Download presentation
Presentation is loading. Please wait.

1
Enteroviruses Dr. Mohammad Shakeeb, MD Specialist in clinical pathology/Microbiology and immunology

2
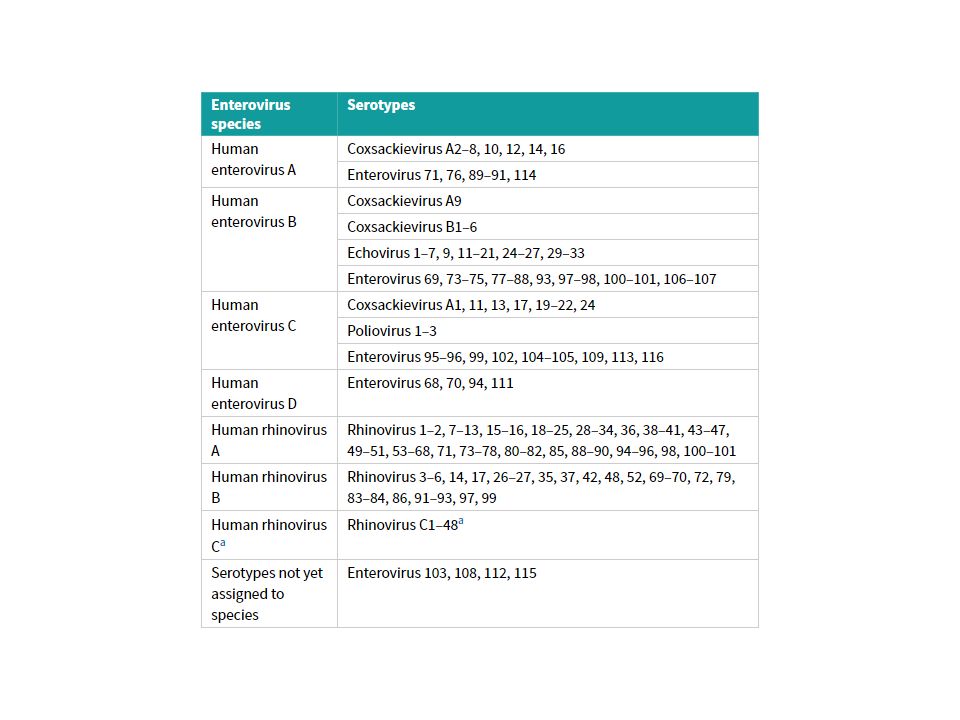
The family picornaviridae comprises small (pico) RNA viruses with a diameter of 27–30 nm. It consists of 12 genera of which the enterovirus (incorporating the former rhinovirus genus), parechovirus and hepatovirus genera are of considerable human importance. The enterovirus genus is divided according to genetic phylogeny into 10 species.
, parechovirus and hepatovirus genera are of considerable human importance. The enterovirus genus is divided according to genetic phylogeny into 10 species..")
4
Viruses belonging to the human enterovirus species A–D of the genus enterovirus infect via the gut. excreted in feces. include the echoviruses, coxsackieviruses and polioviruses. New enteroviruses continue to be isolated

5
RNA genome is single-stranded and of positive sense (ss+ve RNA) and, therefore, can be translated directly by host ribosomes to generate viral proteins. It is surrounded by a capsid consisting of a protein shell arranged in icosahedral symmetry around the genomic RNA. Four major peptides are recognized in the shell: viral protein (VP) 1, VP2, VP3 and VP4, formed from a single precursor protein, VP0, by proteolytic cleavage.
 1, VP2, VP3 and VP4, formed from a single precursor protein, VP0, by proteolytic cleavage..")
6
Specific neutralizing antibodies are considered to be the major mechanism of protection against infection. The virus is non-enveloped.

