Download presentation
Presentation is loading. Please wait.

1
Bernie Miller, MD, CA3 OHSU APOM
Regional Anesthesia Bernie Miller, MD, CA3 OHSU APOM

2
Regional Anesthesia Rendering a specific area of the body insensate to stimulus of surgery or other instrumentation

4
Advantages Major Intra-abdominal surgery Ambulatory Surgery
Cardiac disease Vascular surgery Pulmonary resection/rib fractures Obstetric Patients Chronic Pain Oncologic Surgery?

5
Types of Regional Anesthesia
Topical Local/Field IV block- “Bier Block” Peripheral Nerve block (named after the nerve) Plexus block (eg lumbar, brachial) Central Neuraxial (spinal, epidural)
 Plexus block (eg lumbar, brachial) Central Neuraxial (spinal, epidural)")
6
Topical Anesthesia Application of local anesthetic to mucous membrane
Uses Awake oral or nasal intubation Superficial surgical procedure Advantage Easy to do Disadvantage Potential for large doses leading to toxicity

7
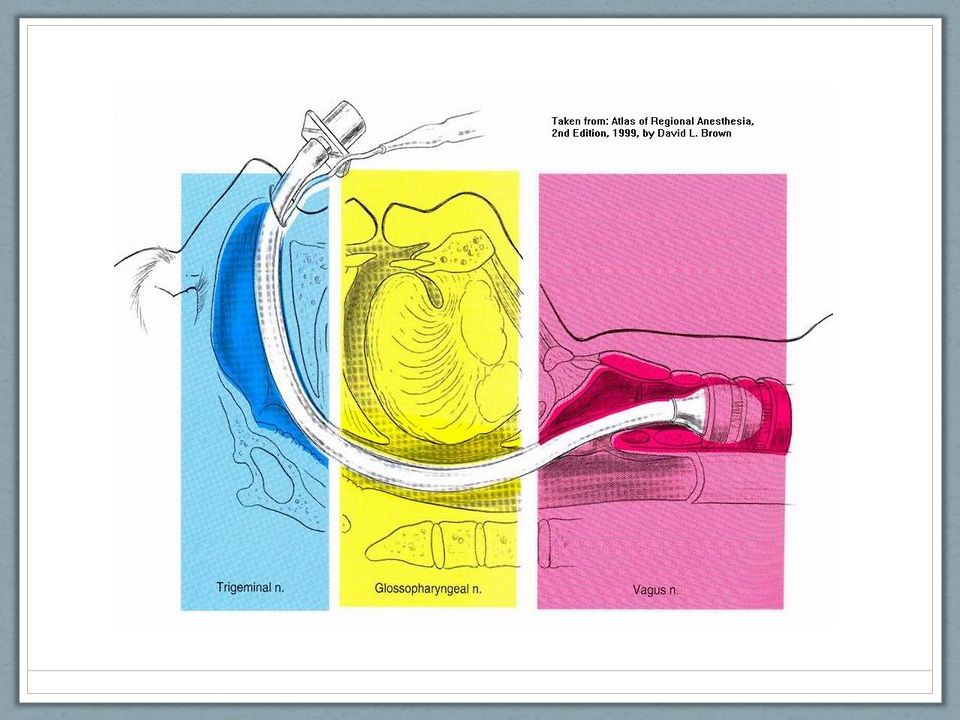
Airway blocks Injection of LA to block airway nerves
Uses: facilitation of awake intubation Advantage: complete lack of sensation in the airway, blunting of airway reflexes Disadvantage: Potential for injury/injection of surrounding major vascular structures or CSF More invasive than topicalization

9
Glossopharyngeal Nerve Block

10
Superior Laryngeal Block
(sensory branch)
")
11
(recurrent laryngeal)
Transtracheal block (recurrent laryngeal)
")
12
Local/Field Anesthesia
Application of local subcutaneously to anesthetize distal nerve endings (small local area or field) Uses: Suturing, minor superficial surgery, line placement Advantages: minimal equipment, technically easy, rapid onset Disadvantages: potential for toxicity if large field
 Uses: Suturing, minor superficial surgery, line placement. Advantages: minimal equipment, technically easy, rapid onset. Disadvantages: potential for toxicity if large field.")
13
“IV” Block – “Bier” Block
Injection of local anesthetic IV for anesthesia of an extremity Uses Any short surgical procedure on a distal extremity Advantages Technically simple, minimal equipment, rapid Disadvantages Duration limited by tolerance of tourniquet pain, toxicity

15
Peripheral/Plexus Nerve Block
Injecting local anesthetic near the course of a named nerve or plexus Uses: Surgical procedures in the distribution of the blocked nerve Pain control of a specific area Advantages: More bang for your buck (more coverage with less LA) Less narcotic Patient can either be sedated or fully awake and functional Limb specific Disadvantages: technical complexity, neuropathy
 Less narcotic. Patient can either be sedated or fully awake and functional. Limb specific. Disadvantages: technical complexity, neuropathy.")
16
Single shot vs Catheter
Fast placement Smaller introducing needle More complex placement- two step process Duration of anesthetic not limited to duration of drug action

