Download presentation
Presentation is loading. Please wait.

1
Veterinary Specialists Of South Florida Presents…

2
Medial Patellar Luxation
VETERINARY SPECIALISTS OF SOUTH FLORIDA Dr. Kelly Alford

3
“Penny” Signalment 6 yo FS Yorkie Presenting Complaint
Weight bearing lameness on the RH limb History No trauma Other dogs in home Non-painful Otherwise healthy Penny, a 6 yo FS Yorkie, presented on emergency for a partial weight bearing lameness on the R hind limb. No traumatic event was witnessed by the owners, however there are other dogs in the house. Penny didn’t seem overtly painful at home. No history of other medical problems, no current medications. On a diet of lamb and rice, UTD on vaccines. Otherwise healthy.

4
Physical Examination BAR, mm = p/m, CRT < 2 sec’s Vital signs wnl
H/L auscultation wnl MPL Grade I on the left stifle Grade IV on the right stifle Partial or full tear of the CCL in the right stifle Rest of PE unremarkable On presentation, Penny was BAR, mucous membranes were moist and pink with a CRT of less than 2 sec’s. Vital signs were within normal limits as was heart/lung auscultation. A medial luxating patella was found bilaterally, with the left stifle having a Grade I and the right stifle having a Grade IV. In the right stifle, a partial or full tear of the CCL ligament was also suspected, a small amt of drawer was elicited on palpation. The remainder of her physical examination was unremarkable. At this time, it was recommended that Penny have a tibial transposition and an extracapsular and wedge resection.

5
Treatment Penny presented 8 days later for surgery PE – unchanged
Blood work: CBC/Chemistry Unremarkable

6
Surgery Surgery Post – Op Arthrotomy Imbrication of the joint capsule
Partial CCLR Medial meniscal release Imbrication of the joint capsule Lateral suture Imbrication of the lateral retinaculum Post – Op Home on Tramadol, Rimadyl and Simplicef Strict cage rest A craniomedial approach was made to the stifle and proximal tibia and the articular surface of the trochlear groove was exposed. The joint was explored and a partial CCLR was found. A medial meniscal release was performed. The joint capsule was imbricated with simple interrupted sutures. A lateral suture was placed around the lateral fabella and the tibial tuberosity. The lateral retinaculum was imbricated. Penny did well post op and sent home on Tramadol, Rimadyl, Simplicef and a bandage.

7
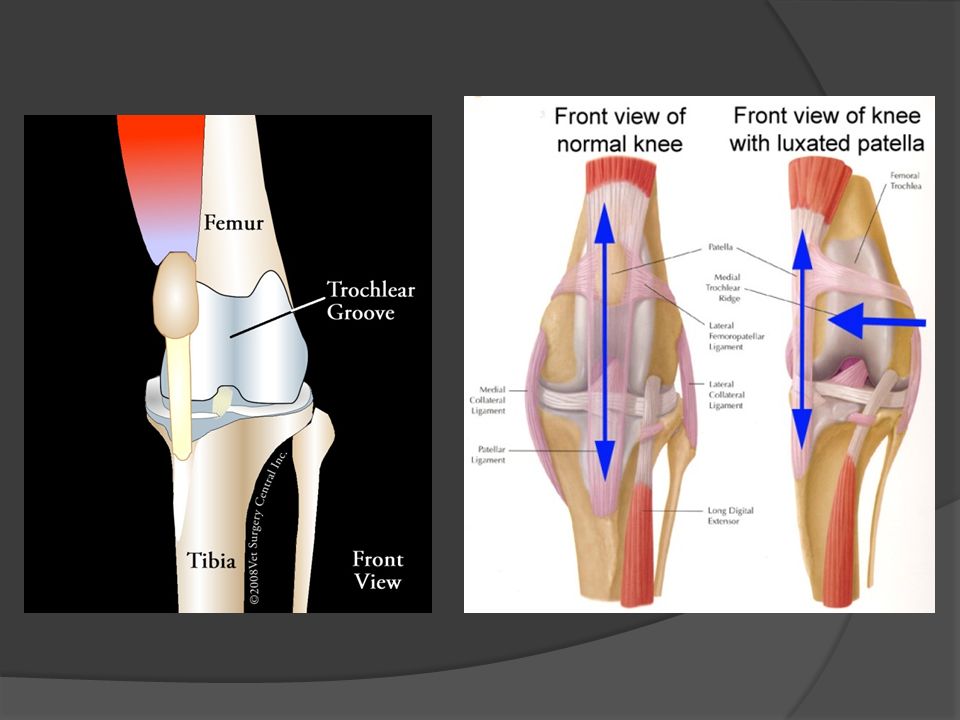
Patellar Luxation Femoropatellar instability
Leads to displacement of the patella from the trochlear groove Medial, lateral or proximal >75% cases are medial (small & large dogs) 50% bilateral Patellar luxation is one of the most common causes of lameness in dogs. It occurs when there is femorapatellar instability leading to displacement of the patella from its normal anatomic position in the femoral trochlear groove. The displacement can be medial, lateral or proximal. Greater that 75% of dogs have a medial luxation, and this includes small and large dogs. Lateral luxation occurs mostly in large dogs. Approximately half of affected dogs have bilateral involvement.
 50% bilateral. Patellar luxation is one of the most common causes of lameness in dogs. It occurs when there is femorapatellar instability leading to displacement of the patella from its normal anatomic position in the femoral trochlear groove. The displacement can be medial, lateral or proximal. Greater that 75% of dogs have a medial luxation, and this includes small and large dogs. Lateral luxation occurs mostly in large dogs. Approximately half of affected dogs have bilateral involvement.")
8
Pathophysiology Associated musculoskeletal abnormalities:
Medial displacement of the quadriceps muscle group Lateral torsion of the distal femur Lateral bowing of the distal 1/3 of the femur Femoral epiphyseal dysplasia Rotational instability of the stifle joint Tibial deformity Most patients with patellar luxation have associated musculoskeletal abnormalities, such as medial displacement of the quadriceps muscle group, lateral torsion of the distal femur, a lateral bowing of the distal one third of the femur, femoral epiphyseal dysplasia, rotational instability of the stifle joint, or tibial deformity.