7
In addition, all enteroviruses: attach to cells of the intestinal tract at specific receptor sites and replicate in the cytoplasm of the intestinal cells. commonly cause asymptomatic immunizing infections which protect against future infections with the same virus. occasionally cause infection of the central nervous system (CNS) and other target organs. are commoner in children than in adults. usually cause infections in late summer and early autumn (in temperate climates).
 and other target organs. are commoner in children than in adults. usually cause infections in late summer and early autumn (in temperate climates)..")
8
Clinical features and pathogenesis The enteroviruses are associated with a wide variety of clinical presentations. the majority of infections are asymptomatic. The main sites affected are: CNS (aseptic meningitis, paralytic poliomyelitis, encephalitis), particularly in children; persistent CNS infection (primarily encephalitis) may develop in immunocompromised patients. skin and mucosa (maculopapular rashes, ulcerative exanthem).
, particularly in children; persistent CNS infection (primarily encephalitis) may develop in immunocompromised patients. skin and mucosa (maculopapular rashes, ulcerative exanthem)..")
9
striated muscle (intercostal myositis, myocarditis accompanied by pericarditis). respiratory tract (rhinitis, pharyngitis, bronchiolitis, pneumonia). eyes (conjunctivitis). postnatal infection in neonates can be severe, extensive and occasionally fatal. Maternal infection in pregnancy is not associated with congenital defects.
. eyes (conjunctivitis). postnatal infection in neonates can be severe, extensive and occasionally fatal. Maternal infection in pregnancy is not associated with congenital defects..")
10
Polioviruses There are three outcomes of poliovirus infection: Asymptomatic infection, or a mild, transient ‘influenza-like’ illness. This is the most likely outcome with only 1% of infections resulting in recognizable clinical illness. The virus is excreted in feces for a limited time. Immunological response develops that protects against re- infection with the same strain.

11
Aseptic meningitis Infections with the same symptoms as above and evidence of CNS involvement. Headache, photophobia, neck stiffness and back pain. Rapid and complete recovery in less than 10 days is usual.

12
Paralytic poliomyelitis (‘polio’) in which the patient develops paralysis. This is the most dramatic form of the infection. Very uncommon. The paralysis is usually flaccid due to destruction of lower motor neurons. Invasion of the brainstem by the virus can lead to incoordination of muscle groups and painful spasms. Paralysis occurs early in the illness but the extent is variable. Damage to nerve cells in the brainstem (bulbar paralysis) can lead to the inability to breathe and swallow.
 can lead to the inability to breathe and swallow..")
13
The time between infection and the development of symptoms is usually 14 days but can range from 3–21 days. Increased muscular activity can lead to paralysis of the limbs used. Women in the third trimester of pregnancy can have severe disease, but there is no firm evidence of congenital defects in infants born to mothers with poliomyelitis;. Patients who have had their tonsils removed have a higher chance of developing bulbar poliomyelitis which has been attributed to the reduction of secretory immunoglobulin (Ig) A in the pharynx and, thus, reduced neutralization of virus.
 A in the pharynx and, thus, reduced neutralization of virus..")
14
Echoviruses Most echovirus infections cause few or no clinical symptoms, but some have been associated with clinical syndromes including: aseptic meningitis. Paralysis. maculopapular rash. respiratory disease.

15
Less frequently, echoviruses may cause: myocarditis and pericarditis neonatal infection. Infection can be widespread in a community. Few suffer from clinical illness. Symptoms occur following a short incubation period of 3–5 days. simple fever, upper respiratory symptoms or diarrhea. The onset of aseptic meningitis is abrupt, with severe headache and vomiting.

16
Symptoms are self-limiting, and after a variable convalescent period a full recovery is made. Most of the echovirus types have been associated with sporadic cases of aseptic meningitis. A number of types have considerable epidemic potential. echovirus 9 epidemics have been common in Europe and North America as large outbreaks. Echovirus 18 has been recovered from faeces of many infants in an outbreak of diarrhoea.