17
Setup/method Often in a designated “block” room or space with dedicated team Supplies Monitor vitals Sedation Can use ultrasound guidance or nerve stimulation Positioning! Localize nerve based on anatomy, confirm location with device Communicate with patient Inject and/or or thread catheter Test dose

18
Nerve stimulator Provides short, low frequency electric impulse to elicit defined muscle response Based on known innervation of nerve Can use transcutaneously to plan approach Can use with needle during block Good response at low output indicates close proximity to the nerve Inject local Should lose response as conduction blocked

19
Ultrasound vs Stimulator
US Stimulator Benefit Direct visualization Real-time visualization Hard-to-find landmarks Drawback Osseous or gas-filled structures impede signal Takes up an extra hand Can be misleading (need to see tip) Benefit Confirm correct nerve function Attaches to needle in use Drawback No visualization of neighboring structures Requires assistant’s hands Discomfort Unreliable in neuropathy
 Benefit. Confirm correct nerve function. Attaches to needle in use. Drawback. No visualization of neighboring structures. Requires assistant’s hands. Discomfort. Unreliable in neuropathy.")
20
Peripheral/Plexus Block
Upper Extremity Brachial plexus interscalene supraclavicular Infraclavicular Axillary Median Ulnar Radial Lower Extremity Femoral Sciatic Obturator Saphenous Tibial Ankle Lumbar plexus Others: TAP block, paravertebral block

21
Upper Extremity Plexi Cervical Plexus Brachial Plexus
Ventral Rami of C1-C4 Located deep to the SCM in the neck Advanced regional technique Brachial Plexus Ventral rami of C5-T1 Responsible for cutaneous and muscular innervation of upper limb

22
Brachial plexus blocks
Level Potential Drawback Uses Interscalene Roots, Trunks Spares inferior trunk Shoulder, upper arm Supraclavicular Trunks, Divisions Risk for pneumo Entire arm, including hand Infraclavicular Cords Pectoral discomfort Entire arm, good for catheter

23
Interscalene Block Patient position Anatomical landmarks
Supine with head rotated 30 degrees to C/L side Anatomical landmarks Determine interscalene groove (AS & MS) at the level of C6 where the nerves emerge from behind the scalene muscles (be careful of the EJ!). Do not confuse the interscalene groove with the AS/SCM groove.
 at the level of C6 where the nerves emerge from behind the scalene muscles (be careful of the EJ!). Do not confuse the interscalene groove with the AS/SCM groove.")
25
Casualty nerves: phrenic – hemidiaphragmatic paralysis
sympathetic chain – Horner’s recurrent laryngeal - hoarseness

27
Supraclavicular

28
Infraclavicular

29
Axillary Nerve Block Advantages
Provides anesthesia for forearm & wrist Fewer complications than a supraclavicular block Limitations Not for shoulder or upper arm surgery Musculocutaneous nerve lies outside of the sheath and must be blocked separately Complications Intravascular injection Elevated bleeding time increases risk for hematoma

30
Axillary Block Position Head turned away from arm being blocked
Abduct to 90º Forearm is flexed to 90º Palpate brachial artery for pulse

31
Axillary Nerve Block

32
Axillary Nerve Block

33
Femoral Nerve Block (L2-L4)
Uses: Knee arthroscopy in combination with intra- articular local anesthetic Good for femoral shaft fractures, ACL, TKA with multimodal regimen Limitations: Not reliable for posterior knee, lower leg or upper thigh Complications: Arterial puncture Abdominal cavity puncture

34
Femoral block landmarks “NAVL”
Draw a line between the ASIS and the pubic tubercle Determine location of femoral artery Introduce needle one cm lateral to artery

36
Sciatic Nerve Block (L4-5, S1-3)
Uses: Nearly complete blockade of the foot and ankle What does the sciatic nerve turn into? Limitations: Not a good block for upper thigh or hip Advantages: Easy to palpate anatomic landmarks No major vessels near the nerve

39
Popliteal nerve block Uses : Lower 2/3 of leg
Does not cover medial (saphenous) Objective Find the sciatic bifurcation Anesthetize both branches Tibial Common peroneal
 Objective. Find the sciatic bifurcation. Anesthetize both branches. Tibial. Common peroneal.")
40
Posterior Approach

41
Finding the bifurcation
Proximal Distal

42
Ankle Block Five nerves Tibial Superficial peroneal Saphenous Sural
Deep peroneal

43
Ankle block

44
Lower Plexus Blocks Lumbar Plexus L2-L4
Form the obturator, lateral femoral cutaneous, and femoral nerves Provides sensory and motor innervation to anterior lower extremity Lumbosacral plexus L4-L5, S1-S3 Primarily forms the sciatic nerve Provides motor and sensory innervation to posterior lower extremity Rarely done

45
L2-L4

46
Lumbar Plexus block Uses: Disadvantages Potential complications
Obturator, femoral, and lateral femoral cutaneous nerves in the belly of the psoas muscle Knee, thigh and hip Catheter frequently used to extend block Disadvantages Not useful for lower leg or foot Cannot use real-time ultrasound Potential complications Bleeding from psoas muscle bed Increased systemic absorption of local anesthetic from increased vascularity

47
Lumbar plexus Positioning
Lateral decubitus positioning with the blocked side up Foot of the side being blocked should be over the dependent leg so the twitches of the patella can be seen.

