Download presentation
Presentation is loading. Please wait.

1
chronic obstructive pulmonary disease (COPD) PREPARED BY: Miss Fatima Hirzallah RN,MSN,CNS
 PREPARED BY: Miss Fatima Hirzallah RN,MSN,CNS")
2
2

3
3

4
4 chronic obstructive pulmonary disease (COPD) Is a disease state characterized by airflow limitation that is not fully reversible. COPD may include disease that cause airflow obstruction (emphysema, bronchitis or chronic obstruction) or a combination of these disorders. Other disease as, bronchiectasis, and asthma were previously classified as types of COPD.
 or a combination of these disorders. Other disease as, bronchiectasis, and asthma were previously classified as types of COPD..")
5
5 Pathophysiology In COPD, the airflow imitation in both progressive & associated with an abnormal inflammatory response of the lungs to noxious particles or gases. The inflammatory process occurs through out the airway, parenchyma, & pulmonary vasculature. Because of the chronic inflammation & the body’s attempts to repair it, narrowing occurs in the small peripheral air way. Over time, this injury & repair process cause scar tissue formatting & narrowing of the airway lumen.

6
6 Airflow obstruction may also due to parenchymal destruction as seen with emphysema, a disease of the alveoli or gas exchange units. When activated by chronic inflammation proteinases and other substances may released & damaging the parenchyma of the lung. Parenchyma change may be due to inflammation, environmental, and genetic factors

7
7 Early in the course of COPD, the inflammatory response cause pulmonary vascular changes, thickening of the vessel wall. This may occur as a result of smoke or tobacco products.

8
8 Chronic Bronchitis A disease of the airway is defined as the presence of cough & sputum production for at least 3 months in each of two consecutive years. In many cases, smoke or environmental pollutants irritant the airway, resulting in hypersecreation of mucus & inflammation. This constant irritation causes the mucous-secretion glands and goblet cell to increase in number, ciliary function is reduce, & more mucus is produced.

9
9 Bronchial walls become thickened, the bronchial lumen is narrowed, and mucus may blug the airway. Alveolar adjacent to the brochioles may become damaged & fibrosed resulting in altered function of the alveolar macrophages. Which play a big role in destroying foreign particles, including bacteria. As a result pt. is more susceptible to respiratory infection.

10
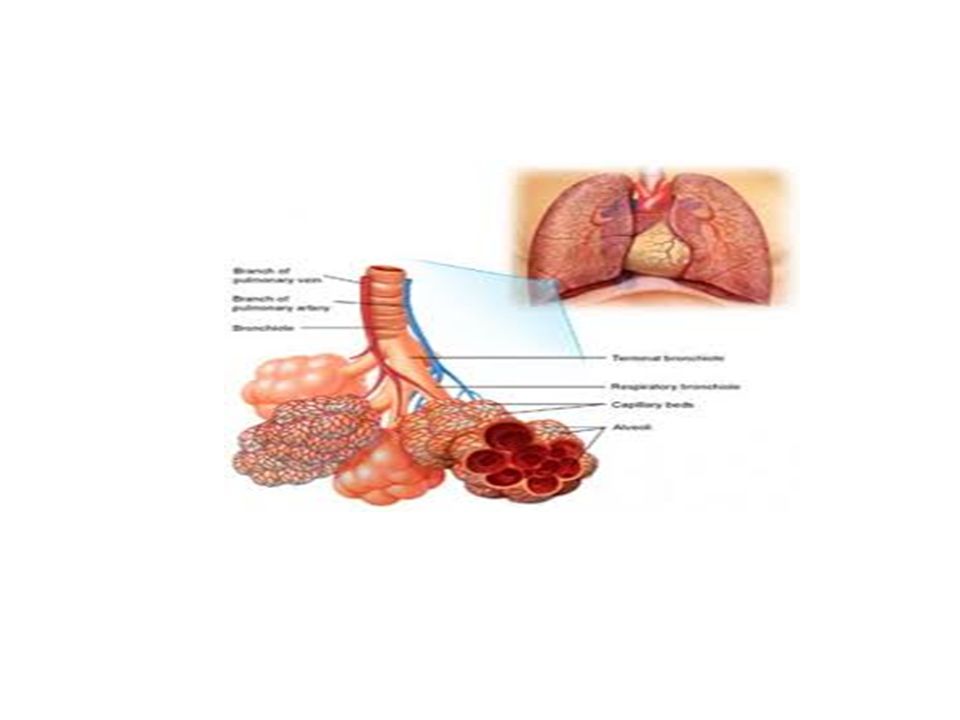
10 Emphysema Impaired gas exchange (O2.CO2).Result from destruction of the walls of over distended alveoli. It’s a pathological term that describes an abnormal distention of the air spaces beyond the terminal bronchioles, with destruction of the walls of the alveoli. Its end process that has progressed slowly for many years.