17
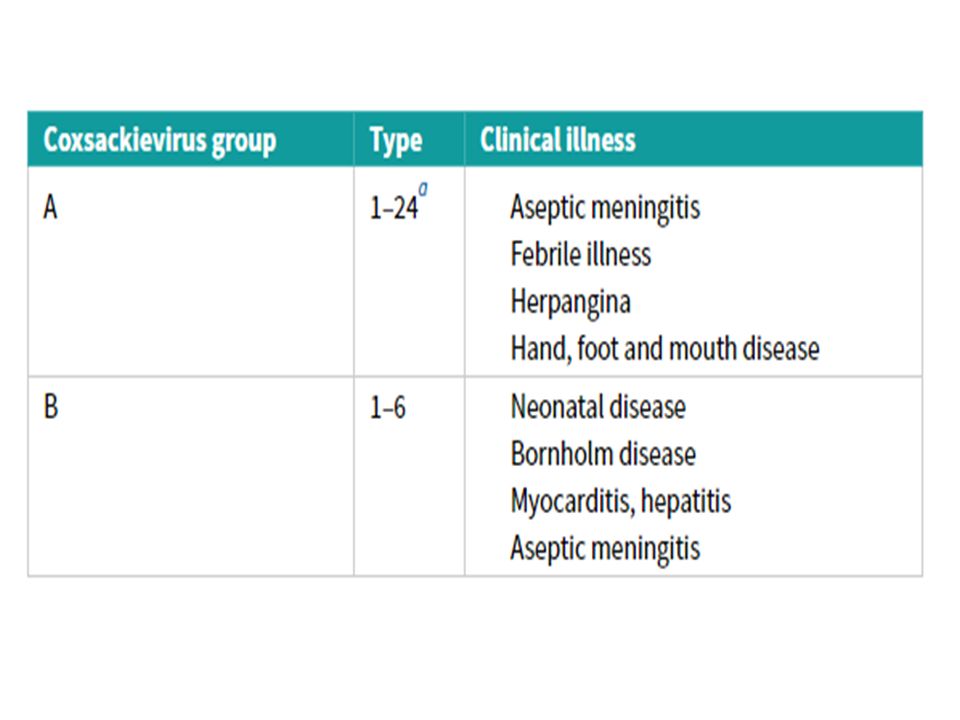
Coxsackieviruses Group A viruses Aseptic meningitis Aseptic meningitis is caused by a number of types (e.g. 2, 4, 7, 9 and 23). Herpangina Herpangina is an acute feverish disease with sore throat and pain on swallowing, usually in young children. characterized by lesions in the mouth consisting of papules on the anterior pillars, soft palate, uvula, pharynx and tonsils; these papules become vesicles and finally shallow ulcers with a greyish base and punched-out edge.
. Herpangina Herpangina is an acute feverish disease with sore throat and pain on swallowing, usually in young children. characterized by lesions in the mouth consisting of papules on the anterior pillars, soft palate, uvula, pharynx and tonsils; these papules become vesicles and finally shallow ulcers with a greyish base and punched-out edge..")
18
There are usually small numbers of lesions. A fine maculopapular rash (‘rubelliform’) is a feature of some Coxsackie infections. Outbreaks may be seen in nurseries and schools. Hand, foot and mouth disease Hand, foot and mouth disease presents as a mildly febrile ulcerative exanthem with painful stomatitis and a painful vesicular rash on the hands and/or feet (less frequently, on buttocks and external genitalia). It lasts about a week. Most cases are seen in summer in children aged 1–10 years
 is a feature of some Coxsackie infections. Outbreaks may be seen in nurseries and schools. Hand, foot and mouth disease Hand, foot and mouth disease presents as a mildly febrile ulcerative exanthem with painful stomatitis and a painful vesicular rash on the hands and/or feet (less frequently, on buttocks and external genitalia). It lasts about a week. Most cases are seen in summer in children aged 1–10 years.")
19
Cases can occur in clusters and in families. The viruses usually implicated are types 5 and 16. Group B viruses Epidemic pleurodynia, or Bornholm disease. Epidemic pleurodynia, or Bornholm disease. First described on the Danish island of Bornholm. It is characterized by fever and the sudden onset of agonizing stitch-like pains in the muscles of the chest, epigastrium or hypochondrium. Pleurisy and pericarditis may complicate epidemic myalgia, although most cases recover within a week.

20
newborn infants In newborn infants, severe and often fatal myocarditis has been reported. And the virus can be found in high concentrations in the myocardium at autopsy. Epidemics have occurred in nurseries when there is evidence of group B virus activity in a community. Myocarditispericarditis Myocarditis and pericarditis can occur in children and adults, and virus has been isolated from pericardial fluid. Coxsackie B viruses are major causes of human myopericarditis, but this is a difficult diagnosis to confirm.

21
It tends to follow a more benign course in the adult. The initial symptoms are often of an upper respiratory or ‘influenza-like’ illness followed 7–10 days later by clinical heart disease. Chest pain is a feature and electrocardiographic abnormalities such as tachycardia and arrhythmias have been found. On clinical examination, murmurs, rubs and, occasionally, pericardial effusions are detected. Aseptic meningitis Aseptic meningitis, sometimes with paralysis, is a common manifestation of infection due to group B viruses. maculopapular rash Occasionally, a maculopapular rash is present.

23
Enteroviruses 68–71

24
Pathogenesis All enterovirus infections follow a similar pattern. differences in the target organs (e.g. CNS, skin, heart or muscle). Virus is ingested. Multiplication in the lymphoid tissue of the tonsils or Peyer’s patches (gut-associated lymphoid tissue, GALT) and the local lymph nodes. It enters the blood and then the CNS.
. Virus is ingested. Multiplication in the lymphoid tissue of the tonsils or Peyer’s patches (gut-associated lymphoid tissue, GALT) and the local lymph nodes. It enters the blood and then the CNS..")
25
The paralytic effect of poliovirus is due to destruction of motor neuron cells in the anterior horns of the spinal cord or bulbar regions. Once within the brain or spinal cord, virus can spread directly to neighboring cells, or indirectly via the CSF. The viremia phase marks the end of the incubation period, and is manifest in the patient by fever and generalized symptoms. It is followed by a period of about 48 h of relative well-being. If antibody is present in blood, virus can be prevented from reaching the CNS.

