Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
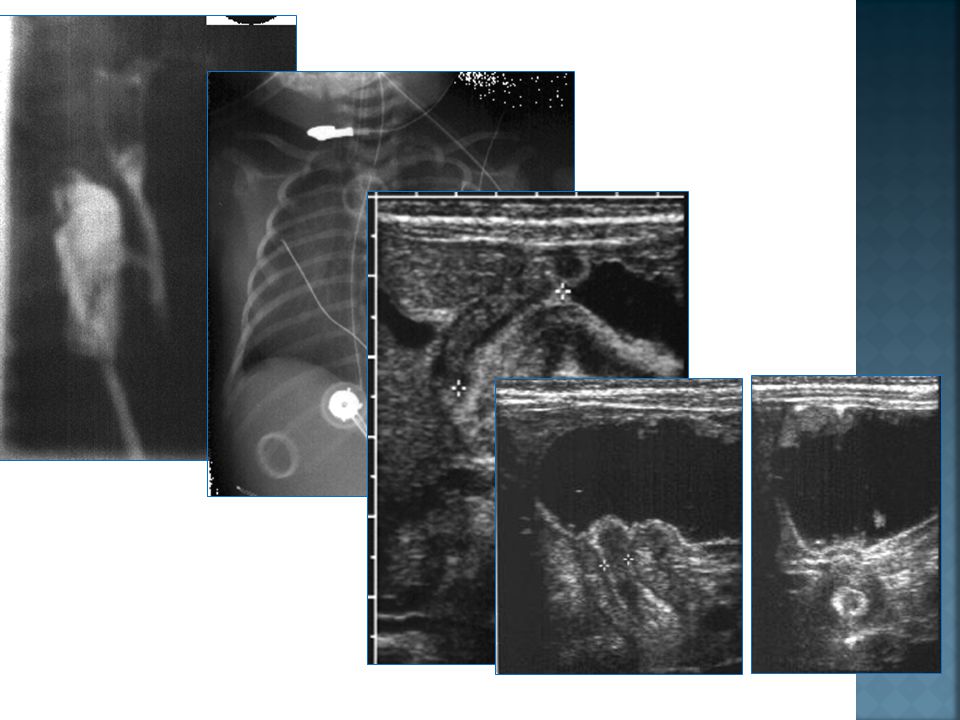
Case 1 Clinical History: 3 month-old male presented with recurrent pneumonia. Mother reported coughing and choking during feeding. Barium swallow was requested searching for????

3
A babygram demonstrates a feeding tube at the level of the thoracic inlet. In addition, there is complete lack of gas in the abdomen.

4
Diagnosis: Proximal tracheal esophageal fistula.
Esophogram and a G-tube study injection of esophageal pouch from above reveals proximal tracheal esophageal fistula at level of thoracic inlet with aspiration of a small amount of barium. Diagnosis: Proximal tracheal esophageal fistula.

5
Discussion The entity is secondary to incomplete division of the primitive foregut. Various types of abnormal division are present.

6
radiographically Inability to pass a feeding tube into the stomach (esophageal atresia). Gasless abdomen in those patients with esophageal atresia and proximal TE fistula. Aspiration pneumonia. Associated anomalies seen in from 17-70% of individuals, encompass cardiac, musculoskeletal (vertebral, radial ray anomalies), gastrointestinal, genitourinary, and chromosomal (trisomy18, 21, and 13).
, gastrointestinal, genitourinary, and chromosomal (trisomy18, 21, and 13).")
7
Complications after repair include:
Anastomotic leak. Recurrent TE fistulal aspiration pneumonia secondary to esophageal stricture. Disordered esophageal motility. Gastro- esophageal reflux.

8
Case 2 Clinical History: Full-term two day old female with dyspnea and cyanosis. Chest X-ray was requested.

9
Diagnosis: Congenital Diaphragmatic Hernia
On the first study there is increased opacity of the left hemithorax with areas of lucency. The left hemidiaphragm is obliterated. The mediastinal structures are shifted to the right.absence of bowel gas within the abdomen. . The next study done several hours later shows a large well- defined area of lucency in the left hemithorax representing swallowed air within the abdominal viscera. Diagnosis: Congenital Diaphragmatic Hernia

10
Discussion 1: 2,500 live births,2 : 1 male to female ratio, bilateral 3%. Types: Bochdalek hernia, posterior lateral segments of the diaphragm, 75% left. Morgagni hernia, 2 to 4% of all CDH. Herniation of abdominal viscera occurs through a defect in the diaphragm caused by failure of the pleural peritoneal canal to close completely during embryonic development. Varying degrees of herniation can occur. These patients will often have hypoplastic lungs due to crowding of the thoracic space.