12
12 As the walls of the alveoli are destroyed, the alveolar surface area in direct contact with the pulmonary capillaries continually decreases, causing an increase in dead space (lung area where no gas exchange can occur) and impaired O2 diffusion, CO2 elimination is impaired resulting in increase CO2 tension in arterial line & resp. acidosis.

14
14

15
15 Consequently blood pulmonary blood flow is increase, forcing the Rt. Ventricle to maintain a higher blood pressure in pulmonary artery. Hypoxemia also increase pulmonary artery pressure. Thus Rt.-sided heart failure (cor pulmonal) is one complication of emphysema. Congestion, dependent edema, distended neck veins, or pain in the region of liver suggests the development of cardiac failure.
 is one complication of emphysema. Congestion, dependent edema, distended neck veins, or pain in the region of liver suggests the development of cardiac failure..")
16
16 Rt.pulmonary hypertrophy may result, followed by Rt. Ventricular failure. (in short cor pulmonary results from pulmonary hypertension, which may causes the Rt.side of the heart to enlarge because of the increased work required to pump blood against high resistance through the pulmonary vascular system).
..")
17
17 There are two main types of emphysema, based on changes taking place in the lung: pan lobular and centrilobular. Pan lobular…destruction of resp. bronchiole, alveolar duct, and alveoli. All air spaces within the lobule are essentially enlarged. In this type pt has barrel chest, dyspnea, to move air out of the lungs, negative pressures is required.

18
18 Risk Factors It includes environmental exposure and host factors for COPD is cigarette smoking, pipe, cigar, & other types of tobacco smoking. Smoking depress the activity of scavenger cells & affect respiratory tract ciliary cleansing mechanism, which keeps breathing passages free of inhaled irritant, bacteria, & other foreign matter. When smoking damaged this cleansing mechanism, airflow is obstructed & air becomes trapped. Behind the obstruction.

19
19 Other factors include prolonged & intense exposure to occupational dusts & chemicals. A host risk of factor, is a deficiency of alpha, anti- trypsin, an enzyme inhibitor that protects the lung parenchyma from injury. This predisposes young pt. to rapid development of lobular emphysema even in the abscent of smoking. Alpha, antitrypsin deficiency is one of the most common genetically linked lethal among causasion & affects approximately one in every 3,000 Americans.

20
20 S&S It characterized by three primary symptoms: cough, sputum production, and dyspnea on exertion. These symptoms often worsen over the time. Often pt cannot participate in even mild exercise because of dyspnea, as COPD progress, dyspnea occur at rest.

21
21 Pt with COPD is at risk respiratory insufficiency & infections. In COPD Pt with a primary emphysematous component, chronic hyperinflation leads to the barrel chest. This results from fixation of the ribs in the inspiration position (due to hyperinflation) and from loss of lung elasticity. Retraction of the supraclavicular fossae occurs on inspiration, causing the shoulder to have upwared. Advance emphysema, the abdominal muscle also contract on inspiration.
 and from loss of lung elasticity. Retraction of the supraclavicular fossae occurs on inspiration, causing the shoulder to have upwared. Advance emphysema, the abdominal muscle also contract on inspiration..")
23
23 Assessment and diagnostic finding Health history for pt with potential COPD. Pulmonary function study. Spirometry is used to evaluate airflow obstruction ABGS. Chest x-ray. alpha, anti-trypsin screening may be performed for pt under age 45, or those with strong family history.

24
24 In DX of COPD, several differential DX must be ruled. ( the primary differential DX is asthma). The key part of differentiation is the pt history, as well as pt responsiveness to bronchodilators.
. The key part of differentiation is the pt history, as well as pt responsiveness to bronchodilators..")
26
26 Complication Respiratory insufficiency & failure are major life threatening complication of COPD. Pneumothorax, pneumonia, atelactasis, & cor pulmonale.

