Download presentation
Presentation is loading. Please wait.

2
Physiology of the Kidneys Body Fluids & Acid Base Balance MDC 2541 974-1548 jdietz@health.usf.edu John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

3
PHYSIOLOGY OF THE KIDNEYS BODY FLUID & ACID BASE BALANCE 2010 Suggested reading assignment: Berne and Levy, Chapter 2 (fluid compartments); Chapters 32-35 (Renal Physiology) and Chapter 36 (Acid Base Regulation) Dr. Dietz: Office - MDC 3538 Ph: 974-1548Email: jdietz@health.usf.edujdietz@health.usf.edu (Office – 3rd floor of the new research wing behind conference room MDC 3510)
.")
4
DATETIMETOPIC Fri., April 248:00-9:50BODY FLUID COMPARTMENTS BODY FLUID IMBALANCES Mon., April 278:00-9:50FILTRATION & CLEARANCE RENAL BLOOD FLOW Tues., April 281:00-2:50PROXIMAL TUBULE CONCENTRATION & DILUTION GLUCOSE, PAH, UREA Wed., April 298:00-9:50SODIUM EXCRETION WATER EXCRETION K+ EXCRETION Ca2+ & Mg2+ EXCRETION Schedule 2010 Fri., May. 18:00-9:50 RENAL HORMONES BODY FLUID REGULATION Mon., May. 48:00-9:50ACID BASE CHEMISTRY H+ EXCRETION Tues., May 51:00-1:50 ACID-BASE BALANCE Wed., May 68:00-9:50Clinical Correlation Dr. Bryan Bognar, Internal Medicine 11:00-11:50Clinical Correlation, Kidney/Acid Base Dr. Valerie Panzarino, Pediatric Nephrology Thurs. May 710:00-11:30Renal/Acid-Base Small Group Clinical Cases

5
Kidney function in disease states, with injury or transplantation, aging, ureteral obstruction, hypertension or hypotension. Clinical measurements of kidney function. Renal Tubular Acidosis (RTA): Types 1, 2 and 4. Effects of renal failure on blood volume, pressure, calcium balance, creatinine and urea, red cell production, acid – base status. Adrenal insufficiency. Changes in body fluid balances with changes in salt intake, I.V. solutions, over-hydration, dehydration, diarrhea and/or vomiting, heart failure, hemorrhage. Hyper- and hypokalemia. Edema formation. Diabetes Insipidus. Acute Renal Failure Glucose handling by the kidneys in diabetes mellitus. Syndrome of Inappropriate ADH secretion. Mechanisms of action for diuretics. Renovascular Hypertension. Acid – Base Disorders: metabolic acidosis, metabolic alkalosis, respiratory acidosis, respiratory alkalosis, mixed acid-base disturbances. Some relevant clinical concepts discussed in this section of the course
: Types 1, 2 and 4. Effects of renal failure on blood volume, pressure, calcium balance, creatinine and urea, red cell production, acid – base status. Adrenal insufficiency. Changes in body fluid balances with changes in salt intake, I.V. solutions, over-hydration, dehydration, diarrhea and/or vomiting, heart failure, hemorrhage. Hyper- and hypokalemia. Edema formation. Diabetes Insipidus. Acute Renal Failure Glucose handling by the kidneys in diabetes mellitus. Syndrome of Inappropriate ADH secretion. Mechanisms of action for diuretics. Renovascular Hypertension. Acid – Base Disorders: metabolic acidosis, metabolic alkalosis, respiratory acidosis, respiratory alkalosis, mixed acid-base disturbances. Some relevant clinical concepts discussed in this section of the course.")
6
RENAL WWW RESOURCES - 2009 Genetic abnormalities in renal transporters: http://www.merck.com/mmpe/sec17/ch237/ch237a.html/ The Merk Manual Chapter on Water, Electrolytes and Acid-Base: http://www.merck.com/mmpe/sec12/ch156/ch156a.html Fluid Physiology: http://www.anaesthesiamcq.com/FluidBook/ Renal Pathology: http://www.uncnephropathology.org/jennette/tutorial.htm http://www-medlib.med.utah.edu/WebPath/RENAHTML/RENALIDX.html http://www.kidneyatlas.org/ Urinalysis: http://www-medlib.med.utah.edu/WebPath/TUTORIAL/URINE/URINE.html Online Practice Tests: http://www.medstudysites.com/Human-Physiology/physiology-exams.php http://academic.pgcc.edu/~aimholtz/AandP/PracticeQuestions/Urinary/urinaryq1.html http://kobiljak.msu.edu/cai/psl501/50196e5q.htm http://www.acbrown.com/kidney/Instructions/RnPQst.htm Renal Physiology Objectives: http://www.the-aps.org/education/MedPhysObj/renal.htm Several Reviews of Renal Physiology: http://mcb.berkeley.edu/courses/mcb136/topic/Kidney_Body_Fluids/ http://www.nda.ox.ac.uk/wfsa/html/u09/u09_016.htm http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/K/Kidney.html http://en.wikipedia.org/wiki/Renal_physiology http://www.acid-base.com/physiology.php Acid-Base Calculator: http://www.health.adelaide.edu.au/paed-anaes/javaman/Respiratory/a-b/ABvalidation.htm Acid-Base cases online: http://www.anaesthesiamcq.com/EduResources/Gases/GasArchive.php Fluid balance in space: http://www.nsbri.org/HumanPhysSpace/introduction/intro-bodychanges.html

7
Medical Physiology Course Outline Cell Transport Excitable Membranes Respiration Acid Base Kidney Heart & Circulation Endocrinology

8
Where are we going ? Fluid compartments iv solutions disturbances Filtration/ blood flow normal Pathophys Reabsorption Salt/water regulation Reabsorption Na/K/Ca urea General Fluid Regulation How the kidneys fit with everything else Acid Base Regulation How the kidneys and lungs work together

9
Body Fluid Compartments Normal Compartment Volumes Changes with I.V. Solutions Pathophysiological changes Molarity vs Osmolarity Osmotic Pressure Membrane Permeability (cell vs capillary)
.")
10
BODY FLUIDS At the end of this section you should know: Normal volumes for the basic fluid compartments as Liters or as a % of body weight. Solute concentrations of the basic compartments. How compartments are measured. How various i.v. solutions affect the different fluid compartments. How changes in fluid intake or output affect the different fluid compartments. How to calculate precise changes in fluid volumes and use the DY diagrams.

11
THREE EMERGENCY ROOM PATIENTS 80 year old male with AD - over medicated because of irritability and has had nothing to drink for 3 days. 3 week old infant with vomiting and diarrhea for 2 days. Gunshot wound - loss of 2 liters of blood.

12
BODY FLUIDS DISTRIBUTION: Total body water (TBW) varies from 50-70% of body weight (ave. = 60%). In an average person (70Kg) this is: 0.6 X 70Kg = 42Kg or 42L
. In an average person (70Kg) this is: 0.6 X 70Kg = 42Kg or 42L.")
13
PERCENTAGE OF WATER IN TISSUES

14
Intracellular (ICF): 40% of Bd. Wt. 28L Extracellular (ECF): 20% of Bd. Wt. 14L Plasma: 4-5% of Bd. Wt. 20% of ECF

15
MEASURING THE SIZE OF COMPARTMENTS Standard Equation Compartment Volume = Amount Injected Final Concentration

16
Molar and Equivalent Concentrations HCO 3 -

17
Osmolality: millimoles of solute/Kg of H 2 O; Osmolarity: millimoles of solute/L of H 2 O Activity of H 2 O decreases as Osmolality increases. Colligative Properties of Solutions: Depend on number of molecules and not on their nature. Osmolality A B Boiling Point Freezing Point Vapor Pressure Osmotic Pressure

18
APPROXIMATE IONIC COMPOSITION OF THE BODY WATER COMPARTMENTS

19
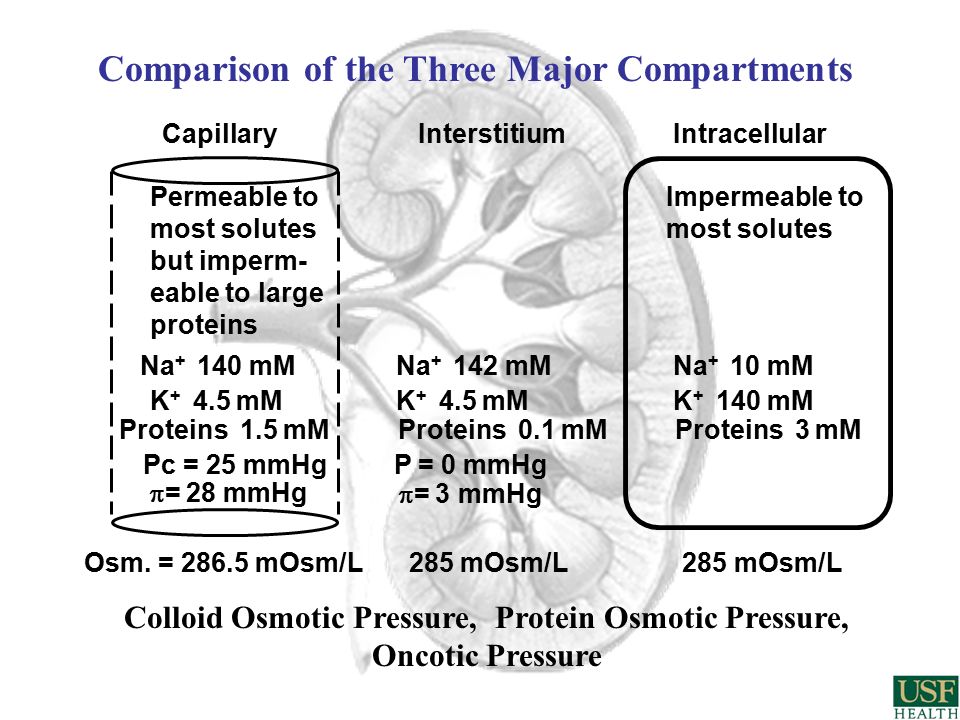
CapillaryInterstitiumIntracellular Na + 140 mMNa + 142 mMNa + 10 mM K + 4.5 mM K + 140 mM Proteins 1.5 mM Proteins 0.1 mM Proteins 3 mM Osm. = 286.5 mOsm/L 285 mOsm/L 285 mOsm/L Pc = 25 mmHg P = 0 mmHg = 28 mmHg = 3 mmHg Permeable to most solutes but imperm- eable to large proteins Impermeable to most solutes Comparison of the Three Major Compartments Colloid Osmotic Pressure, Protein Osmotic Pressure, Oncotic Pressure

20
CHANGES IN BODY FLUID COMPARTMENT VOLUMES

21
“The total body content of sodium is the principal determinant of extracellular and intravascular fluid volume” Na + & anions – Extracellular K + & anions – Intracellular D 5 W = Water – adds no effective osmoles At equilibrium, osmolality is the same in all compartments Calculate TBW first, then ECF and ICF

22
Problem We infuse 1 liter of D5W (5% Dextrose in water). How many total osmoles have we infused? What is the new osmolality after infusion?

