
Pseudokidney sign

13
Gastro esophageal junction
The segment of esophagus between the diaphragm and the stomach is called the gastroesophageal junction. On a longitudinal midline view of the epigastrum, this is seen as a target sign posterior to the left lobe of the liver. Be able to recognize an image of the Gastroesophageal Junction (GE junction)
")
15
Gastroesophageal Junction (GE junction)
")
16
Acute Appendicitis Acute appendicitis is the most common cause of an acutely painful abdomen. Patients present with Peri-umbilical pain shifting to RLQ Leukocytosis (increased WBC count) Nausea, vomiting, and low-grade fever Rebound tenderness
 Nausea, vomiting, and low-grade fever. Rebound tenderness.")
17
McBurney’s point The right lower quadrant location of the most tender area in the early stages of appendicitis.

18
Appendicitis is caused by the obstruction of the appendiceal lumen by a fecalith or hyperplasia of the submucosa. Mucosal secretions increase the intraluminal pressure and compromise venous and lymphatic drainage. Bacterial infection leads to gangrene and perforation. Perforation leads to peritonitis.

19
Graded –compression ultrasound is utilized to displace bowel gas and decrease the distance between the transducer and the appendix. Sonographic criteria for diagnosing an inflammatory appendix includes Non-compressible appendix > 6 mm diameter Appendicolith (fecalith) NOTE: Do not be afraid to push the gas away. In female patients of child-bearing age, right lower quadrant pain may be due to pathology of the appendix or gynecologic structures.
 NOTE: Do not be afraid to push the gas away. In female patients of child-bearing age, right lower quadrant pain may be due to pathology of the appendix or gynecologic structures.")
20
Color flow hyperemia can be observed with an inflamed appendix.
Be able to identify several images/examples of acute appendicitis.

22
Normal Appendix

23
Abnormal Appendix: Thickened appendix secondary to Crohns’s disease.

24
Hypertrophic Pyloric Stenosis
Hypertrophic pyloric stenosis (HPS or sometimes referred to as IHPS) has a 4 to 1 male to female ratio. Characterized by hypertrophy of the circular muscle resulting in elongation of the pylorus and constriction of the canal.
 has a 4 to 1 male to female ratio. Characterized by hypertrophy of the circular muscle resulting in elongation of the pylorus and constriction of the canal.")
26
The neonatal (3-6 weeks of age) patient presents with
Projective vomiting Palpable olive-shaped abdominal mass Ultrasound is the method of choice for diagnosing HPS. The diagnostic criteria includes Pyloric muscle thickness >3mm Pyloric channel length >12 mm Pyloric cross section >15 mm With hypertrophic pyloric stenosis, there is an increase in the pyloric diameter and length.

27
Identify images of a hypertrophic pyloric stenosis with muscle thickness measured, channel length measured, and cross section measured.

28
IHPS

29
IHPS : Radiology string sign

30
IHPS

31
Laboratory values Carcinoembryoinic antigen (CEA)
Increased levels are found in patients with colon carcinoma. Although it is not specific for colon cancer, it is also associated with cirrhosis, ulcerative colitis, and other cancers.

32
Diverticulitis Diverticulitis is the inflammation of diverticulum (Colonic outpouchings). Diverticulum commonly involve the sigmoid colon. Symptoms of diverticulitis include Fever Leukocytosis Left lower quadrant pain

34
Sonographic findings include:
Thickening of the bowel wall (> 4mm) Abscess formation Inflamed diverticula (round echogenic structures Be able to identify an image of diverticulitis
 Abscess formation. Inflamed diverticula (round echogenic structures. Be able to identify an image of diverticulitis.")
35
Diverticulitis of the Sigmoid colon

36
Bowel Obstruction Mechanical small-bowel obstruction (SBO) can be caused by Intraluminal (food bolus) Bowel wall lesion (tumor, Crohn disease) Extrinsic (adhesions, hernia)-most common Prolonged bowel obstruction can result in Bowel ischemia Bowel necrosis Septicemia Perforation Peritonitis
 Extrinsic (adhesions, hernia)-most common. Prolonged bowel obstruction can result in. Bowel ischemia. Bowel necrosis. Septicemia. Perforation. Peritonitis.")
38
Symptoms include Abdominal distention Paint Vomiting Hypotension (caused by fluid depletion) Leukocytosis Ultrasound is used to demonstrate loops of distended bowel, level of obstruction, and peristalsis Identify images of Bowel obstruction in the small bowel and the large colon.

39
Bowel Obstruction

40
Duodenal Atresia Duodenal atresia presents in newborns with the onset of vomiting within hours of birth. Once delivered, epigastric fullness form dilatation of the stomach and proximal duodenum is noted. Duodenal atresia may be discovered during a prenatal ultrasound. The ultrasound evaluation will demonstrate: Polyhydramnios Fluid-filled stomach Fluid-filled proximal duodenum This is referred to as the double bubble sign Identify an image of the double bubble sign

43
Duodenal Atresia

44
Intussusception Intussusception is a process in which a segment of intestine invaginates into the adjoining intestinal lumen (telescoping), causing a bowel obstruction. This is the most common cause of obstruction in infants and typically occurs less than one year of age.
, causing a bowel obstruction. This is the most common cause of obstruction in infants and typically occurs less than one year of age.")
46
Classic symptoms of Intussusception include
Vomiting Abdominal pain Rectal bleeding Although difficult to detect, a physical finding of a sausage-shaped mass in the right hypochondrium is a classic sign of an Intussusception. Sonographically, Intussusception usually presents as an oval, pseudokidney-appearing mass. On a transverse view, concentric rings of folded bowel are typically seen. Identify images of Intussusception on transverse views.

47
Intussusception: Target Sign

48
This one has a Think Tank
Next week Think Tank Time!!!!!

Similar presentations