10
Pathophysiology Medial malalignment of the quadriceps muscles
Retards distal femoral physis growth Less pressure on the lateral aspect allows accelerated growth Lateral bowing of the distal femur Abnormal growth while the physes are active Tibial deformities Medial displacement of the tibial tuberosity, medial bowing of the proximal tibia, lateral torsion of the distal tibia Medial malalignment of the quadriceps muscles in dogs with medial patellar luxation produces sufficient pressure on the distal femoral physis to retard growth. At the same time, there is less pressure on the lateral aspect of the distal femoral physis, which allows accelerated growth. Decreased length of the medial cortex relative to the increased length of the lateral cortex results in the lateral bowing of the distal femur. Abnormal growth continues as long as the quadriceps is displaced medially and the physes are active. Therefore the degree of lateral bowing depends on the severity of patellar luxation and the patient’s age at the onset of luxation. Tibial deformities are the result of abnormal forces acting on the proximal and distal physes of the tibia. These deformities seen with medial luxation include medial displacement of the tibial tuberosity, medial bowing of the proximal tibia and lateral torsion of the distal tibia.

11
Articular Cartilage Responds to change in pressure
Increased pressure: retards growth Decreased pressure: accelerates growth Abnormal trochlear groove Near normal to absent Patella produces a physiologic pressure on the articular cartilage that retards cartilage growth Continued pressure from the patella is responsible for the development of the normal depth of the trochlear groove If no pressure is exerted, the trochlea fails to gain proper depth Articular cartilage responds to increased or decreased pressure in the same manner as the physis. Increased pressure retards growth and decreased pressure accelerates growth. Dogs with MPL have abnormal development of the trochlear groove. The degree varies from a near-normal trochlea to an absent trochlear groove. Articulation of the patella within the groove exerts a physiologic pressure on the articular cartilage that retards cartilage growth. Continued pressure by the patella is responsible for the development of normal depth of the trochlear groove. If the physiologic pressure exerted isn’t present, then the trochlea fails to gain proper depth.