23
Add 1 Liter of D5W = Water TBWECFICF

24
Add 1 Liter of D5W = Water TBWECFICF Glucose is metabolized so no osmoles are added.

25
Add 1 Liter of D5W = Water TBWECFICF

26
Add 1 Liter of D5W = Water TBWECFICF

27
Add 1 Liter of D5W = Water TBWECFICF

28
Add 1 Liter of D5W = Water TBWECFICF 1/3 ECF and 2/3 ICF

29
Addition of 1 L of H 2 O

30
CapillaryInterstitiumIntracellular Na + 140 mMNa + 142 mMNa + 10 mM K + 4.5 mM K + 140 mM Proteins 1.5 mM Proteins 0.1 mM Proteins 3 mM Osm. = 286.5 mOsm/L 285 mOsm/L 285 mOsm/L Pc = 25 mmHg P = 0 mmHg = 28 mmHg = 3 mmHg Permeable to most solutes but imperm- eable to large proteins Impermeable to most solutes Comparison of the Three Major Compartments Colloid Osmotic Pressure, Protein Osmotic Pressure, Oncotic Pressure

31
Problem We infuse 1 liter of normal saline (0.9%) of 0.150M How many total osmoles have we infused? What is the new osmolality after infusion?

32
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF
 TBWECFICF")
33
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF 0.150M NaCl = 150 mM Na + & 150 mM Cl - in 1 L so there are 300 mOsm total solute added as an isotonic solution
 TBWECFICF 0.150M NaCl = 150 mM Na + & 150 mM Cl - in 1 L so there are 300 mOsm total solute added as an isotonic solution")
34
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF
 TBWECFICF")
35
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF
 TBWECFICF")
36
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF
 TBWECFICF")
37
Add 1 Liter of Normal Saline 0.150M (0.9%) TBWECFICF
 TBWECFICF")
38
Add 1 L of normal saline (0.9%) or 0.150M or 150 mM or 300 mOsm/L
 or 0.150M or 150 mM or 300 mOsm/L")
39
CapillaryInterstitiumIntracellular Na + 140 mMNa + 142 mMNa + 10 mM K + 4.5 mM K + 140 mM Proteins 1.5 mM Proteins 0.1 mM Proteins 3 mM Osm. = 286.5 mOsm/L 285 mOsm/L 285 mOsm/L Pc = 25 mmHg P = 0 mmHg = 28 mmHg = 3 mmHg Permeable to most solutes but imperm- eable to large proteins Impermeable to most solutes Comparison of the Three Major Compartments Colloid Osmotic Pressure, Protein Osmotic Pressure, Oncotic Pressure

40
Problem We infuse 2 Liters of a 0.45% solution of NaCl. How many total osmoles have we infused? What is the new osmolality after infusion?

41
Problem We infuse 2 Liters of a 0.45% solution of NaCl. How many total osmoles have we infused? What is the new osmolality after infusion?

42
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF
 TBWECFICF")
43
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF 0.075M NaCl = 75 mM Na + & 75 mM Cl - but 2 L so there are 300 mOsm total added as a hypotonic solution
 TBWECFICF 0.075M NaCl = 75 mM Na + & 75 mM Cl - but 2 L so there are 300 mOsm total added as a hypotonic solution")
44
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF
 TBWECFICF")
45
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF
 TBWECFICF")
46
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF
 TBWECFICF")
47
Add 2 Liter of Half-Normal Saline (0.45%) TBWECFICF
 TBWECFICF")
48
Problem What would you expect to happen to fluid compartments if we infuse KCl?

49
Fluids Commonly Lost

50
LOSS OF GI FLUIDS

52
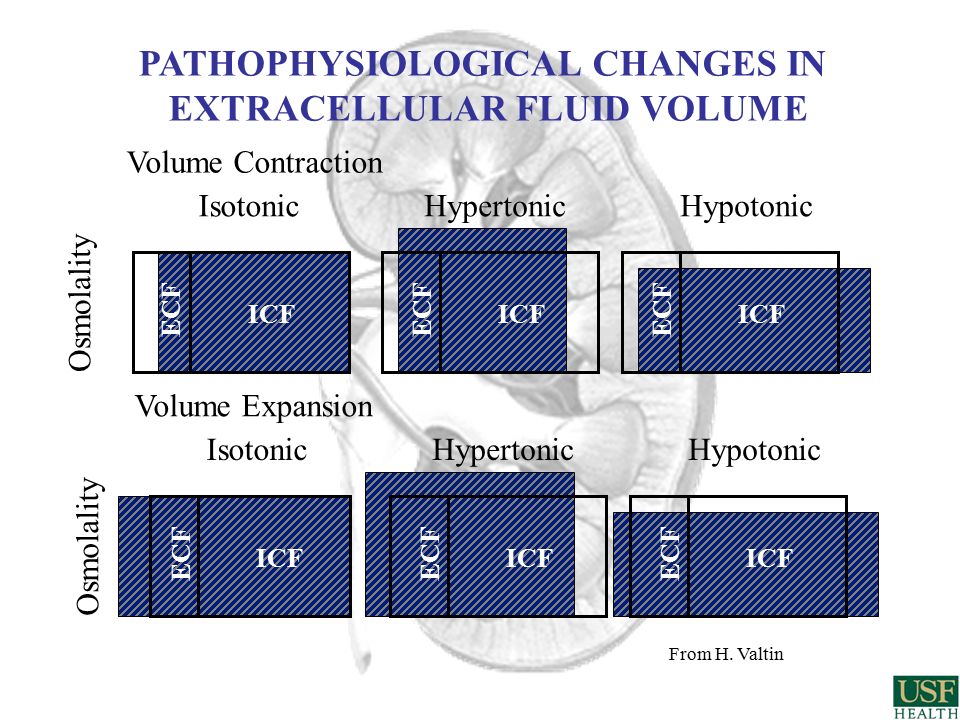
Volume Contraction IsotonicHypertonicHypotonic ECF ICF ECF ICF Osmolality Volume Expansion IsotonicHypertonicHypotonic ECF ICF ECF ICF ECF ICF Osmolality From H. Valtin ICF PATHOPHYSIOLOGICAL CHANGES IN EXTRACELLULAR FLUID VOLUME

53
80 year old male with AD - over medicated because of irritability and has had nothing to drink for 3 days. 3 week old infant with vomiting and diarrhea for 2 days. Gunshot wound - loss of 2 liters of blood. THREE EMERGENCY ROOM PATIENTS

54
CapillaryInterstitiumIntracellular Na + 140 mMNa + 142 mMNa + 10 mM K + 4.5 mM K + 140 mM Proteins 1.5 mM Proteins 0.1 mM Proteins 3 mM Osm. = 286.5 mOsm/L 285 mOsm/L 285 mOsm/L Pc = 25 mmHg P = 0 mmHg = 28 mmHg = 3 mmHg Permeable to most solutes but imperm- eable to large proteins Impermeable to most solutes Comparison of the Three Major Compartments Colloid Osmotic Pressure, Protein Osmotic Pressure, Oncotic Pressure

55
Glomerular Filtration Glomerular Capillary Starling Forces (review from CV) Filtration as bulk flow (both ions and water) Clearance (volume of plasma/time) John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida, College of Medicine

56
POP QUIZ Which of the following are true concerning fluid compartments (Answer True or False)? A. ECF is 2/3 of total body water (TBW). B. The major ECF cation is Na+. C. A normal saline infusion increases ECF volume but decreases ICF volume. D. Hypertonic NaCl infusion increases ECF volume but decreases ICF volume. E. Plasma volume = the distribution of water minus the distribution of Na+. F ? ? ? ? ? F F T T
. B. The major ECF cation is Na+. C. A normal saline infusion increases ECF volume but decreases ICF volume. D. Hypertonic NaCl infusion increases ECF volume but decreases ICF volume. E. Plasma volume = the distribution of water minus the distribution of Na+. F . F F T T.")
57
Glomerular Filtration At the end of this section you should know: the arrangement of the renal arterioles, capillary beds, tubular segments renal innervation. how glomerular capillaries and filtration forces compare to other capillary beds how GFR is affected by physiological and pathophysiological conditions. how GFR is measured clinically using creatinine and what is meant by renal "clearance". how GFR can change in disease or aging and by compensatory hypertrophy.

58
Renal Failure Patient Patient Data (Plasma)Change from Normal K + Phosphate Calcium Sulfate Urea Hematocrit Blood Pressure Bicarbonate pH
Change from Normal K + Phosphate Calcium Sulfate Urea Hematocrit Blood Pressure Bicarbonate pH ")
59
FUNCTIONS OF THE KIDNEYS Remove wastes. Reg. Vol. and Composition of ECF. Acid-Base Balance. Blood Pressure Regulation. Removal of Foreign Substances. RBC Production. Vitamin D Activity.

