Download presentation
Presentation is loading. Please wait.

1
Cranial nerve palsy

2
Oculomotor nerve palsy
The nuclear complex of the third (IIIrd) nerve lies in midbrain After leaving the brainstem, the nerve enters subarachnoid space and courses forward and laterally between posterior cerebral artery and superior cerebellar artery. At this level the nerve is compressed by Berry Aneurysms then the artery pass through cavernous sinus, together with trochelear 4th ,abducent 6th ,first division (opthalmic ) and second division (maxillary ) of the 5th cranial nerve ,after that through superior orbital fissure to supplly somatic: Superior rectus (SR), inferior rectus (IR), inferior oblique (IO), medial rectus (MR).
 nerve lies in midbrain After leaving the brainstem, the nerve enters subarachnoid space and courses forward and laterally between posterior cerebral artery and superior cerebellar artery. At this level the nerve is compressed by Berry Aneurysms then the artery pass through cavernous sinus, together with trochelear 4th ,abducent 6th ,first division (opthalmic ) and second division (maxillary ) of the 5th cranial nerve ,after that through superior orbital fissure to supplly somatic: Superior rectus (SR), inferior rectus (IR), inferior oblique (IO), medial rectus (MR).")
5
and levator palpebrae superioris (LPS) as well as autonomic (pupillary sphincter and ciliary) muscles of the eye . Oculomotor nerve lesions : 1-In nuclear lesions in the midbrain; most common cause is stroke 2-Subarachnoid space is the most likely site of involvement in isolated IIIrd nerve palsies.the pathology may be compressive or infarction secondary to microvascular involvement in diabetics and hypertensives. Also compress by an aneurysm.

6
3-in cavernous sinus, one must note the associated
signs and symptoms. It may be associated with the dysfunction of IVth and VIth nerves, first or second division of trigeminal nerve most common cause is thrombosis and infection especially in diabetic