12
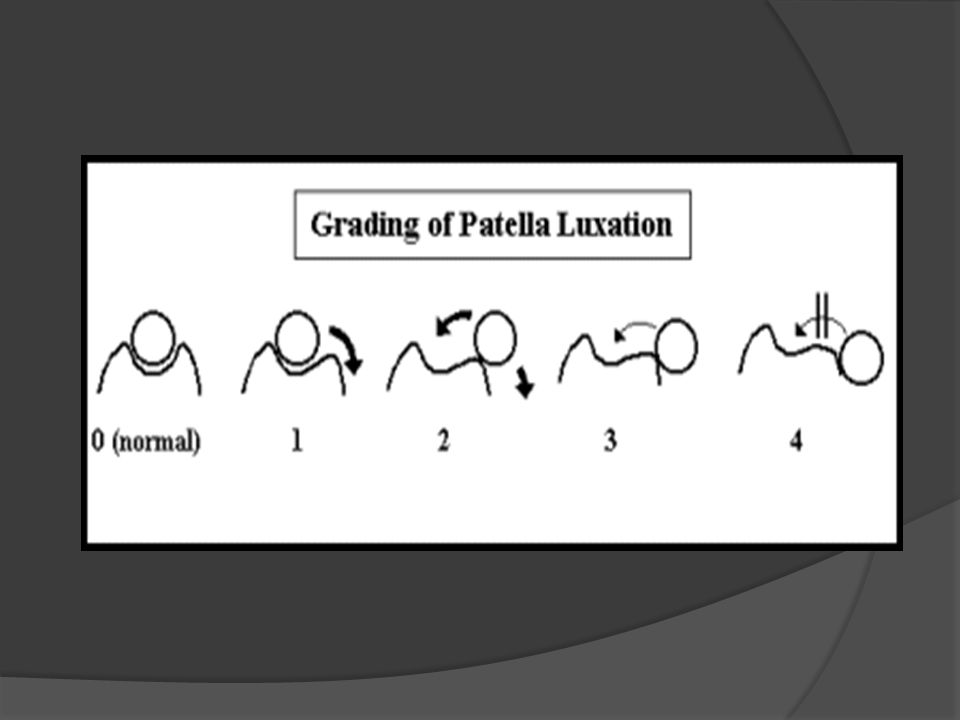
Grading System Severity classified into grades:
I: patella manually luxated when stifle is in extension, spontaneous luxation rare II: intermittent luxation with a non-painful, “skipping” lameness III: permanent luxation that can be reduced manually IV: permanent, non-reducible luxation The degree of the pathologic skeletal condition seen with patellar luxation varies considerably between the mildest and severest forms. A system for classifying the patellar luxation has been developed. In grade I, the patella can be luxated with the stifle held in full extension. The patella reduces when pressure is released. There is no crepitation or bony deformity. Spontaneous luxation is rare and clinical signs are absent or occur infrequently. Grade II luxation occurs when spontaneous luxation of the patella occurs with clinical signs of a non-painful, “skipping” type of lameness. Angular and torsional deformities of the femur may be present to a mild degree. May progress to a grade 3. Grade 3 is characterized by a patella that remains luxated most of the time, but may be manually reduced when the stifle is in extension. However, with flexion and extension of the stifle, the patella luxates again. There is medial displacement of the quadriceps muscle group. Abnormalities of the supporting soft tissue of the stifle joint and deformities of the femur and tibia may be present. The patient is also described as having a “crouched” gait b/c the dog often uses the leg in a semiflexed, internally rotated position. This condition is often bilateral. Grade IV is the most severe and occurs when there is permanent, nonreducible luxation of the patella. The tibia is rotated from 60 to 90 degrees relative to the sagittal plane and the trochlear groove is shallow to absent. There is also medial displacement of the quadriceps group. If not corrected early, there is severe bony and ligamentous deformities that develop and often aren’t repairable.

14
Signalment Dogs >>> cats Toy and miniature dog breeds
Higher incidence: Miniature and toy poodles, Yorkshire terriers, Pomeranians, Pekingese, Chihuahuas and Boston terriers Age – generally after 4 months of age Females 1.5: 1 over males This disease occurs mostly in dogs, rarely in cats. It is most common in toy and miniature breeds of dogs, specifically miniature and toy poodles, yorkies, pomeranians, pekingese, chihuahuas and boston terriers. Though clinical signs can be seen shortly after birth, affected dogs are usually greater than 4 months of age. Females also tend to be 1 and a half times more likely to be affected than males.