60
Proximal Tubule Distal Tubule Thin descending Thin ascending Loop of Henle Thick ascending (diluting segment) Early Late Collecting Duct Cortical Medullary
 Early Late Collecting Duct Cortical Medullary")
61
Blood Supply to the Kidneys Glomerular capillaries Peritubular capillaries Vasa recta Note the 3 capillary beds: Afferent Arteriole Efferent Arteriole

62
Blood Supply to the Kidneys

63
Innervation of the Kidneys Sympathetic Afferent & Efferent Arterioles Juxtaglomerular cells Tubule

64
Basic Theory of Urine Formation Filtration Reabsorption Secretion Excretion

65
Organ to Cellular to Molecular

66
Glomerular Filtration Production of a protein - free filtrate of plasma

67
THE GLOMERULAR MEMBRANE Three Sieves in Series Capillary Endothelium Basement Membrane Bowman’s Capsule Epithelium (podocytes)
")
68
Permeability Based on Molecular Size

70
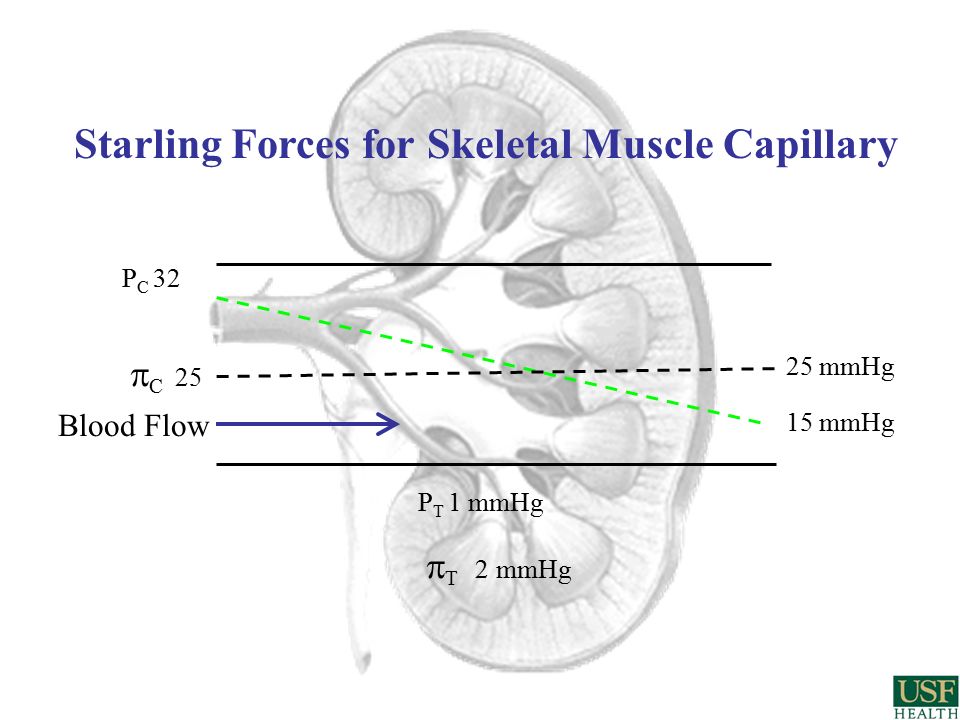
Starling Forces for Skeletal Muscle Capillary P C 32 P T 1 mmHg C 25 T 2 mmHg 15 mmHg 25 mmHg Blood Flow

71
Starling Forces Across the Glomerular Capillary GFR = 125 ml/min = 180 L/day NFP = 10 - 12 mmHg outward P GC 60 P BC 15 mmHg GC 25 BC 0 mmHg 58 mmHg 35 mmHg Blood Flow

72
Filtration Coefficient (Kf) Permeability Surface Area
 Permeability Surface Area")
73
P GC 60 P BC 15 mmHg GC 25 BC 0 mmHg 58 mmHg 35 mmHg Blood Flow Regulation of GFR

74
Changes in Kf (Permeability or Surface area): Mesangial Cell Contraction or Relaxation + ANP, NO - AII, Endothelin, Norepi, Epi, ADH
: Mesangial Cell Contraction or Relaxation + ANP, NO - AII, Endothelin, Norepi, Epi, ADH")
75
A volume of plasma from which a substance is completely removed by the kidneys per unit time. Clearance Where UF = urine flow; Ux = urine concentration of X; Px = plasma concentration of X; Cx = clearance of X C x = UF U x = Volume/Time eg. ml/min or L/day P x

76
Freely FilteredNot Metabolized Not ReabsorbedDoes Not Change GFR Not Secreted Not Produced Measurement of GFR (Inulin M.W. = 5,000) Amount Filtered = Amount Excreted GFR · P IN = UF ·U IN GFR = UF ·U IN = C IN P IN (Filtered Inulin = Excreted Inulin) Excreted Inulin Plasma Inulin (volume/time)
 Amount Filtered = Amount Excreted GFR · P IN = UF ·U IN GFR = UF ·U IN = C IN P IN (Filtered Inulin = Excreted Inulin) Excreted Inulin Plasma Inulin (volume/time).")
77
1 ?1 Inulin in the Kidney Renal Plasma Flow (RPF) = 600 RPF = 475 GFR = 125 I = 1 I = RPF = 599 Peritubular Capillaries Salts & Water Reabsorbed but no Inulin Reabsorbed Vasa Recta Capillaries Salts & Water Reabsorbed but no Inulin Reabsorbed Renal Artery Renal Vein Urine Flow = 1 - 5 I = 50 -100 (All flows are in ml/min) (I = Inulin concentration in mg/dl) RPF = 415 RPF = 60 Glomerulus ? 0.8?
78
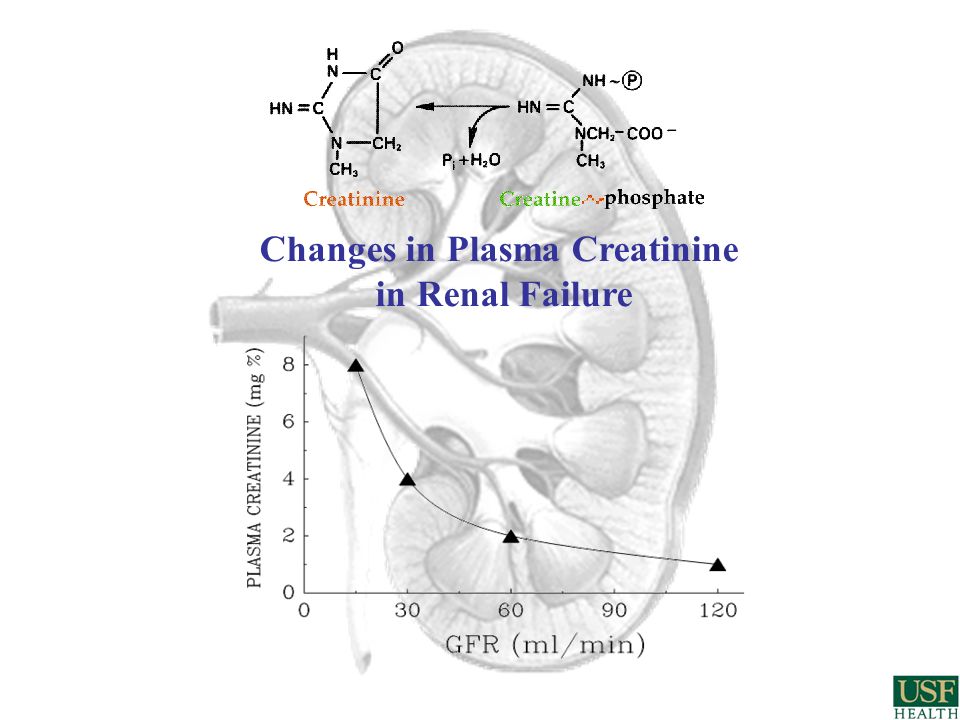
Changes in Plasma Creatinine in Renal Failure

79
Compensatory Hypertrophy 1) Changes in GFR a. Disease b. Transplantation 2) Changes in GFR with age “The Four Stages of Life”
 Changes in GFR with age The Four Stages of Life .")
80
Changes in GFR in Chronic Renal Disease