27
27 Medical Management Risk reduction, cessation of smoking is the most effective intervention to prevent COPD. (nicotin gum, inhaler, patches, nasal spray) Pharmacological therapy: bronchodilator, relieve bronchospasm and relieve airway obstruction by allowing increased oxygen distribution through out the lungs and improving alveolar ventilation. A metered-dose inhaler (MDI) is a pressurized device containing an aerosolized powder of medication. Pt instructed on the correct use of the device. (holding chamber).
 Pharmacological therapy: bronchodilator, relieve bronchospasm and relieve airway obstruction by allowing increased oxygen distribution through out the lungs and improving alveolar ventilation. A metered-dose inhaler (MDI) is a pressurized device containing an aerosolized powder of medication. Pt instructed on the correct use of the device. (holding chamber)..")
29
29 Corticosteroids: inhaled and systemic corticosteroid (oral or IV) may be used in COPD, but are used more frequantely in asthma. It has been shown that corticosteroid don’t slow the decline in lung infection, these medication may improve symptoms. Medication regimens used to manage COPD are based on disease severity. For stage one or mild, a short acting bronchodilator. For stage II bronchodilator with inhaled corticosteroid. For stage III or sever regular treatment with one or more bronchodilator and inhaled corticosteroid.

30
30 Pt should receive a yearly influenza vaccine & pneumococcal vaccine every 5-7 years as preventive measures. Management of exacerbation: its difficult to DX, primary causes is tracheobronchial infection & air pollution. Secondary causes are pneumonia, pneumothorac, rib fracture. Optimizing of bronchodilator therapy is the first line. Depending on S&S antibiotic agent, corticosteroid, O2 therapy & respiratory intervention may be used

31
31 O2 therapy: can be administered as long-term continuous therapy, during exercise or to prevent acute dyspnea. Because hypoxemia stimulates respiration in the pt with sever COPD, increasing O2 flow to a high rate may greatly raise the pt blood oxygen level at the same time, this will suppress the respiratory drive, causing increase retention of CO2. The nurse should closely monitor the pt respiratory response to O2 administration via physical assessment, pulse oximetry, and \or arterial blood gases.

32
32 Surgical management: bullectomy is a surgical option for select pt with bolous emphysema. Bullae are enlarged airspaces that don’t contribute to ventilation but occupy space in the thorax. Lung volume reduction surgery: involves the removal of a portion of the diseased lung parenchyma. This allows functional tissue to expand, resulting in improved elastic recoil of the lung, improved chest wall & diaphragmatic mechanism.

33
33 Lung transplantation Pulmonary rehabilitation: it’s well established & widely accepted as a means to alleviate symptoms and optimizing functional status. Most rehabilitation program includes educational, psychosocial, behavioral, & physical competent. Breathing exercise is used to improve functional status.

34
34 NSG Management The nurse plays a key role in identifying potential candidates for pulmonary rehabilitation and in facilitating, & reinforcement the material learned in program. PT Education: is a major component of pulmonary rehabilitation program. It may include normal anatomy & physiology of the lung, path., medication, home O2 therapy, nutrition, coping with chronic disease & communication with health team.

35
35 Breathing exercises: the breathing of most people with COPD is shallow, rapid, & inefficient. With practice this type of upper chest breathing can be changed to diaphragmatic breathing. Inspiratory muscle training. Once the pt diaphragmatic breathing, a program of inspiratory muscle training may be prescribed to help strengthen the muscles used in breathing.

36
36 Activity pacing: pt with COPD has decrease exercise tolerance during specific periods of day. This true on arising in the morning, because bronchial secretion collect in the lungs during night while pt is lying down. Self-care activities: pt encourage to precipitate. Physical conditioning: its include breathing exercise & general exercise.

37
37 Oxygen therapy: portable O2 is allow pt to exercise, work, and travel. Nutritional therapy: 25% of COPD undernourished, also assessment of caloric need & meal planning. Coping measures: frustration of having to work to breath & realization that the disease is prolonged. Nurse needs to provide education, and support to family. (NSG Process-discuss).
..")
38
THANKS

Similar presentations






>")


 into the atmosphere Filter, moisten,>")
 Dr. Walaa Nasr Lecturer of Adult Nursing Second year.>")






>")

 is one of the most common lung disease Makes it difficult to breathe There are two main forms of COPD.>")