26
Enteroviruses are lytic, destroying the infected cell within a few hours to days. Cell damage will trigger an inflammatory response; the resultant edema may affect neurons. As the edema resolves, function will recover in these uninfected cells. explaining the apparent improvement in the degree of paralysis in the weeks to months after the acute stage.

27
Laboratory diagnosis Virus isolation was the most useful method for establishing a diagnosis. Examination of CSF is an essential part of the laboratory diagnosis of meningitis. Nucleic acid amplification tests have become the most common approach to enterovirus detection. Although specific IgM and IgG (EIA) for enteroviruses are available, their use is limited.
 for enteroviruses are available, their use is limited..")
28
Treatment Treatment is symptomatic. Epidemiology and transmission The only natural source of poliovirus is man. The virus is spread from person to person. no intermediate host is known.

29
Transmission All enteroviruses are excreted in large numbers from the gut and are ingested to cause infection. This can be achieved in the following ways: by direct transfer on fingers (fecal–oral transfer). on eating utensils.( اواني ) through contamination of food or drink. by entry through the conjunctiva (rare). Outbreaks are often seen in closed communities (e.g. military establishments) and schools.
. on eating utensils.( اواني ) through contamination of food or drink. by entry through the conjunctiva (rare). Outbreaks are often seen in closed communities (e.g. military establishments) and schools..")
30
Cases are most infectious late in the incubation period, but infection can be transmitted at any time during virus excretion in feces. Social factors, such as standards of hygiene and overcrowding, are also important. Sewage can contain polioviruses, particularly when there is infection in a community. Enteroviruses can survive for several months in river water. unlikely to survive in chlorine-treated water or swimming pools where the recommended level of chlorination is achieved.

31
Prevention and control After natural infection, immunity is long lasting. Virus-neutralizing antibodies are formed early during the disease (often before the 7th day). persist for several decades. Secretory IgA is produced in the gut. In the clinical setting, standard infection control precautions (including adequate hand hygiene) are critical in preventing spread.
. persist for several decades. Secretory IgA is produced in the gut. In the clinical setting, standard infection control precautions (including adequate hand hygiene) are critical in preventing spread..")
32
Immunization Polio is a vaccine preventable disease. There are two types of polio vaccine: inactivated. live-attenuated.

33
Inactivated polio vaccine (Salk vaccine) Developed by Jonas Salk (USA). this vaccine contains strains of the three types of virus grown in monkey kidney cell culture and inactivated by exposure to formaldehyde. The vaccine should be administered by deep subcutaneous or intramuscular injection. A primary course of three injections given with an interval of 1 month between each dose is recommended for infants of 2 months of age.

34
followed by booster doses at 1–3 years after the primary course and at 5–10 years after the first booster. Live-attenuated polio vaccine (Sabin vaccine) Developed by Albert Sabin (USA) in 1959. it contains live but attenuated strains of poliovirus types 1, 2 and 3, grown in cultures of either monkey kidney cells or human diploid cells. The vaccine is administered orally. thus mimics natural infection with stimulation of circulating IgG and local secretory IgA in the pharynx and alimentary tract.
 Developed by Albert Sabin (USA) in it contains live but attenuated strains of poliovirus types 1, 2 and 3, grown in cultures of either monkey kidney cells or human diploid cells. The vaccine is administered orally. thus mimics natural infection with stimulation of circulating IgG and local secretory IgA in the pharynx and alimentary tract..")
35
producing local resistance to subsequent infection with wild- type polioviruses. The wide circulation of vaccine virus, which helps to maintain immunity in the community. Vaccine-associated poliomyelitis has been reported in oral vaccine recipients at a rate of 1 in 2 million doses, and it has also been seen in contacts of recipients. The primary course consists of three separate doses given at the same time as the then used diphtheria/tetanus/pertussis vaccine.

36
Each dose contains all three poliovirus strains. In infants, three drops are dropped from a spoon directly into the mouth. A reinforcing dose is given to children at school entry and prior to leaving school.

Similar presentations













 Virus>")


, Hepatovirus Picornavirus, enterovirus 72 27 nm 1 serotype only, although there are 4 genotypes.>")


