Download presentation
Presentation is loading. Please wait.

1
Glandular lesion and Iatrogenic lesion

2
“TBS” – Glandular cells
Atypical endocervical cells (NOS or specify in comments) endometrial cells (NOS or specify in comments) glandular cells (NOS or specify in comments) endocervical cells, favor neoplastic glandular cells, favor neoplastic Endocervical adenocarcinoma in situ Adenocarcinoma endocervical, endometrial, extrauterine, NOS
 endometrial cells (NOS or specify in comments) glandular cells (NOS or specify in comments) endocervical cells, favor neoplastic. glandular cells, favor neoplastic. Endocervical adenocarcinoma in situ. Adenocarcinoma. endocervical, endometrial, extrauterine, NOS.")
3
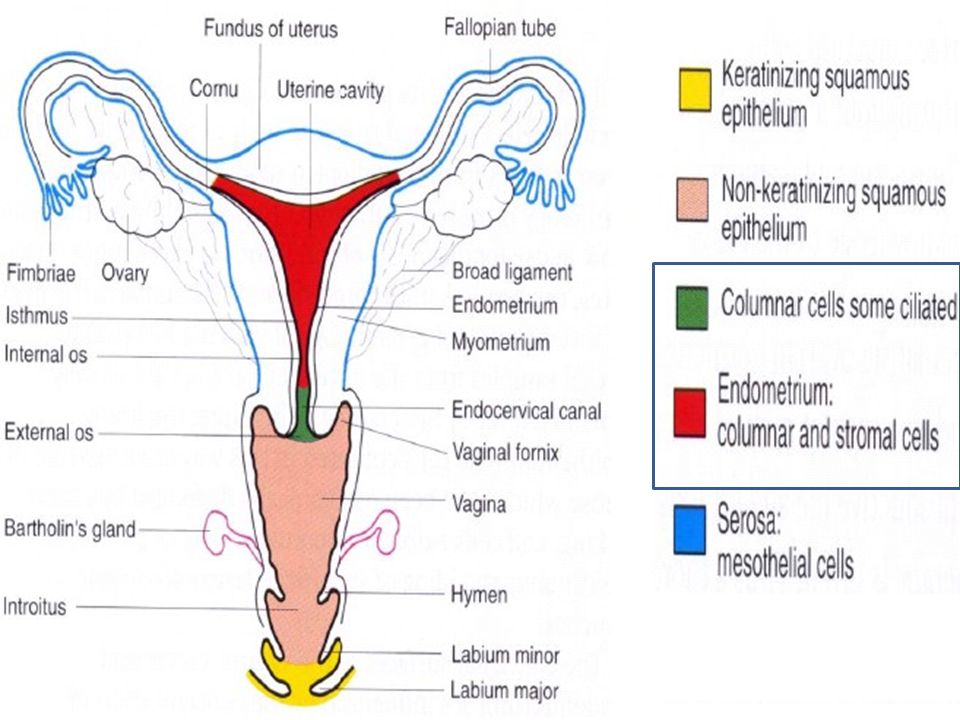
Glandular Lesions of the Female Genital Tract
Sampling techniques; Routine smears: The vaginal pool may contain exfoliated cells from the endocervix, endometrium, and endosalpinx, and even from the ovaries 2. Endometrial aspiration 3. Endometrial lavage

