Download presentation
Presentation is loading. Please wait.

1
Adrenal insufficiency

2
Objectives By the end of this lecture, the student will be able to:
Define adrenal insufficiency. List the causes of adrenal insufficiency. Describe clinical presentation of Addison’s disease. Outline the plan of management of Addison’s disease. Define adrenal crisis and recognize its clinical features. Identify the lines of treatment of adrenal crisis.

3
There is a decrease in the secretion of cortisol and or aldosterone
Definition: There is a decrease in the secretion of cortisol and or aldosterone Variable presentation and potentially fatal. Prevalence of permanent adrenal insufficiency is 5 in 10,000. CAUSES Secondary (low ACTH) is the most common. Pituitary tumors (endocrine adenomas, rarely carcinoma). Mass lesions affecting the HP region(craniopharyngioma, meningioma, metastases). Pituitary irradiation. Pituitary apoplexy/hemorrhage. Pituitary infiltration (TB, actinomycosis, sarcoidosis, Wegener's granulomatosis, metastases). Chronic glucocorticoid excess. Glucocorticoids are hormone steroids such as cortisol that regulate metabolism of glucose Mineralcorticoids are also hormone steroids such as aldesterone that balances water and salt intake However children lead to a more rapid progression of the disease than adults Although gender is considered to be equally effected, there are many studies that show there is a slightly higher prevalence in women than in men This figure shows the regulation of cortisol which is regualted by the adrenal glands and ultimately by the pitutary.
 is the most common. Pituitary tumors (endocrine adenomas, rarely carcinoma). Mass lesions affecting the HP region(craniopharyngioma, meningioma, metastases). Pituitary irradiation. Pituitary apoplexy/hemorrhage. Pituitary infiltration (TB, actinomycosis, sarcoidosis, Wegener s granulomatosis, metastases). Chronic glucocorticoid excess. Glucocorticoids are hormone steroids such as cortisol that regulate metabolism of glucose. Mineralcorticoids are also hormone steroids such as aldesterone that balances water and salt intake. However children lead to a more rapid progression of the disease than adults. Although gender is considered to be equally effected, there are many studies that show there is a slightly higher prevalence in women than in men This figure shows the regulation of cortisol which is regualted by the adrenal glands and ultimately by the pitutary.")
4
Combined pituitary hormone deficiency (CPHD).
Congenital isolated ACTH deficiency. Primary (high ACTH) Addison’s disease: Autoimmune (sporadic or polyglandular failure, APS1 and APS2)) Adrenal infection (TB, HIV, CMV, cryptococcosis, histoplasmosis, coccidioidomycosis). Adrenal infiltration (Metastases, lymphomas, sarcoidosis, amyloidosis, hemochromatosis). Bilateral adrenalectomy. Adrenoleukodystrophy (ALD).
 Addison’s disease: Autoimmune (sporadic or polyglandular failure, APS1 and APS2)) Adrenal infection (TB, HIV, CMV, cryptococcosis, histoplasmosis, coccidioidomycosis). Adrenal infiltration (Metastases, lymphomas, sarcoidosis, amyloidosis, hemochromatosis). Bilateral adrenalectomy. Adrenoleukodystrophy (ALD).")
5
Adrenal hemorrhage (Meningococcal sepsis (Waterhouse-Friderichsen syndrome), primary antiphospholipid syndrome. Imparied Steriodiogensis CAH Drugs (ketoconazole, etomidate, metyrapone etc)
")
6
Addison’s disease First discovered by Thomas Addison in 1855
First described as an infection of the adrenal gland- most commonly TB. Now instead of infection, its most commonly characterized by an autoimmune destruction of the adrenal glands He was a British physician that studied 6 pattients all that had TB. Since TB prevalence has decreased, it is now characterized by an autoimmune destruction of adrenal glands. There has to be 90% destruction of the adrenal glands in order to be considered Addison’s. One famous person that had Addison’s is John F. Kennedy and he is thought to be the first Addisonians to survive major surgery.

7
Epidemiology Addison’s disease is a rare and chronic disease.
Prevalence of 2 in 10,000 per year. 1.4 million deaths per year around the world. Usually effects year-olds, but can be seen in all ages. AI arising from suppression of the HPA axis as a consequence of exogenous glucocorticoid treatment occurs in 0.5–2% of the population in developed countries.