81
Daily Creatinine Excretion Production varies based on weight & gender Excretion equals creatinine production Excretion can be normal even in renal disease GFR = UF ·U creatinine (Creatinine Excretion) P Creatinine
 P Creatinine")
82
Problem: 24 hour urine collection for GFR 1. Tell patient to go home and collect all urine in container provided. 2. Patient goes home. Patient pees in container. 3. Patient goes to Walmart to buy dental floss, uses store restroom. 4. Patient goes home. Patient pees in container. Etc. 5. Patient gets up at 3:00am and uses toilet. 6. Next day: Patient returns container to office. Draw a blood sample. Volume collected – 1,800 ml (normal range) Collection time – 24 hours Urine creatinine = 70 mg/dl (normal range) Plasma creatinine = 1.4 mg/dl (high end of normal) Creatinine Clearance (GFR) = Should you order a renal biopsy? calculated as 90 L/day or 62 ml/min.
 Collection time – 24 hours Urine creatinine = 70 mg/dl (normal range) Plasma creatinine = 1.4 mg/dl (high end of normal) Creatinine Clearance (GFR) = Should you order a renal biopsy. calculated as 90 L/day or 62 ml/min..")
83
Daily Creatinine Excretion Normal PersonKidney disease Creatinine (Cr) Production (1mg/minute) Plasma Cr = 1 mg/dl Plasma Cr = 4 mg/dl Amount of Filtered Cr = 1 mg/minute Amount of Filtered Cr = 1 mg/minute Volume Filtered 25 ml/min [Cr] = 4 mg/dl Volume Filtered 100 ml/min [Cr] = 1 mg/dl Amount of Excreted Cr = 1 mg/minute Amount of Excreted Cr = 1 mg/minute Recall that all of the filtered Creatinine is excreted. Blame Tania Condarco
![Daily Creatinine Excretion Normal PersonKidney disease Creatinine (Cr) Production (1mg/minute) Plasma Cr = 1 mg/dl Plasma Cr = 4 mg/dl Amount of Filtered Cr = 1 mg/minute Amount of Filtered Cr = 1 mg/minute Volume Filtered 25 ml/min [Cr] = 4 mg/dl Volume Filtered 100 ml/min [Cr] = 1 mg/dl Amount of Excreted Cr = 1 mg/minute Amount of Excreted Cr = 1 mg/minute Recall that all of the filtered Creatinine is excreted.](http://images.slideplayer.com/37/10685824/slides/slide_83.jpg "Blame Tania Condarco.")
84
RENAL BLOOD FLOW (RBF) NORMAL = 1200-1300ml/min. (both kidneys) = 20-25% of C. O. RENAL PLASMA FLOW (RPF) = RBF (1-hematocrit) = 600-700 ml/min. (both kidneys) FILTRATION FRACTION (FF) =GFR/RPF = 125ml/min/650 ml/min = 20 % Regulation of Blood Flow (review of CV) Clearance (again?) John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine
 = RBF (1-hematocrit) = ml/min. (both kidneys) FILTRATION FRACTION (FF) =GFR/RPF = 125ml/min/650 ml/min = 20 % Regulation of Blood Flow (review of CV) Clearance (again ) John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine.")
85
At the end of this section you should know: the distribution of renal blood flow, extra-renal RBF regulation and autoregulation. how renal plasma flow (RPF) is measured using clearance. how to calculate RBF, RPF and Filtration Fraction (FF). how renal oxygen consumption is effected by changes in RBF or GFR. RENAL BLOOD FLOW (RBF)
 is measured using clearance. how to calculate RBF, RPF and Filtration Fraction (FF). how renal oxygen consumption is effected by changes in RBF or GFR. RENAL BLOOD FLOW (RBF).")
87
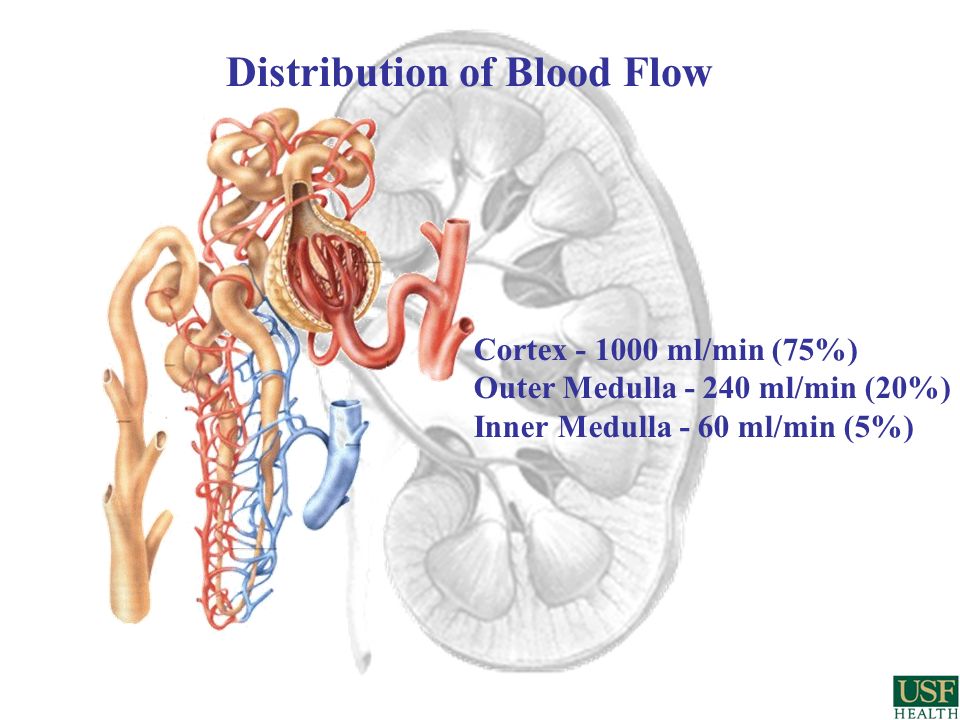
Distribution of Blood Flow Cortex - 1000 ml/min (75%) Outer Medulla - 240 ml/min (20%) Inner Medulla - 60 ml/min (5%)
 Outer Medulla ml/min (20%) Inner Medulla - 60 ml/min (5%)")
88
Measurement of Renal Plasma Flow (RPF) (Fick Method) X Artery / min = (X Vein / min) + (X Ureter / min) RPF (ml/min) · [ X] Artery = (RPF (ml/min) · [X] Vein ) + (UF (ml/min) · [X] Ureter ) RPF = UF · U X (X Artery - X Vein ) RPF = UF · U X P X RPF = ERPF (C PAH ) 0.9 If X Vein = 0 then C PAH = UF · U PAH = ERPF P PAH Infuse a substance in a patient to achieve a steady plasma concentration
![Measurement of Renal Plasma Flow (RPF) (Fick Method) X Artery / min = (X Vein / min) + (X Ureter / min) RPF (ml/min) · [ X] Artery = (RPF (ml/min) · [X] Vein ) + (UF (ml/min) · [X] Ureter ) RPF = UF · U X (X Artery - X Vein ) RPF = UF · U X P X RPF = ERPF (C PAH ) 0.9 If X Vein = 0 then C PAH = UF · U PAH = ERPF P PAH Infuse a substance in a patient to achieve a steady plasma concentration](http://images.slideplayer.com/37/10685824/slides/slide_88.jpg "Measurement of Renal Plasma Flow (RPF) (Fick Method) X Artery / min = (X Vein / min) + (X Ureter / min) RPF (ml/min) · [ X] Artery = (RPF (ml/min) · [X] Vein ) + (UF (ml/min) · [X] Ureter ) RPF = UF · U X (X Artery - X Vein ) RPF = UF · U X P X RPF = ERPF (C PAH ) 0.9 If X Vein = 0 then C PAH = UF · U PAH = ERPF P PAH Infuse a substance in a patient to achieve a steady plasma concentration")
89
PAH in the Kidney RPF = 600 RPF = 475 GFR = 125 PAH = 1 RPF = 599 Peritubular Capillaries Salts & Water Reabsorbed /no PAH Reabsorbed/ PAH secreted into tubule Vasa Recta Capillaries Salts & Water Reabsorbed but no PAH Reabsorbed or Secreted Renal Artery Renal Vein Urine Flow = 1 - 5 PAH = 300-600 (All flows are in ml/min) (PAH = para-aminohippurate concentration in mg/dl) RPF = 415 RPF = 60 Glomerulus PAH = 1 PAH = 0 PAH = 0.1
 (PAH = para-aminohippurate concentration in mg/dl) RPF = 415 RPF = 60 Glomerulus PAH = 1 PAH = 0 PAH = 0.1")
90
Typical Clearance Values PAH (p-amino-hyppurate) 650 ml/min Creatinine130 ml/min Inulin125 ml/min Urea55 ml/min Na+2 ml/min H 2 O1 ml/min glucose0 ml/min Albumin0 ml/min
 650 ml/min Creatinine130 ml/min Inulin125 ml/min Urea55 ml/min Na+2 ml/min H 2 O1 ml/min glucose0 ml/min Albumin0 ml/min")
91
Blood Pressure Intrinsic: autoregulation 1. Myogenic 2. Tubuloglomerular feedback prostaglandins Extrinsic: nerves hormones Control of Renal Blood Flow

92
Renal Oxygen Consumption:

93
POP QUIZ Which of the following are true concerning renal filtration and blood flow (Answer True or False)? A. Glomerular capillary hydrostatic pressure is lower than that of muscle capillaries. B. GFR can be measured by the clearance of creatinine. C. Afferent arteriole dilation will decrease GFR. D. Sympathetic stimulation will decrease RBF and GFR. E. A decrease in blood pressure from 100 to 80 mmHg will result in a proportional decrease in RBF. F ? ? ? ? ? F F T T

94
Filtration Reabsorption - NFP + NFP - NFP Starling Forces Ion channels & Transporters Cell Membrane Permeability Concentration gradients Osmolality REABSORPTION

95
At the end of this section you should know: the mechanisms for an isotonic reabsorption of fluid in the PT. (i.e. permeability, active and passive transporters). the role of peritubular capillaries in PT reabsorption. how active Na+ transport provides the driving force for reabsorption. how inulin can be used as a marker for water reabsorption in the tubule. how glucose and a.a. are reabsorbed by secondary active transport. PROXIMAL TUBULE
. the role of peritubular capillaries in PT reabsorption. how active Na+ transport provides the driving force for reabsorption. how inulin can be used as a marker for water reabsorption in the tubule. how glucose and a.a. are reabsorbed by secondary active transport. PROXIMAL TUBULE.")
96
General Reabsorption in the Tubule

97
1,500 g 6 g Renal Handling of Salt Filtration Excretion

98
PROXIMAL TUBULE

99
Proximal Tubule Reabsorption Early Late

100
Proximal Tubule Reabsorption

101
PROXIMAL TUBULE SUMMARY 2/3 of salts and water reabsorbed All glucose and a.a. reabsorbed Reabsorption is isotonic: PT Osmolality is isotonic at the beginning & the end

102
CONCENTRATION & DILUTION Loop of Henle & Collecting Duct Permeability and Solute Transport in the John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

103
CONCENTRATION & DILUTION At the end of this section you should know: permeability aspects of the Loop of Henle, DT & CD. the importance of the high medullary interstitial osmolality. the reabsorption of Na+, Cl-, urea and water in the Loop, DT and CD. changes in osmolality along the tubule and actions of ADH on the CD.