15
Clinical Presentation
History Intermittent weight-bearing lameness Holds leg up – flexed position Grade IV – severe lameness & gait abnormalities PE Findings Vary depending on severity Laboratory Findings Non specific Dogs with an MPL usually present with an intermittent weight-bearing lameness. They may be seen holding the leg in a flexed position for a few steps. Dogs with more severe luxation's display severe gait abnormalities and lameness. The diagnosis of an MPL is based on finding or eliciting MPL during a PE. Findings can vary depending on the severity of luxation. For example, dogs with a Grade I may be diagnosed as an incidental finding on PE. Whereas more severely affected dogs can be found to have medially displaced patella's alongside the femoral condyle. Lab findings are usually non-specific and no consistent lab findings are seen with this disease. Arthrocentesis demonstrates changes associated with osteoarthritis

16
Diagnostics Radiographs Grade I-II Grade III-IV
May show the patella within the trochlear sulcus or displaced medially Grade III-IV Show the patella displaced medially Full limb radiographs may show varus or valgus deformities and torsion of the tibia and femur Radiographic appearance can vary depending on the Grade. I-II may show the patella within the trochlear groove or displaced medially. Proper positioning of the limb is important to eliminate artifactual appearing luxation's. Grade III-IV luxation's typically show a medially displaced patella. Full limb radiographs may help to assess varus or valgus deformities and torsion of the tibia and femur. For more severe cases requiring long bone osteotomy and correction, special views such as skyline views, of the femur or CT aid in determining the specific type and degree of deformity.

18
Differential Diagnosis
CCLR Concurrent in 15-20% of cases Avulsion of the tibial tubercle Hip luxation/FHO Shortens limb d/t laxity of quadriceps mechanism Rupture of the patellar tendon Avascular necrosis of the femoral head Malunion & malalignment of fractures of femur or tibia May result in displacement of the quadriceps muscle group

19
Treatment Conservative management Surgical management Older
Asymptomatic Surgical management Young Lame Active growth plates Patients can be treated conservatively or surgically. The TOC depends on the clinical history, PE findings, frequency of luxation and the patient’s age. Surgery is usually not pursued in asymptomatic older patients. Those that benefit from surgery are the younger patient’s that display lameness. Intermittent patellar luxation in these animals can cause premature wear of the articular cartilage of the patella. Surgery is indicated at any age in patients that are lame, and strongly advised in those with active growth plates because skeletal deformity can worsen rapidly. Patient’s with bilateral severe luxation's may require multiple surgeries and probable continued lameness b/c of the severity of the underlying long bone abnormalities.

20
Surgery Numerous techniques described:
Tibial tuberosity transposition Medial restraint release Lateral restraint reinforcement Trochlear groove deepening Femoral osteotomy Tibial osteotomy Antirotational sutures Transposition of the origin of the rectus femoris Combination of techniques most effective Soft tissue and orthopedic Primary abnormality is biomechanical Numerous techniques have been described to aim to restrain the patella within the trochlear groove. These include tibial tuberosity transposition, medial restraint release, lateral restraint reinforcement, trochlear groove deepening, femoral osteotomy, tibial osteotomy, antirotational sutures and transposition of the origin of the rectus femoris. A combination of techniques are usually needed to achieve patellar stability. The primary problem is biomechanical. Surgeries that involve only deepening the trochlear groove, capsule and fascial release, and imbrication are more prone to failure. The patella and groove have not been permanently realigned.

21
Soft Tissue Release of the medial retinaculum
Stabilizes patella in groove Reinforcement of the lateral retinaculum Imbrication of the joint capsule Quadriceps release Anti-rotational suture Release of the medial retinaculum may be necessary to allow the patella to stabilize in the deepened trochlear groove. This involves incision in the retinaculum or joint capsule and allowing the tissue to remain open. It allows the patella to move to the opposite side of where the incision is made. Once the patella is stable, the lateral retinaculum is reinforced via imbrication. This is tightening of the soft tissues on the medial or lateral aspect of the joint. This may be performed by an imbricating suture, such as a Lembert pattern, or by actual incision of the tissue and overlap (classically the “vest-over-pants” suture). In some instances the attachment of the quadriceps mechanism to the femur prevents realignment of the extensor mechanism following orthopedic reconstruction. When this occurs, the joint capsule is incised and the incision is extended proximally along the quadriceps musculature. The quadriceps is then undermined to release it from the femur, allowing realignment to occur. This is a suture generally placed from the fabella to the tibial crest or parapatellar region, and is used to prevent internal rotation of the tibia. The suture is generally used to temporarily stabilize the patella, and ultimate stabilization is based on fibrous tissue production.
. In some instances the attachment of the quadriceps mechanism to the femur prevents realignment of the extensor mechanism following orthopedic reconstruction. When this occurs, the joint capsule is incised and the incision is extended proximally along the quadriceps musculature. The quadriceps is then undermined to release it from the femur, allowing realignment to occur. This is a suture generally placed from the fabella to the tibial crest or parapatellar region, and is used to prevent internal rotation of the tibia. The suture is generally used to temporarily stabilize the patella, and ultimate stabilization is based on fibrous tissue production.")
22
Trocheoplasty Deepening of the trochlear groove:
Trochlear wedge or block recession Trochlear chondroplasty Trochlear sulcoplasty all trochleoplasties involve deepening of the trochlear groove in order to help “capture” the patella and prevent luxation. These include a trochlear wedge or block recession, a trochlear chondroplasty or a trochlear sulcoplasty. A wedge or block recession is technically more challenging but preserves the articular cartilage.