8
Clinical Features Signs and Symptoms Caused by Glucocorticoid Deficiency: Chronic fatigue Weight loss, anorexia Myalgia, joint pain Hypoglycemia, Hyponatremia due to loss of feedback inhibition of ADH release Anemia, eosinophilia and lymphocytosis Low blood pressure, postural hypotension Fever Slightly increased TSH (due to loss of feedback inhibition of TSH release) Symptoms are generally nondescriptive and can be thought of as sypmtoms for many other less significant problems. They include…. Hypercalcemia which is increase in blood calcium, hypoglycemia which is low blood glucose, hypoatremia which is low blood sodium levels, an hyperkalemia which is raised blood potassium. There is also esinophilia and lympocytosis which is an increase in esinophils and lymphocytes in blood. You can also have metabolic acidosis due to loss of aldosterone which leads to less reabosprtion of sodium in the distal tubule of the nephron in kidneys. There is an event called addisonian crisis which is caused by your flight or fight response so if some has an exteremly traumatic experince or doesn’t manage their disease accordingly this could occur. Its charactereized by severly low blood pressure which could lead to potential coma or death.
 Symptoms are generally nondescriptive and can be thought of as sypmtoms for many other less significant problems. They include…. Hypercalcemia which is increase in blood calcium, hypoglycemia which is low blood glucose, hypoatremia which is low blood sodium levels, an hyperkalemia which is raised blood potassium. There is also esinophilia and lympocytosis which is an increase in esinophils and lymphocytes in blood. You can also have metabolic acidosis due to loss of aldosterone which leads to less reabosprtion of sodium in the distal tubule of the nephron in kidneys. There is an event called addisonian crisis which is caused by your flight or fight response so if some has an exteremly traumatic experince or doesn’t manage their disease accordingly this could occur. Its charactereized by severly low blood pressure which could lead to potential coma or death.")
9
Abdominal pain, nausea, vomiting Dizziness, postural hypotension
Signs and Symptoms Caused by Mineralocorticoid Deficiency (Primary AI Only) : Abdominal pain, nausea, vomiting Dizziness, postural hypotension Salt craving Low blood pressure, postural hypotension Increased serum creatinine (due to volume depletion) Hyponatremia Hyperkalemia
 : Abdominal pain, nausea, vomiting. Dizziness, postural hypotension. Salt craving. Low blood pressure, postural hypotension. Increased serum creatinine (due to volume depletion) Hyponatremia. Hyperkalemia.")
10
Signs and Symptoms Caused by Adrenal Androgen Deficiency :
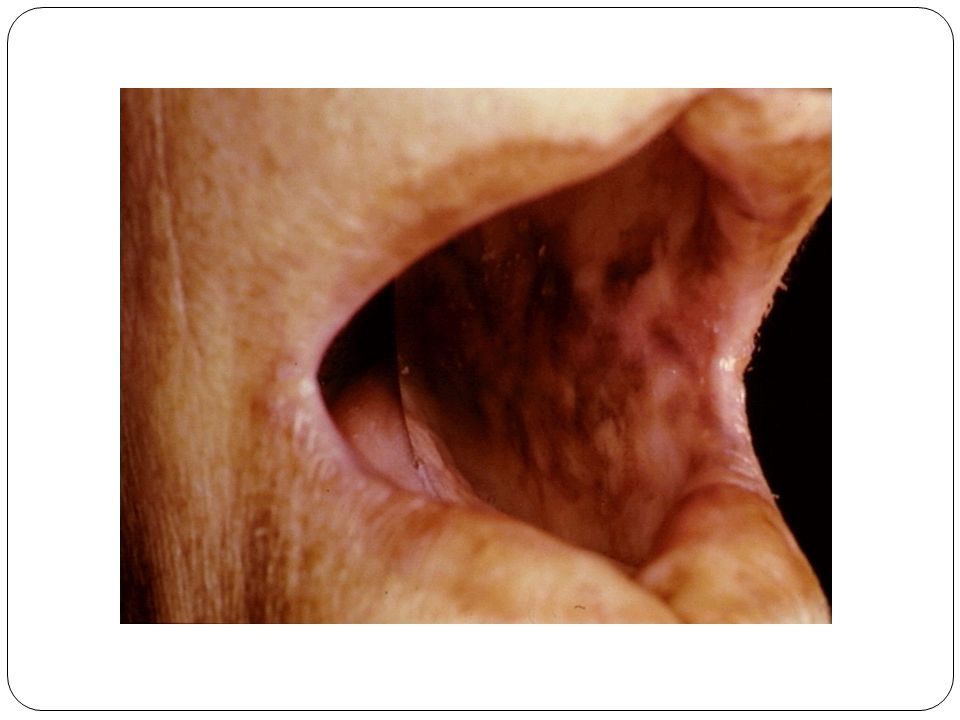
Lack of energy Dry and itchy skin (in women) Loss of libido (in women) Loss of axillary and pubic hair (in women) Other Signs and Symptoms: Hyperpigmentation (primary AI only) [due to excess of pro-opiomelanocortin (POMC)–derived peptides] Alabaster-colored pale skin (secondary AI only) (due to deficiency of POMC-derived peptides)
 Loss of libido (in women) Loss of axillary and pubic hair (in women) Other Signs and Symptoms: Hyperpigmentation (primary AI only) [due to excess of. pro-opiomelanocortin (POMC)–derived peptides] Alabaster-colored pale skin (secondary AI only) (due to deficiency of POMC-derived peptides)")
13
Acute adrenal insufficiency
More frequently observed in patients with primary AI. Postural hypotension may progress to hypovolemic shock. AI may mimic features of acute abdomen. May resemble neurologic disease, with decreased responsiveness, progressing to stupor and coma. An adrenal crisis can be triggered by an intercurrent illness, surgical stress, infection.