104
300 1200 900 400 500 600 700 800 1100 1000
105
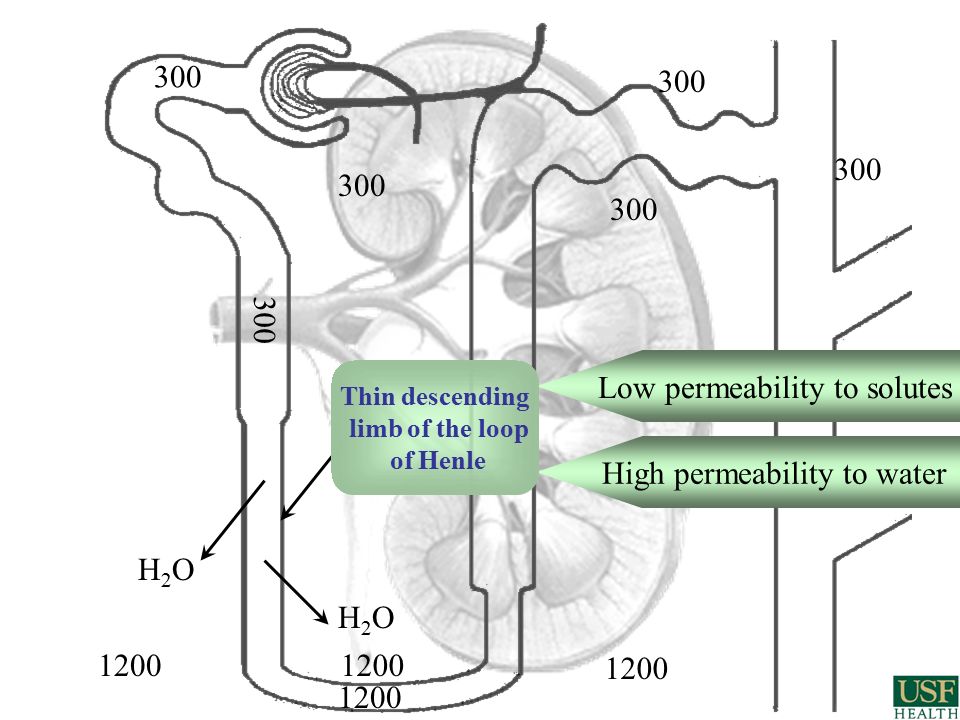
300 1200 Low permeability to solutes High permeability to water H2OH2O H2OH2O 1200 Thin descending limb of the loop of Henle

106
300 1200 permeable to solutes H2OH2O H2OH2O Thin ascending limb of the loop of Henle low permeability to H 2 O NaCl Urea

107
300 1200 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 150 Thick Ascending limb of the loop of Henle (TAL) Diluting segment impermeable to H 2 O Special carriers co-transport ions from tubule to interstitium Na + K+K+ 2 Cl - Na + K+K+ 2 Cl -
 Diluting segment impermeable to H 2 O Special carriers co-transport ions from tubule to interstitium Na + K+K+ 2 Cl - Na + K+K+ 2 Cl -")
108
300 1200 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 150 Distal Tubule Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - Impermeable to H 2 O Special carriers co-transport ions from tubule to interstitium 60 NaClNaCl

109
300 1200 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 150 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 60 NaClNaCl Cortical Collecting Duct 1200 H2OH2O H2OH2O H2OH2O H2OH2O Medullary Collecting Duct Variable permeability to H 2 O Regulated by Antidiuretic Hormone (ADH)
")
110
Antidiuretic Hormone (ADH) Arginine Vasopressin (AVP) Plasma Osmolality (osmorecptors) Blood Pressure (baroreceptors) Kidney V 2 receptor H 2 O reabsorption Collecting Duct Arterioles V 1 receptor Vasoconstriction
 Arginine Vasopressin (AVP) Plasma Osmolality (osmorecptors) Blood Pressure (baroreceptors) Kidney V 2 receptor H 2 O reabsorption Collecting Duct Arterioles V 1 receptor Vasoconstriction")
111
Collecting Duct ADH cAMP Lumen (hypotonic) Interstitium (hypertonic) V 2 H 2 O
 Interstitium (hypertonic) V 2 H 2 O")
113
Summary of ADH Actions on the Kidneys Increases permeability of entire Collecting Duct to Water. Increases permeability of Medullary CD to Urea. Decreases Vasa Recta blood flow. Increases expression of the Na/K/2Cl transporter in the TAL. ?Question? How can each of these effects increase the concentration of the urine?

114
300 1200 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 150 Na + K+K+ 2 Cl - Na + K+K+ 2 Cl - 60 NaClNaCl 1200 H2OH2O H2OH2O H2OH2O H2OH2O H2OH2O H2OH2O

115
High medullary interstitial osmolality Reabsorption of Na + and Cl - in the thick ascending limb (diluting segment). Low flow through vasa recta. Counter current multiplication. Counter current exchange. Importance of urea.

116
300 - The Counter Current Multiplier 300 100 500 H2OH2O H2OH2O 300 500 300 700 50

117
Counter Current Exchange (a function of the vasa recta capillaries) Na+, Cl- & Urea out Na+, Cl- & Urea in
 Na+, Cl- & Urea out Na+, Cl- & Urea in")
118
A Simple Counter Current Exchanger Bath B Bath A Which bath will stay warm longer ? The tube of cold water carries heat away from the bath.

119
Loop Diuretics

120
Numbers in ( ) refer to the volume of filtrate in ml/min remaining to be reabsorbed
 refer to the volume of filtrate in ml/min remaining to be reabsorbed")
121
Renal Regulation of Special Substances Urea, Glucose, Phosphate, Sulfate, Water, Sodium, Potassium & Calcium John R. Dietz Physiology & Biophysics University of South Florida College of Medicine

122
Renal Regulation of Special Substances (Urea, Glucose, Phosphate & Sulfate) At the end of this section you should know: How urea is reabsorbed. Principles of secondary active transport and how it applies to carrier mediated secretion and reabsorption. Transport maximum and how it is calculated. Renal handling of glucose in diabetes.

123
Reabsorption of Urea 50% of Filtered Urea Reabsorbed 4 5 30 100 500 600 Tubular Concentrations of Urea are in mmoles/L Maximal ADH H2OH2O H2OH2O H2OH2O H2OH2O

124
Reabsorption of Glucose in the Proximal Tubule LumenBasal Membrane Na + K+K+ Glucose Na + SGLT 1 GLUT 2

125
Glu Sodium Powered Secondary Active Transport Na + Lumen Cell Membrane Stanley J. Nazian, Ph..D., This slide was stolen without remorse from Na + Glu

126
Reabsorption of Glucose in the Proximal Tubule Lumen Capillary Na + K+K+ Glucose Na + SGLT 1 GLUT 2

127
Facilitated Diffusion Interstitium Cell Membrane Glu

128
Secondary Active Transport

129
Reabsorption of Glucose Excreted Filtered Reabsorbed Excreted = Filtered - Reabsorbed 2 3 1

131
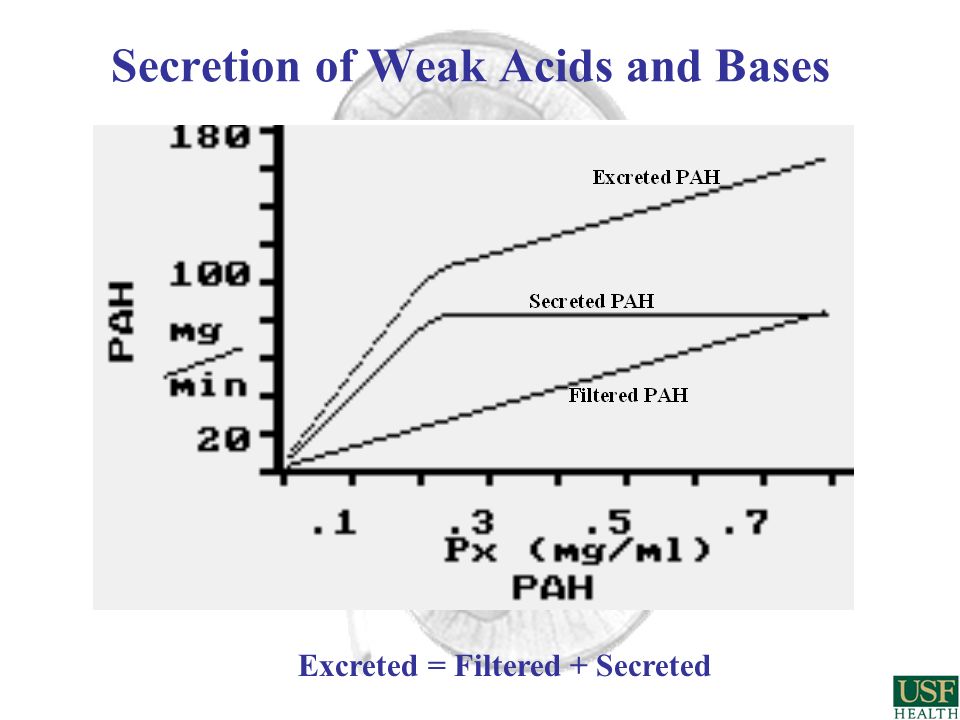
Secretion of Weak Acids and Bases Excreted = Filtered + Secreted

132
Fanconi’s Syndrome hyperaminoaciduria glucoseuria hyperphosphaturia hypersulfaturia bicarbonaturia natriuresis severe water loss

133
POP QUIZ Which of the following are true concerning renal tubular absorption (Answer True or False)? A. Most of the filtrate is absorbed in the thick ascending limb of the loop of Henle. B. Fluid leaving the Proximal Tubule is iso-osmotic to plasma. C. Renal medulary hyperosmolality is dependent on mainly passive mechanisms. D. Most reabsorption in the renal tubules is directly or indirectly dependent on Na/K APTase. E. ADH increases water absorption in most parts of the renal tubule. F ? ? ? ? ? F F T T

134
ANGIOTENSIN II SYMPATHETICS ALDOSTERONE HEMODYNAMICS ANP PROTEIN OSMOTIC PRESSURE Regulation of Na+ Excretion John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

135
At the end of this section you should know how each of the following affect Sodium reabsorption: Blood pressure GFR Aldosterone Angiotensin II atrial natriuretic peptide (ANP) and BNP Protein osmotic pressure Renal nerves (epinephrine or norepinephrine. Renal Regulation of Special Substances (Sodium and Chloride)
.")
137
Sodium (Na) Natriuretic? Egyptian valley: Wadi El-Natron Natrium (Lt.) from Natrum (Gr.) from Egyptian - Natron increases sodium excretion
 from Natrum (Gr.) from Egyptian - Natron increases sodium excretion.")
138
Regulation of Na+ Excretion Decreases in GFR decrease Na+ Excretion Changes in Filtration Pressure with decreased blood pressure. Changes in Permeability: (Mesangial Cell Contraction or Relaxation) + ANP, NO - AII, Endothelin, Norepi, Epi, ADH
 + ANP, NO - AII, Endothelin, Norepi, Epi, ADH.")
139
Atrial Natriuretic Peptide (Factor) ANP (ANF) Decreases Na + Reabsorption Regulation of Na+ Excretion Medullary Collecting Duct Na + ANP (or BNP) cGMP Lumen Capillary Na + K + X
 ANP (ANF) Decreases Na + Reabsorption Regulation of Na+ Excretion Medullary Collecting Duct Na + ANP (or BNP) cGMP Lumen Capillary Na + K + X")
140
Electron Micrograph of Rat Atrium J. D. Jamieson; G. E. Palade The Journal of Cell Biology, Vol. 23, No. 1. (Oct., 1964), pp. 151-172.
, pp")
141
Rat atrial extracts increase sodium excretion when injected into anesthetized rats Atrial Natriuretic Factor (ANF) Atrial Natriuretic Peptide (ANP) DeBold et al., Life Sci.1981
 Atrial Natriuretic Peptide (ANP) DeBold et al., Life Sci.1981")
142
Volume Expansion Atrial Stretch Vasodilatation Blood Pressure Increased Na + & H 2 O Excretion ANP atrial natriuretic peptide Actions mediated by cGMP