11
Associated anomalies:
Malrotation in 95% of affected children secondary to interruption of the normal rotation that occurs as the bowel returns to the abdomen. Neural tube defects (30%). Cardiovascular lesions (20%) VSD and TOF. Symptoms: Severe respiratory distress at birth e.g. dyspnea and cyanosis (hypoplastic lungs). Acute intestinal obstruction can also occur. Diagnosis: Is usually made by radiographic examination. Differential diagnosis: Cystic adenomatoid malformations of the lung.
. Cardiovascular lesions (20%) VSD and TOF. Symptoms: Severe respiratory distress at birth e.g. dyspnea and cyanosis (hypoplastic lungs). Acute intestinal obstruction can also occur. Diagnosis: Is usually made by radiographic examination. Differential diagnosis: Cystic adenomatoid malformations of the lung.")
12
Complications: Pulmonary hypertension often complicates the pre- and postoperative course. In most centers, overall mortality rate remains about 50%. Treatment: Respiratory support as well as surgical repair of the diaphragmatic defect. Nasogastric intubation with suction will decrease air and fluid within the abdominal viscera decreasing ventilatory compromise. Extracorporal membrane oxygenation (ECMO) may improve prognosis although mortality rate remains about 50%.
 may improve prognosis although mortality rate remains about 50%.")
13
Case 3 Clinical History: Four week-old infant presented with post-prandial vomiting and failure to thrive. Abdominal US was requested.

14
CHPS (congenital hypertrophic pyloric stenosis)
Longitudinal ultrasonographic images pyloric muscle thickness of 4 mm, and pyloric channel length of 17 mm. CHPS (congenital hypertrophic pyloric stenosis)
")
15
discussion Diagnosis:
Clinical. In an infant who presents with non-bilious, post-prandial vomiting, failure to thrive, and a palpable mass ("olive") in the epigastric region, hypertrophic pyloric stenosis is a presumptive diagnosis. The etiology: Unknown, ?? prolonged spasm muscular hypertrophy. Demographic factors: Age at presentation: majority between 2-6 weeks. Sex predilection: males > females. Race predilection: uncommon in blacks. Inheritance pattern: dominant polygenic . The value of imaging studies is in any doubt as to the diagnosis.
 in the epigastric region, hypertrophic pyloric stenosis is a presumptive diagnosis. The etiology: Unknown, prolonged spasm muscular hypertrophy. Demographic factors: Age at presentation: majority between 2-6 weeks. Sex predilection: males > females. Race predilection: uncommon in blacks. Inheritance pattern: dominant polygenic . The value of imaging studies is in any doubt as to the diagnosis.")
16
US findings Ultrasound is the imaging modality-of-choice:
(longitudinal images) necessary for diagnosis are as follows: Pyloric muscle thickness: > 4 mm Pyloric channel length: > 17 mm Pyloric muscle length: > 19 mm Little fluid entering the duodenum If the pyloric canal length is less than 18mm, then the diagnosis of HPS should be in doubt. Treatment: pyloromyotomy is the preferred mode of therapy, and in most cases is successful.
 necessary for diagnosis are as follows: Pyloric muscle thickness: > 4 mm. Pyloric channel length: > 17 mm. Pyloric muscle length: > 19 mm. Little fluid entering the duodenum. If the pyloric canal length is less than 18mm, then the diagnosis of HPS should be in doubt. Treatment: pyloromyotomy is the preferred mode of therapy, and in most cases is successful.")
17
Case 4 Clinical History:
10-year-old boy with crampy abdominal pain and fever. US was requested.

18
Diagnosis: Acute appendicitis.
Findings: Enlarged (diameter = 9 mm) noncompressible, hyperemic appendix with periappendiceal fluid as well as fluid within the pouch of Douglas.
 noncompressible, hyperemic appendix with periappendiceal fluid as well as fluid within the pouch of Douglas.")
19
Discussion: Acute appendicitis is the most common indication for emergency laparotomy in children. Perforation occurs with a much greater frequency (approximately 25%) in the pediatric population. The pathogenesis generally begins with luminal obstruction distention venous compromise arterial compromise perforation periappendiceal abscess.
 in the pediatric population. The pathogenesis generally begins with luminal obstruction distention venous compromise arterial compromise perforation periappendiceal abscess.")
20
Clinical picture: The usual initial symptoms are vague visceral abdominal pain secondary to the distention of the appendix. After 4 to 6 hours, as the inflammation spreads to the parietal peritoneum, the pain increases in intensity and becomes somatic in nature localized at "McBurney's Point" in the RLQ. Nausea, vomiting, and anorexia are frequently associated. The typical historical and physical findings are found in approximately 2/3 of patients eventually determined to have appendicitis. The clinical diagnosis is not always entirely straightforward especially in children who may not be able to communicate their symptoms adequately. Imaging methods must be used in patients with indeterminate clinical findings to avoid unnecessary laparotomies.

21
Ultrasound is the current diagnostic modality of choice.
A cross-sectional diameter measurement > 6 mm along with noncompressibility in a patient with persistent RLQ pain is considered reliable evidence of appendicitis. Associated findings include: loss of the echogenic submucosal layer. fluid-filled lumen which will be anechoic. hyperechoic appendicolith with acoustic shadowing. +/- periappendiceal fluid collections or mass which may displace adjacent structures. These latter findings are more likely to be seen in association with perforation.

23
Thank you Dr/ Naglaa M Elsayed

Similar presentations












 Department of Pediatrics>")





 Dr JACOB MATHEW DEPT. OF PAED. SURGERY Dr AHMED ABANAMY HOSPITAL.>")