23
Tibial Tuberosity Transposition
Realigns the extensor mechanism Realigns the attachment of the patellar ligament The tibial tuberosity transposition changes the alignment of the extensor mechanism relative to the femoral trochlea. Most commonly, the tuberosity is moved to a lateral position to correct MPL’s. This procedure is used to realign the extensor mechanism by realigning the attachment of the patellar ligament. It is described in detail in many texts, and is illustrated in this presentation.

24
Femoral Osteotomy Severe skeletal deformities Goal
Varus bowing of the distal femur Medial torsional deformity of the proximal tibia Goal Realign the stifle joint In conjunction with previous procedures Femoral osteotomy is used only in patients that have such severe skeletal deformities that the afore mentioned techniques are inadequate and maintaining patellar reduction. These deformities usually include varus bowing of the distal femur and medial torsional deformity of the proximal tibia. The goal of surgery is to realign the stifle joint in the frontal plane where the transverse axis of the femoral condyles I perpendicular to the longitudinal axis of the femoral diaphysis. The above mentioned procedures are done in conjunction with this procedure. Require specialized training and equipment.

25
CCLR Quadriceps mechanism Chronic luxation
Secondary stabilizer of the stifle joint for cranial drawer Chronic luxation Increased stress on the CCL Eventual rupture The quadriceps mechanism is a secondary stabilizer of the stifle joint for cranial drawer. Thus, chronic luxation of the patella may lead to increased stress on the CCL and eventual rupture. Combinations of CCL and patellar luxation are common findings, esp in small breed dogs.

26
Post-operative care Soft padded bandage Restricted exercise
6 weeks Physical rehabilitation Leash walks Gradual return to normal activity Over 6 weeks Radiographs at 6-8 weeks Assess healing of the tibial crest transposition The limb is placed in a soft-padded bandage for approximately 3 days. Exercise restriction to include specific physical rehabilitation and leash walking for 6 wks. The patient should then be gradually returned to normal activity over a 6 wk period. Radiographs should be taken at 6 to 8 wks to evaluate healing of the tibial crest transposition.

27
Prognosis Grade I-III Grade IV Excellent after surgical correction DJD
Reluxation 50% of cases Grade I Grade IV Guarded Multiple surgeries Corrective osteotomies Recurrent luxation after surgery has been reported in up to 50% of joints re-evaluated. However, most are grade I luxation's that don’t affect clinical function. Overall prognosis for patient’s with a grade I-III that undergo surgical stabilization is excellent for return to normal function. DJD progresses despite tx but it is not as severe as that reported with CCLR. Prognosis for grade IV is guarded and many require mult surgeries and some patella's can’t be reduced without major corrective osteotomies.

28
“Penny” - outcome 4 days post-op 3 weeks post-op Bandage removal
Placing weight when standing Emphasized restricted activity Owner let Penny off leash in lobby 3 weeks post-op Acutely lame after jumping off couch Seemed okay at recheck to owner Walking well, placing weight on all 4 limbs No instability detected on palpation

29
References Fossum, TW. Small Animal Surgery. 3rd edition, Elsevier, 2007, pp Tilley, LP, Smith, FW. Blackwell’s Five-Minute Veterinary Consult: Canine & Feline. 4th edition, Blackwell, 2007, pp Slatter, D. Textbook of Small Animal Surgery. 3rd edition, Saunders, 2002, pp Johnston, S. Patella Luxation. SAMS 5345 Lecture, 2008.

30
We would like to thank you for your continued support and referrals.

Similar presentations


>")


>")







 Tear. Development of LCL Tear A varus force to the medial aspect of the knee while bearing weight can put enough stress.>")


 Tear>")

>")