143
Similar Structures of the Natriuretic Peptides Family Atria Other tissues Brain Atria Ventricles CNS Vasculature

144
Dendroaspis angusticeps Green Mamba Dendroaspis natriuretic peptide (DNP)
")
145
SODIUM EXCRETION ATRIAL STRETCH ANP BLOOD VOLUME EXPANSION ALDOSTERONE BLOOD PRESSURE Actions of Atrial Natriuretic Peptide GFR Actions mediated by cGMP

146
Active ANP Neutral Endopeptidase Inhibitors Increase ANP Neutral Endopeptidase Neutral Endopepidase Inhibitor Inactive ANP

147
Sympathetic Increase Na+ Reabsorption Arterioles JG Cells Kf (Surface Area) Tubule PP1 Na + K + Lumen Capillary Na + P P Active APTase Inactive APTase Norepinephrine and Angiotensin II Ca 2+ /Calmodulin - Tubule Sympathetics (Norepi or Epi) increase the active Na/K APTase and thus increase Na reabsorption. AII has a similar effect but different receptor.

148
Angiotensin II Increases Na+ Reabsorption Angiotensin II constricts both arterioles but has more effect on efferent. FF = GFR RPF Result: Protein Osmotic Pressure Increased in peritubular Capillaries Aldosterone Kf (surface area) Proximal Reabsorption Filtration Fraction (FF)
 Proximal Reabsorption Filtration Fraction (FF).")
149
Regulation of Na+ Excretion Aldosterone Increases Na + Reabsorption Distal Tubule and Cortical Collecting Duct Lumen Capillary -70 mV Na + K + + K + K +

150
Decreased Protein Osmotic Pressure Increases Na+ Excretion (glomerulus)
")
151
Decreased Protein Osmotic Pressure Increases Na+ Excretion (Proximal Tubule)
")
152
Increased Na + Intake Results in Increased Blood Flow to Cortex Juxtamedullary Nephron Salt Sparing Cortical Nephron Salt Wasting

153
ANGIOTENSIN II SYMPATHETICS ALDOSTERONE HEMODYNAMICS ANP PROTEIN OSMOTIC PRESSURE Regulation of Na+ Excretion

154
Regulation of Water & K + Excretion John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

155
Renal Regulation of Special Substances (Water and Potassium) At the end of this section you should know: How water excretion is controlled by ADH How water excretion is markedly affected by solute excretion (osmotic diuresis). Regulation of ADH secretion (review) that potassium excretion is controlled by secretion in the DT and cortical CD. how changes in plasma K+ or aldosterone affect K+ secretion. how potassium excretion is altered by diuretics.
 that potassium excretion is controlled by secretion in the DT and cortical CD. how changes in plasma K+ or aldosterone affect K+ secretion. how potassium excretion is altered by diuretics..")
156
Collecting Duct ADH cAMP Lumen (hypotonic) Interstitium (hypertonic) V 2 H 2 O
 Interstitium (hypertonic) V 2 H 2 O")
157
Primary control of H 2 O excretion by ADH. Osmotic diuresis The reabsorption of solutes is not dependent on the reabsorption of water. The reabsorption of water is dependent on the reabsorption of solutes. Increased solute excretion nearly always results in increased urine flow Regulation of Water Excretion

158
Osmotic Diuresis

159
Regulation of Water Excretion ADH effects urine flow (UF) by altering free water excretion. If Uosm > Posm = net H 2 O reabsorption (or negative free water excretion). If Uosm < Posm = net H 2 O excretion (or positive free water excretion). If the urine is isoosmotic to plasma then free water excretion = 0. Most factors (other than ADH) alter UF by changing solute excretion.
. If Uosm < Posm = net H 2 O excretion (or positive free water excretion). If the urine is isoosmotic to plasma then free water excretion = 0. Most factors (other than ADH) alter UF by changing solute excretion..")
160
? You have a patient with hypertension who you have been treating with a loop diuretic for 1 month. His initial plasma [K+] was 4.5 mEq/L and has decreased to 3.0 mEq/L ? Why would a diuretic cause hypokalemia ? ? How much potassium has the patient lost ? ? How can your knowledge of physiological processes help you treat the hypoklemia ? Potassium

161
Volume (L) 028 14 ECFICF 140 mmoles/L 4.5 mmoles/L 4000 mmoles 60 mmoles Potassium Intake = 100 mmoles/day Potassium Excretion = 100 mmoles/day 90% urine 10% feces
 ECFICF 140 mmoles/L 4.5 mmoles/L 4000 mmoles 60 mmoles Potassium Intake = 100 mmoles/day Potassium Excretion = 100 mmoles/day 90% urine 10% feces")
162
Regulation of Potassium Excretion 100% of the filtered K + is reabsorbed by the beginning of the distal tubule K + Reabsorption K + Secretion

163
Regulation of Potassium Excretion Aldosterone Increases K + Secretion & K + Stimulates K + Secretion Directly Distal Tubule and Cortical Collecting Duct Lumen Capillary -70 mV Na + K + K + + K +

165
? You have a patient with hypertension who you have been treating with a loop diuretic for 1 month. His initial plasma [K+] was 4.5 mEq/L and has decreased to 3.0 mEq/L ? Why would a diuretic cause hypokalemia ? ? How much potassium has the patient lost ? How can your knowledge of physiological processes help you treat the hypoklemia ? Potassium

166
Diuretics and Potassium ? Why would a diuretic cause hypokalemia ?

167
Renal Contribution to Calcium Homeostasis

168
Renal Regulation of Special Substances (Calcium, Phosphate, Magnesium) At the end of this section you should know: mechanisms controlling Ca2+ absorption. mechanisms controlling phosphate excretion. Mg2+ is absorbed in the TAL and excretion affected by diuretics. changes in calcium balance in renal failure.

169
Renal Contribution to Calcium Homeostasis 1. Calcium reabsorption. Parathyroid hormone (PTH) -increases reab. DT and CD. Vitamin D also increases reab. in DT. 2. Phosphate excretion. PTH-decreases reab. PT. 3. Active form of Vitamin D is made in the kidneys
 -increases reab. DT and CD. Vitamin D also increases reab. in DT. 2. Phosphate excretion. PTH-decreases reab. PT. 3. Active form of Vitamin D is made in the kidneys.")
170
Regulation of Calcium Reabsorption Early Distal Tubule Na + Cl - Na + K + Lumen Capillary AT P -ase Na + Ca ++ -70 mV PTH Ca ++ PTH PTH stimulates calcium entry from lumen to cell and calcium movement from cell to plasma exchanged for Na+. Thiazide Diuretics X

171
Regulation of Calcium Ca ++ Blood Parathyroid Gland PTH Ca ++ Vit. D 3 Ca ++ absorption Ca ++ PO 4 - Ca ++ PO 4 - PTH Ca ++ and PO 4 - resorption PTH Vit. D 3 Ca ++ reabsorption & PO 4 - excretion Ca ++ PO 4 -

172
Calcium handling in renal disease Vitamin D 3 Plasma Ca 2+ PTH Bone Plasma HPO 4 2- ? ? ? ? ?

173
Ca ++ Blood Calcium handling in renal disease Parathyroid Gland PTH Ca ++ PO 4 - Ca ++ Vit. D 3 Ca ++ absorption Ca ++ PO 4 - PTH Ca ++ and PO 4 - resorption PTH Vit. D 3 Ca ++ reabsorption & PO 4 - excretion Ca ++ PO 4 -

174
1. Reabsorbed primarily in the Thick Ascending Limb. 2. Reabsorption stimulated by: PTH Calcitonin ADH Hypomagnesemia 3. Excretion markedly increased by diuretics. Renal Contribution to Magnesium Homeostasis ?

175
Thick Ascending Limb of Loop of Henle Na + K + Lumen (+) Capillary Na + K + 2 Cl - K + Ca 2+ Mg 2+
 Capillary Na + K + 2 Cl - K + Ca 2+ Mg 2+")
176
Renal Hormones & Fluid Balance Review of everything John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida, College of Medicine

177
Renal Hormones & Fluid Balance At the end of this section you should know: Regulation of erythropoietin secretion. Regulation of renin secretion. Prostaglandins as renal vasodilators help regulate RBF. Mechanisms for monitoring body fluid volume and osmolality. Regulation of both salt and water intake and output. Physiologic changes to salt deficit or excess. Fluid balance changes to hypertension or hypotension.