7
4-in the superior orbital fissure together with cranial nerves 4th ,6th and first division of trigeminal nerves associated with proptosis. Cavernous sinus syndrome The cavernous sinuses are paired, venous structures located on either side of the sella turcica, They receive venous tributaries from the superior and inferior orbital veins, The cavernous sinus contains the carotid artery, its sympathetic plexus, and the oculomovement nerves (third, fourth, and sixth cranial nerves). In addition, the ophthalmic branch and the maxillary branch of the fifth nerve traverse the cavernous sinus.
. In addition, the ophthalmic branch and the maxillary branch of the fifth nerve traverse the cavernous sinus.")
10
Clinical manifestation : ophthalmoplegia, chemosis, sometimes proptosis, trigeminal sensory loss in opthalmic and maxillary branches . Casuses 1- Cavernous sinus thrombosis is a serious condition that can follow infection of the face, paranasal sinuses (particularly the sphenoid sinus) or teeth most commonly in diabetic 2- metastases and nasopharyngeal carcinoma 3- aneurysms of the intracavernous portion of the carotid artery
 or teeth most commonly in diabetic. 2- metastases and nasopharyngeal carcinoma. 3- aneurysms of the intracavernous portion of the carotid artery.")
12
Jugular foramen syndrome
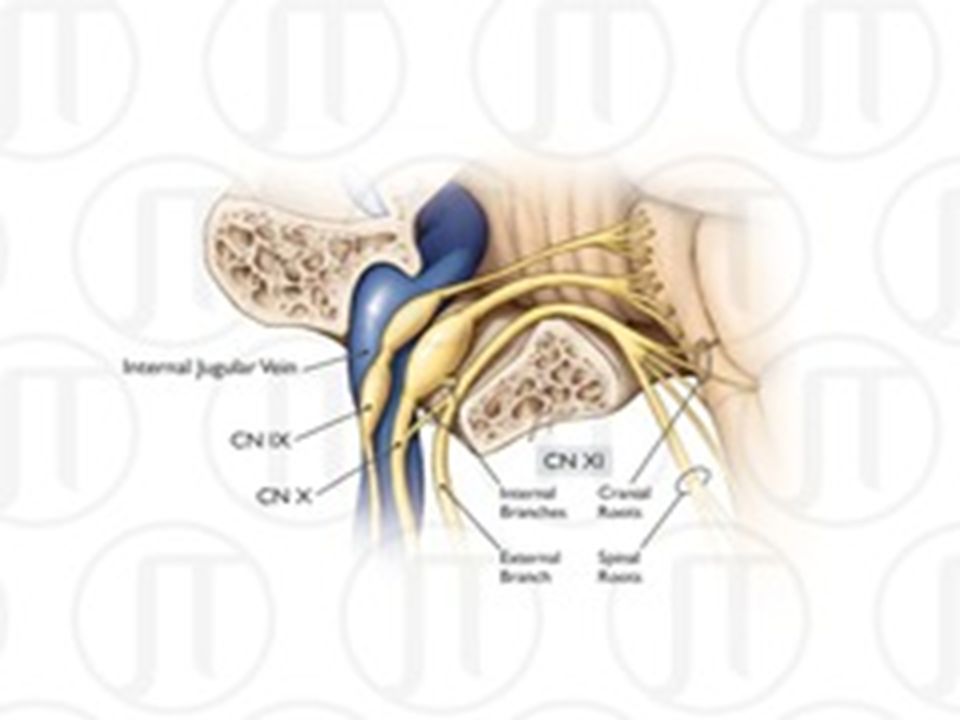
The jugular foramen is a large aperture in the base of the skull, Cranial nerves IX, X, and XI and the internal jugular vein pass through the jugular foramen. Clinical significance: is characterized by the paresis of (9th,10th&11th ) cranial nerves together so patient may complain from 1- dysphagia, dysphonia/hoarseness, 2- deviation of the uvula towards the normal side 3- sternocleidomastoid and trapezius muscles paresis Common Causes A- Metastatic tumors B- Infections
 cranial nerves together so patient may complain from. 1- dysphagia, dysphonia/hoarseness, 2- deviation of the uvula towards the normal side. 3- sternocleidomastoid and trapezius muscles paresis. Common Causes. A- Metastatic tumors. B- Infections.")
14
Bell’s palsy Bell’s palsy is an acute peripheral facial palsy, Bell’s palsy may occur in childhood; incidence increases steadily with age. There is no change in incidence with season, latitude or geography and no evidence for familial clustering. Weak associations may exist with diabetes and hypertension. A viral aetiology has been postulated on the basis that detection of herpes simplex virus type 1 (HSV-1) DNA in endoneurial fluid in most patients. Both primary HSV-1 infection and reactivation of latent infection have been implicated
 DNA in endoneurial fluid in most patients. Both primary HSV-1 infection and reactivation of latent infection have been implicated.")
18
Clinical features Rapid onset of facial weakness progressing over 48 hours (and occasionally up to 5 days) is preceded or accompanied by diffuse retro-auricular pain in the region of the mastoid, Facial weakness and asymmetry with drooling of liquids from the corner of the mouth on the affected side often lead the patient to suspect a stroke; most patients present promptly to primary care physicians. Not infrequently, patients mistakenly report that the contralateral unaffected side is the weak side. All facial muscles are usually equally affected., eye closure and blinking are reduced or absent (with a visible Bell’s phenomenon
 is preceded or accompanied by diffuse retro-auricular pain in the region of the mastoid, Facial weakness and asymmetry with drooling of liquids from the corner of the mouth on the affected side often lead the patient to suspect a stroke; most patients present promptly to primary care physicians. Not infrequently, patients mistakenly report that the contralateral unaffected side is the weak side. All facial muscles are usually equally affected., eye closure and blinking are reduced or absent (with a visible Bell’s phenomenon.")
20
attempted eye closure).
Ectropion formation may lead to overflow of tears on to the cheek. The angle of the mouth droops with reduction of the nasolabial fold, smoothing of skin wrinkles; the platysma muscle is also involved. The extent of maximal facial weakness is variable, but is severe in the majority, although occasionally patients present with very mild facial weakness

21
Loss of taste, often described as a muddy or metallic taste, and hyperacusis (because of paralysis of stapedius) indicate involvement of the chorda tympani and the branch to stapedius, Respectively Management and outcome Complete or almost complete recovery, without recurrence, over 3–8 weeks is the norm in at least 85% of cases, even without any treatment. Reassurance about the good prognosis is important. Inability to blink in severe facial weakness may lead to exposure keratitis and early evaluation should include

22
assessment of the eye. Lubricating eye drops are often required and patients should be shown how to tape the eye closed at night. Severe facial weakness with complete inability to close the eye requires urgent ophthalmological assessment; lateral tarsorrhaphy and/or temporary insertion of a gold weight into the upper lid may be necessary. Early treatment with oral steroids (prednisolon)and antiviral agents(oral acylovire) is worthy .
and antiviral agents(oral acylovire) is worthy ..")
Similar presentations











 in Drake et al.>")

















>")