48
Lumbar plexus Landmarks
Locate both iliac crests and and draw a line between them, this is usually the location of L4 (Tuffier’s) Generally, the plexus will be 4cm lateral to the spinous process along this line.
 Generally, the plexus will be 4cm lateral to the spinous process along this line.")
49
TAP block Transversus abdominis plane block
Good for abdominal surgery Single shot (less frequently catheter) Can be used as rescue LA spread between internal oblique and transversus abdominus muscles Anesthetize anterior rami of T7-L1
 Can be used as rescue. LA spread between internal oblique and transversus abdominus muscles. Anesthetize anterior rami of T7-L1.")
50
TAP block

51
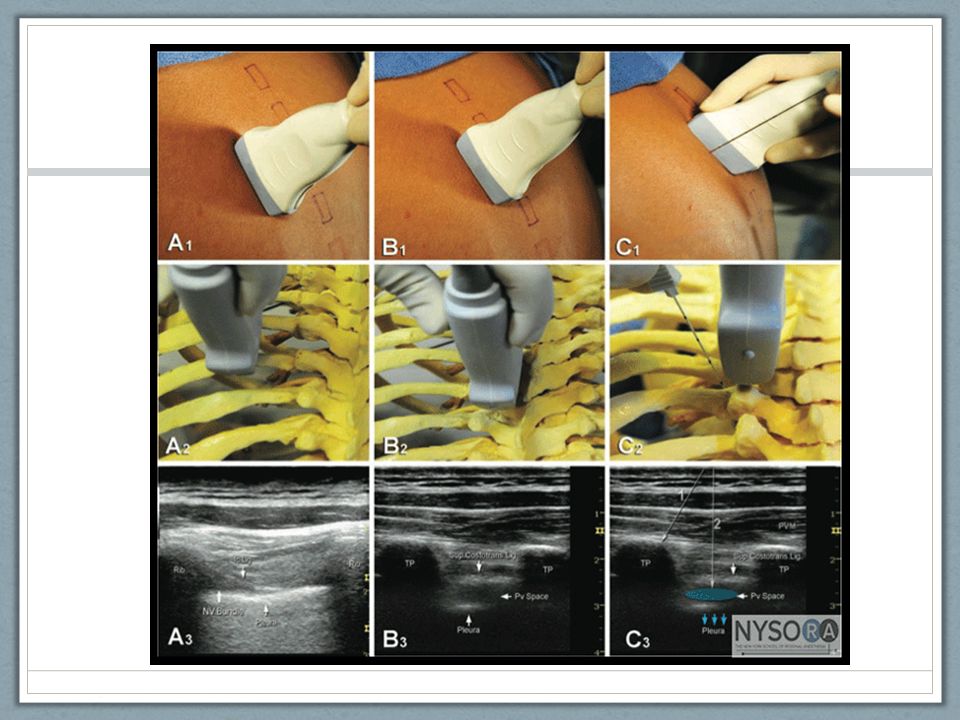
Paravertebral block Anesthetize thoracic spinal nerves within paravertebral space above L1 Thoracic, chest wall, breast, rib fx Unilateral or bilateral Usually single shot, catheter possible Landmark or ultrasound Complications?

53
In-line approach

54
Neuraxial anesthesia

55
Epidural Injection of local anesthetic +/- adjunct into the epidural space (lumbar, thoracic, caudal) Usually catheter is left in place for continued infusion Useful for intraoperative and post-operative pain control as well as labor analgesia Benefits: decreased ileus, pain control without respiratory depression, improved perfusion Potential drawbacks: hypotension (sympathectomy), pruritis, possible wet tap, potential for epidural hematoma or vascular injection, one-sided or patchy block
, pruritis, possible wet tap, potential for epidural hematoma or vascular injection, one-sided or patchy block.")
56
Thoracic epidural catheter

57
Spinal Injection of local anesthetic +/- adjunct into spinal space
Usually single shot procedure Can combine with epidural (CSE) Lumbar ONLY Complete motor and sensory block Fast to perform, quick onset, relatively short duration depending on choice of anesthetic, rarely fails More pronounced hypotension, possible spinal HA, possible high spinal
 Lumbar ONLY. Complete motor and sensory block. Fast to perform, quick onset, relatively short duration depending on choice of anesthetic, rarely fails. More pronounced hypotension, possible spinal HA, possible high spinal.")
58
Spinal via introducer

59
Want to learn more? http://www.nysora.com http://www.asra.com
Dr. Woodworth: iBook and Sakai

Similar presentations











 Brain Spinal cord Peripheral nervous system (PNS) Nerve outside the brain and spinal.>")













, Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi Medical college.>")