178
RBC Production Oxygen Delivery { Hypoxia Ischemia Erythropoietin Kidney - Heme receptor (Peritubular Capillaries) Bone Marrow Erythroid Precursor Cells to Normoblasts
 Bone Marrow Erythroid Precursor Cells to Normoblasts")
179
Renin-Angiotensin system Regulation of Blood Pressure and Sodium Output The American Heritage® Dictionary of the English Language

180
Stimulation of Renin Secretion Blood pressure activates renal vascular receptor (baroreceptor) and renin. Blood pressure also GFR and delivery of Cl - to Macula Densa in the distal tubule which renin. Blood pressure causes a reflex activation of renal sympathetic nerves which renin. Juxtaglomerular Apparatus

181
Renin-Angiotensin-Aldosterone System

182
Emerging! ACE (angiotensin converting enzyme) Converts AI (10 aa) to AII (8 aa) Actions of AII vasoconstrictor releases aldosterone anti-natriuretic causes heart remodeling causes cardiac fibrosis ACE 2 Converts AII to A 1-7 (7 aa) Actions of A 1-7 vasodilator decreases aldosterone natriuretic prevents heart remodeling prevents cardiac fibrosis IMHO this will lead to new treatments for hypertension and CHF.
 Converts AI (10 aa) to AII (8 aa) Actions of AII vasoconstrictor releases aldosterone anti-natriuretic causes heart remodeling causes cardiac fibrosis ACE 2 Converts AII to A 1-7 (7 aa) Actions of A 1-7 vasodilator decreases aldosterone natriuretic prevents heart remodeling prevents cardiac fibrosis IMHO this will lead to new treatments for hypertension and CHF..")
183
Blood Pressure Renin (Kidney) Angiotensin I Angiotensin II Angiotensinogen (Liver) Angiotensin Converting Enzyme (ACE) Aldosterone Na + Reabsorption FF ADH & Thirst (water reabsorption) Vasoconstriction
 Angiotensin I Angiotensin II Angiotensinogen (Liver) Angiotensin Converting Enzyme (ACE) Aldosterone Na + Reabsorption FF ADH & Thirst (water reabsorption) Vasoconstriction ")
184
Hypertension Ureteral Constriction Renal Artery Constriction

185
Blood Pressure Renal Prostaglandins RBF Vasoconstriction (eg. AII and Norepi) Dilation RBF Infuse Angiotensin II into the renal artery 1 min.
 Dilation RBF Infuse Angiotensin II into the renal artery 1 min..")
186
Acute Renal Failure Pre-Renal Renal Post-Renal

187
CONTROL OF BODY SALT AND WATER What factors is the body trying to control and why? Where are the receptors? What are the effectors? What are the responses? ECF VOLUME ECF OSMOLALITY

188
Intake Output WATER

189
CONTROL OF WATER INTAKE Primarily by THIRST Stimuli: 1) Increased Osmolality 2) Decreased Arterial Pressure 3) Decreased Blood Volume 4) Angiotensin II WARNING: This is NOT an example of good bed-side manner
 Increased Osmolality 2) Decreased Arterial Pressure 3) Decreased Blood Volume 4) Angiotensin II WARNING: This is NOT an example of good bed-side manner")
190
CONTROL OF WATER OUTPUT Primarily by ADH Stimuli: 1) Increased Osmolality 2) Decreased Arterial Pressure 3) Decreased Blood Volume 4) Angiotensin II 5) Trauma 6) Surgery 7) Drugs eg. opiates and anesthetics.

191
NaCl Intake Blood Volume Plasma Proteins Atrial PressureArterial Pressure GFR Regulation of Na + Excretion Na + Excretion ANP SecretionSympathetics Renin Angiotensin II Aldosterone ? ? ? ? ? ? ? ? ? ? ?

192
Puffy Face and Bird legs

194
CapillaryInterstitiumIntracellular Na + 140 mMNa + 142 mMNa + 10 mM K + 4.5 mM K + 140 mM Proteins 1.5 mM Proteins 0.1 mM Proteins 3 mM Osm. = 286.5 mOsm/L 285 mOsm/L 285 mOsm/L Pc = 25 mmHg P = 0 mmHg = 28 mmHg = 3 mmHg Permeable to most solutes but imperm- eable to large proteins Impermeable to most solutes Comparison of the Three Major Compartments Colloid Osmotic Pressure, Protein Osmotic Pressure, Oncotic Pressure

195
Control of Water Intake & Output

196
Blood Volume Atrial Pressure Arterial Pressure GFR Hemorrhage Na + Excretion ANP Sympathetics Renin Angiotensin II Aldosterone ADH H 2 O Excretion ? ? ? ? ? ? ? ? ? ? ?

197
Congestive Heart Failure Clinical Correlation Dr. Bryan Bognar Internal Medicine

198
ACID-BASE BALANCE Regulation of Body pH 1)Chemical Buffering. 2) Respiratory Compensation. 3) Renal Compensation Why is pH regulated? How does a buffer work? CO 2 – Carbonic acid John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine
 Respiratory Compensation. 3) Renal Compensation Why is pH regulated. How does a buffer work. CO 2 – Carbonic acid John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine.")
199
Patient: Found unconscious with no pulse & no respiration. Blood drawn for electrolytes and gases (While attempting CPR) pH = 7.02(7.35-7.45)* O 2 = 30 mmHg(85-95)* CO 2 = 80 mmHg(35-45)* HCO 3 - = 19 mM(22-28)* Na + = 141 mEq/L(136-144) Cl - = 103 mEq/L(100-108) K + = 4.0 mEq/L(3.5-4.5)
 pH = 7.02( )* O 2 = 30 mmHg(85-95)* CO 2 = 80 mmHg(35-45)* HCO 3 - = 19 mM(22-28)* Na + = 141 mEq/L( ) Cl - = 103 mEq/L( ) K + = 4.0 mEq/L( ).")
200
pH AcidBase

201
Acid-base Chemistry At the end of this section you should know: Basic buffer chemistry. How to use the Hen.-Hass. Equation. Buffers in plasma, RBCs and other cells. Three lines of defense against changes in pH. pH: norm = 7.40, range 6.80-7.80 normal [H+] = 40 nM

202
Why do we regulate our pH? pH Normal = 7.40 (7.35-7.45) Viable range = 6.80 - 7.80 pH = 7.40 then [H+] = 40 nM = 0.000000040 M pH = 7.20 then [H+] = 60 nM pH = 7.10 then [H+] = 80 nM
 Viable range = pH = 7.40 then [H+] = 40 nM = M pH = 7.20 then [H+] = 60 nM pH = 7.10 then [H+] = 80 nM.")
203
Henderson-Hasselbalch Equation: pH = pK + log HCO 3 - CO 2

204
Production of Acids by the Human Body: Volatile Acids: CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + Non-Volatile Acids (fixed acids): H + + SO 4 2-
: H + + SO 4 2-")
205
First Line of Defense: Fast Physicochemical Buffering. Strong acid + Buffer salt Neutral salt + Weak acid H + + Cl - + Na + + HCO 3 - Na + + Cl - + H 2 CO 3 H 2 CO 3 CO 2 + H 2 O HCl H + + Cl - 100% HSO 4 - H + + SO 4 2- 10% H 2 CO 3 H + + HCO 3 - 0.07% Conjugate Base Dissociation of Acids

206
K = [H + ] [A - ] [HA] [H + ] = K [HA] [A - ] -log [H + ] = -log K - log [HA] [A - ] pH = pK + log __[A - ] __ [HA]
![K = [H + ] [A - ] [HA] [H + ] = K [HA] [A - ] -log [H + ] = -log K - log [HA] [A - ] pH = pK + log __[A - ] __ [HA]](http://images.slideplayer.com/37/10685824/slides/slide_206.jpg "K = [H + ] [A - ] [HA] [H + ] = K [HA] [A - ] -log [H + ] = -log K - log [HA] [A - ] pH = pK + log __[A - ] __ [HA]")
207
Titration Curves for the Bicarbonate and Phosphate Buffer Systems

208
pH = pK + log HCO 3 - = pK + log HPO 4 2- = pK + log Prot - pCO 2 H 2 PO 4 - H n Prot The Isohydric Principle: Special Characteristics of the Bicarbonate Buffer System: High [HCO 3 - ] [HCO 3 - ]/CO 2 = 24 : 1.2 or 20 : 1 Open System: Controlled pCO 2.
![pH = pK + log HCO 3 - = pK + log HPO 4 2- = pK + log Prot - pCO 2 H 2 PO 4 - H n Prot The Isohydric Principle: Special Characteristics of the Bicarbonate Buffer System: High [HCO 3 - ] [HCO 3 - ]/CO 2 = 24 : 1.2 or 20 : 1 Open System: Controlled pCO 2.](http://images.slideplayer.com/37/10685824/slides/slide_208.jpg "pH = pK + log HCO 3 - = pK + log HPO 4 2- = pK + log Prot - pCO 2 H 2 PO 4 - H n Prot The Isohydric Principle: Special Characteristics of the Bicarbonate Buffer System: High [HCO 3 - ] [HCO 3 - ]/CO 2 = 24 : 1.2 or 20 : 1 Open System: Controlled pCO 2.")
209
Henderson-Hasselbalch Equation: pH = pK + log [HCO 3 - ] [H 2 CO 3 ] CO 2 + H 2 O pH = pK + log [HCO 3 - ] Dissolved CO 2 + H 2 CO 3 400 : 1 pH = 6.1 + log 24 mMoles/L 0.03 x 40 mmHg*** pH = 6.1 + log 24 mMoles/L = 6.1 + log 20 1.2 mMoles/L = 7.40
![Henderson-Hasselbalch Equation: pH = pK + log [HCO 3 - ] [H 2 CO 3 ] CO 2 + H 2 O pH = pK + log [HCO 3 - ] Dissolved CO 2 + H 2 CO : 1 pH = log 24 mMoles/L 0.03 x 40 mmHg*** pH = log 24 mMoles/L = log mMoles/L = 7.40](http://images.slideplayer.com/37/10685824/slides/slide_209.jpg "Henderson-Hasselbalch Equation: pH = pK + log [HCO 3 - ] [H 2 CO 3 ] CO 2 + H 2 O pH = pK + log [HCO 3 - ] Dissolved CO 2 + H 2 CO : 1 pH = log 24 mMoles/L 0.03 x 40 mmHg*** pH = log 24 mMoles/L = log mMoles/L = 7.40")
210
ADDITION OF A STRONG ACID (eg. HCl): First Line of Defense: The Henderson-Hasselbalch Equation Fast Chemical Buffering 12 H + + 12 Cl - + 24 Na + + 24 HCO 3 - 24 Na + + 12 Cl - + 12 HCO 3 - + 12 H 2 CO 3 12 CO 2 + 12 H 2 O pH = 6.1 + log 12 mmoles/L 1.2 + 12 mmoles/L pH = 6.1 + log 12 mmoles/L 13 mmoles/L pH = 6.06
: First Line of Defense: The Henderson-Hasselbalch Equation Fast Chemical Buffering 12 H Cl Na HCO 3 - 24 Na Cl HCO H 2 CO 3 12 CO H 2 O pH = log 12 mmoles/L mmoles/L pH = log 12 mmoles/L 13 mmoles/L pH =")
211
Alveolar ventilation increased further because of acidosis. pH = 6.1 + log 12 mmoles/L 0.75 mmoles/L (pCO 2 = 25mmHg) pH = 7.30 Second Line of Defense: Fast Respiratory Component. Alveolar ventilation increased to maintain pCO 2 at 40 mmHg (1.2 mmoles/L). pH = 6.1 + log 12 mmoles/L 1.2 mmoles/L pH = 7.10
 pH = 7.30 Second Line of Defense: Fast Respiratory Component. Alveolar ventilation increased to maintain pCO 2 at 40 mmHg (1.2 mmoles/L). pH = log 12 mmoles/L 1.2 mmoles/L pH =")
212
Third Line of Defense: Slow Renal Compensation (H + secretion and HCO 3 - reabsorption) Over a period of days plasma HCO 3 - returns to normal. pH = 6.1 + log 24 mmoles/L 1.2 mmoles/L pH = 7.40