14
Diagnosis Determined by low level of adrenal hormone after stimulation with synthetic ACTH hormone (tetracosactide or short Synacthen test) Short Test: 250 micrograms of cosyntropin i.m or i.v injection Blood cortisol levels min (cortisol post cosyntropin is < 500 nmol/l) CBC, serum Na, K, creatinine, urea, TSH For dDx: Plasma ACTH, rennin, S. aldosterone. High ACTH, high PRA, low aldosterone (primary AI) Low- normal ACTH, normal PRA and aldosterone (secondary)
 CBC, serum Na, K, creatinine, urea, TSH. For dDx: Plasma ACTH, rennin, S. aldosterone. High ACTH, high PRA, low aldosterone (primary AI) Low- normal ACTH, normal PRA and aldosterone (secondary)")
15
Adrenal autoantibody Antibodies against (steroid secreting cells, thyroid Ag, parietal cells, pancreatic cells) CBC to look for pernicious anemia Blood Ca and glucose CXR, U/S and X-ray of adrenals for TB calcifications CT or MRI of adrenals for malignancies, hemorrhage. HIV test Serum Na and K Tests for 17OHP and in men plasma VLCFA. MRI pituitary for hypothalamic pituitary mass.

16
Treatment Replacement ( always need glucocorticoid and usually mineralcorticoid therapy). Cortisol orally 15 mg at morning and 5 mg at evening 1 mg hydrocortisone, 1.6 mg cortisone acetate, 0.2 mg prednisolone, 0.25 mg prednisone, and mg dexamethasone. Doses change according to lifestyle, i.e. stress, infection, or injury Have to carry emergency injection of hydrocortisone and steroid card/bracelet indentifying their condition. Monitor treatment by body w.t and BP.

17
Mineralocorticoid replacement is by giving fludrocortison 0. 05- 0
Mineralocorticoid replacement is by giving fludrocortison mg/day Adrenal androgen replacement is an option in patients with lack of energy, despite optimized glucocorticoid and mineralocorticoid replacement. It may also be indicated in women with loss of libido. Replacement can be achieved by once-daily administration of 25–50 mg DHEA. Treatment is monitored by measurement of DHEAS, androstenedione, and testosterone.

18
A 32-year-old woman with known hypothyroidism is admitted to hospital
A 32-year-old woman with known hypothyroidism is admitted to hospital. Her BP is 86/53 mmHg and her pulse 100 bpm. Investigations reveal: Serum Na: 126 mmol/L ( ) Serum K: 5.8 mmol/L ( ) Serum glucose: 3.0 mmol/L ( ) What is the most likely diagnosis? What is the most appropriate investigation to confirm your diagnosis?
 Serum K: 5.8 mmol/L ( ) Serum glucose: 3.0 mmol/L ( ) What is the most likely diagnosis What is the most appropriate investigation to confirm your diagnosis")
19
Addisonian Crisis Severe hypotension (shock) Hyperkalemia Hyponatremia
Hypoglycemia Unexplained fever, diarrhea, vomiting Could cause coma and death Precipitated by infection, surgery or intercurrent disease

20
Treatment It is a medical emergency
IV fluid( normal saline 1L/h and 10% dextrose) Hydrocortisone 100 mg bolus then mg over 24h (infusion or multiple injections) until GI symptoms improve then start oral therapy Mineralocorticoid replacement can be initiated once the daily hydrocortisone dose has been reduced to <50 mg. Treat ppt cause
 Hydrocortisone 100 mg bolus then mg over 24h (infusion or multiple injections) until GI symptoms improve then start oral therapy. Mineralocorticoid replacement can be initiated once the daily hydrocortisone dose has been reduced to <50 mg. Treat ppt cause.")
Similar presentations





, FRCP Consultant Endocrinologist>")








 are the triangle-shaped and orange- colored endocrine.>")