213
Acid Excretion John R. Dietz, Physiology & Biophysics University of South Florida, College of Medicine

214
Acid Excretion At the end of this section you should know: how H+ and HCO3- are formed in the renal tubular cells. the permeability of the tubule to H+ and HCO3- and how H+ is exchanged for Na+. the three substances that H+ combines with in the renal tubule. how physiological perturbations (e.g. CO2) affect H+ secretion, HCO3- reabsorption and NH4+ production. how H+ secretion is affected by aldosterone, K+ or in disease states.
 affect H+ secretion, HCO3- reabsorption and NH4+ production. how H+ secretion is affected by aldosterone, K+ or in disease states..")
215
Henderson-Hasselbalch Equation: pH = pK + log HCO 3 - CO 2 pH =

216
H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+

217
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + HCO 3 - Cl - HCO 3 - Na + H+H+ ATPase H+H+ C.A. BloodCellLumen ATPase H+H+ K+K+ Renal Transport of HCO 3 - & H +

218
H + exchanged for Na + H + ATPase H + - K + ATPase Various Mechanisms of H+ Secretion

219
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + Bicarbonate Reabsorption C.A. Filtered H 2 CO 3 CO 2 + H 2 O C.A. Primarily in Proximal Tubule - 0 % of Acid Excretion BloodCellLumen HCO 3 - Na + HCO 3 - Na + H+H+ H+H+

220
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + Bicarbonate Reabsorption C.A. Filtered H 2 CO 3 CO 2 + H 2 O C.A. Primarily in Proximal Tubule - 0 % of Acid Excretion BloodCellLumen HCO 3 - Na + HCO 3 - Na + H+H+ H+H+

221
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + Titratable Acid Excretion C.A. Na + Filtered H + + HPO 4 2- Primarily in Distal Tubule & CD - 33 % of Acid Excretion Na + + H 2 PO 4 - or H SO 4 - + HPO 4 2- or SO 4 2- H+H+ BloodCellLumen HCO 3 - Cl - ATPase

222
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + Ammonium Excretion C.A. H + + NH 3 Primarily in Distal Tubule & CD - 66 % of Acid Excretion NH 4 + H+H+ NH 3 produced in the cortex from glutamine NH 3 [H+] is 1000 X greater in the lumen than the cell HCO 3 - Cl - ATPase

223
H+ Secretion in the Nephron

224
Factors that Stimulate H+ Secretion Acidosis Metabolic or Respiratory Hypokalemia Aldosterone

225
Regulation of H+ Excretion CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + HCO 3 - Na + H+H+ C.A. BloodCellLumen ATPase

226
Renal Responses to a Metabolic Acidosis Decreased filtered bicarbonate Increased H + secretion Increased NH 3 production

227
H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ H+H+ Increased Renal Acid Secretion in Acidosis

228
Long-term Renal Compensation for Acidosis

229
Respiratory Alkalosis

230
CO 2 + H 2 O H 2 CO 3 HCO 3 - + H + HCO 3 - Na + H+H+ C.A. BloodCellLumen HCO 3 - Respiratory Alkalosis ATPase

231
H+H+ H+H+ H+H+ H+H+ H+H+ HCO 3 - Decreased Acid Secretion with Respiratory Alkalosis (Hyperventilation)
")
232
Renal Tubule Acidosis (RTAs) 1.Type 1 - Distal RTA 2.Type 2 - Proximal RTA 3.Type 4 - Lack of Aldosterone
 1.Type 1 - Distal RTA 2.Type 2 - Proximal RTA 3.Type 4 - Lack of Aldosterone")
233
Clinical Aspects of Acid-Base Balance pH = pK + log HCO 3 - CO 2 John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

234
Clinical Aspects of Acid-Base Balance At the end of this section you should know: The physiological changes in the 4 primary acid base disturbances. How to read a Davenport diagram Compensation for acid-base disturbances. Causes of Acid-Base disturbances. Acid-Base Balance Disturbances

235
Buffering by Hemoglobin CO 2 HCO 3 - /H 2 CO 3 Solution (HCO 3 - = 24 mM) HCO 3 - /H 2 CO 3 + BUF - /HBUF (Hemoglobin) Remember: CO 2 + H 2 O H 2 CO 3 H + + HCO 3 -
 HCO 3 - /H 2 CO 3 + BUF - /HBUF (Hemoglobin) Remember: CO 2 + H 2 O H 2 CO 3 H + + HCO 3 -")
236
TRANSPORT OF CO 2 AND BUFFERING BY HEMOGLOBIN Most CO 2 is transported in the blood as HCO 3 -

237
pH = pK + log HCO 3 - CO 2 Normal Acid-Base Conditions

238
A RESPIRATORY ACIDOSIS SOME POSSIBLE CAUSES: 1) COPD, CHF and other lung diseases. 2) Anesthetics and Drugs pH = pK + log HCO 3 - CO 2
 Anesthetics and Drugs pH = pK + log HCO 3 - CO 2 .")
239
RESPIRATORY ALKALOSIS SOME POSSIBLE CAUSES: 1) Pain. 2) Hysteria. 3) Hypoxia. pH = pK + log HCO 3 - CO 2 B
 Hysteria. 3) Hypoxia. pH = pK + log HCO 3 - CO 2 B.")
240
METABOLIC ACIDOSIS SOME POSSIBLE CAUSES: 1) Loss of Base (eg. diarrhea). 2) Gain of Acid (diabetes, renal failure). pH = pK + log HCO - 3 CO 2 C
. 2) Gain of Acid (diabetes, renal failure). pH = pK + log HCO - 3 CO 2 C.")
241
pH = pK + log HCO - 3 CO 2 METABOLIC ALKALOSIS SOME POSSIBLE CAUSES: 1) Over Ingestion of Base. 2) Loss of Acid (Vomiting, Gastric Suction Tube). D
 Loss of Acid (Vomiting, Gastric Suction Tube). D.")
242
Anion Gap Plasma [Na + ] - ( [Cl - ] + [HCO 3 - ] ) or approximately 8-16 mEq/L (5-11 mEq/L) Metabolic Acidosis Normal anion gap acidosis - HCO 3 - decreases and replaced by Cl - shift: Eg. Diarrhea or simple gain of H + + Cl - Increased anion gap acidosis - HCO 3 - decreases and replaced by other anions so no Cl - shift: Eg. lactic acidosis and diabetic keto-acidosis
![Anion Gap Plasma [Na + ] - ( [Cl - ] + [HCO 3 - ] ) or approximately 8-16 mEq/L (5-11 mEq/L) Metabolic Acidosis Normal anion gap acidosis - HCO 3 - decreases and replaced by Cl - shift: Eg.](http://images.slideplayer.com/37/10685824/slides/slide_242.jpg "Diarrhea or simple gain of H + + Cl - Increased anion gap acidosis - HCO 3 - decreases and replaced by other anions so no Cl - shift: Eg. lactic acidosis and diabetic keto-acidosis.")
243
Something to remember for Years 2-4

244
Renal and Respiratory Compensatory Responses to Disturbances in Acid-Base Balance

245
AcidosispHAlkalosis 7.35- 7.45 Metabolic (Bicarbonate) 22- 28 Respiratory (CO 2 ) 45- 35 Willie’s Acid-Base Box Patient pH = 7.27 HCO 3 - = 25 CO 2 = 60 From William Lipscomb, Ph.D.
 Respiratory (CO 2 ) Willie’s Acid-Base Box Patient pH = 7.27 HCO 3 - = 25 CO 2 = 60 From William Lipscomb, Ph.D.")
246
AcidosispHAlkalosis 7.35- 7.45 Metabolic (Bicarbonate) 22- 28 Respiratory (CO 2 ) 45- 35 Willie’s Acid-Base Box Patient pH = 7.34* HCO 3 - = 30* CO 2 = 60* From William Lipscomb, Ph.D. *After compensation

247
Patient: Found unconscious with no pulse & no respiration. Blood drawn for electrolytes and gases (While attempting CPR) pH = 7.02(7.35-7.45)* O 2 = 30 mmHg(85-95)* CO 2 = 80 mmHg(35-45)* HCO 3 - = 19 mM(22-28)* Na + = 141 mEq/L(136-144) Cl - = 103 mEq/L(100-108) K + = 4.0 mEq/L(3.5-4.5)
 pH = 7.02( )* O 2 = 30 mmHg(85-95)* CO 2 = 80 mmHg(35-45)* HCO 3 - = 19 mM(22-28)* Na + = 141 mEq/L( ) Cl - = 103 mEq/L( ) K + = 4.0 mEq/L( ).")
248
AcidosispHAlkalosis 7.35- 7.45 Metabolic (Bicarbonate) 22- 28 Respiratory (CO 2 ) 45- 35 Willie’s Acid-Base Box Patient pH = 7.02 HCO 3 - = 19 CO 2 = 80
 Respiratory (CO 2 ) Willie’s Acid-Base Box Patient pH = 7.02 HCO 3 - = 19 CO 2 = 80")
249
Renal Failure Patient Patient Data (Plasma)Change from Normal K + Phosphate Calcium Sulfate Urea Hematocrit Blood Pressure Bicarbonate pH
Change from Normal K + Phosphate Calcium Sulfate Urea Hematocrit Blood Pressure Bicarbonate pH ")
250
Physiology of the Kidneys Body Fluids & Acid Base Balance MDC 2541 974-1548 jdietz@health.usf.edu John R. Dietz, Ph.D. Molecular Pharmacology & Physiology University of South Florida College of Medicine

Similar presentations











Regulation of body fluid volume 2)Regulation of Osmolarity & Ion Balance 3)Regulation of pH 4)Excretion of Wastes.>")







. Other excretory.>")