5
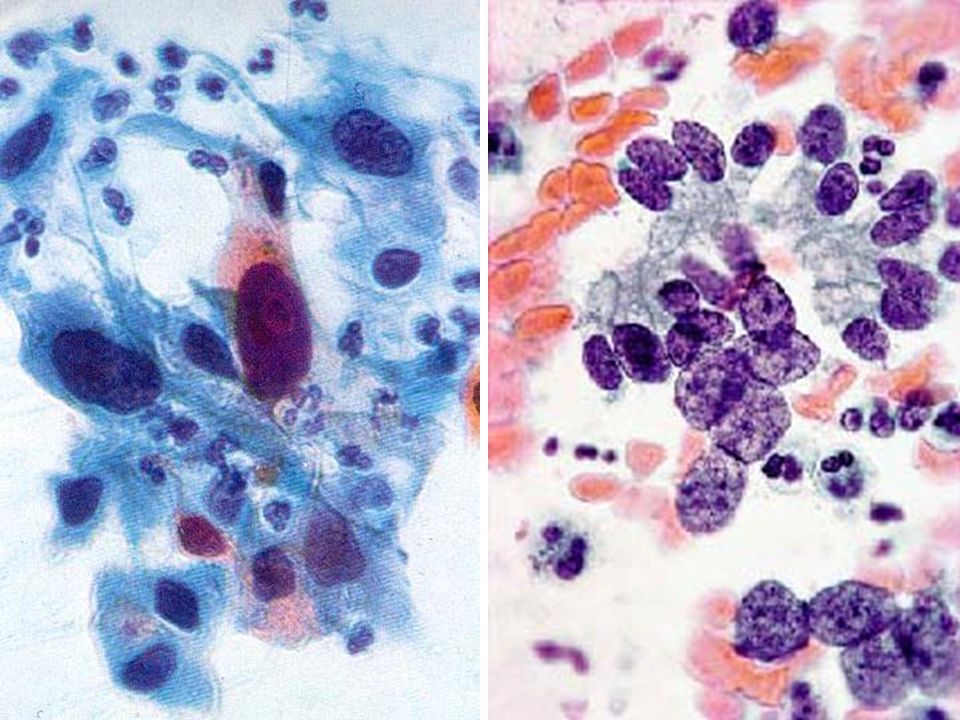
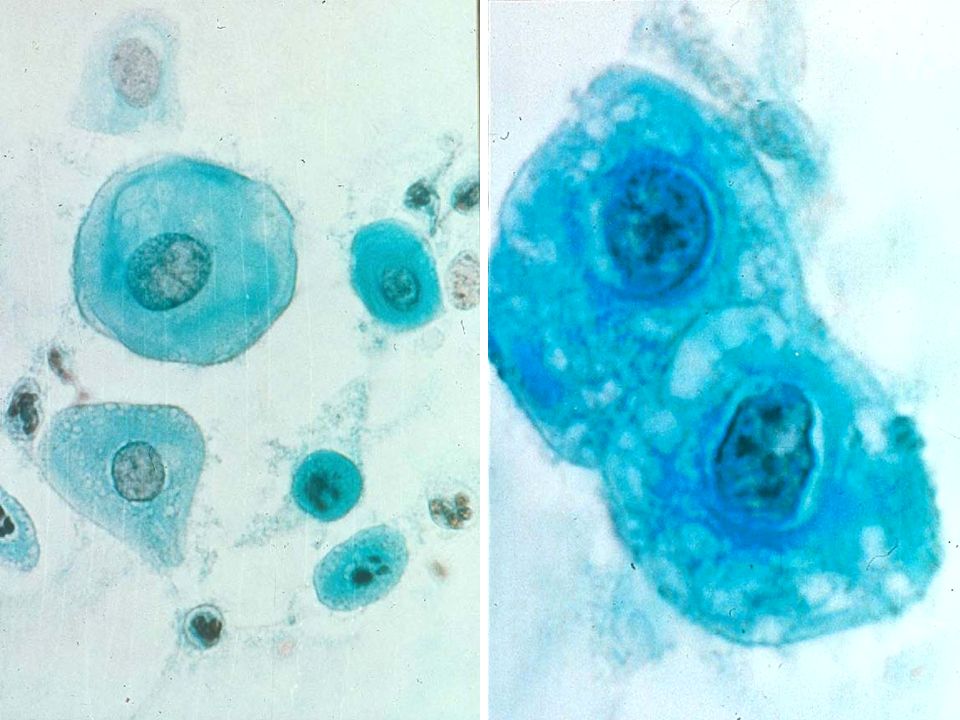
Normal endocervical cells

6
Endocervical Adenocarcinoma
Risk Factors; Estrogen High socio-economic status HPV Relation with squamous lesion; Endocervical adenoCa. → squamous lesion (>50%) Squamous lesion → adenocarcinoma (4%)
 Squamous lesion → adenocarcinoma (4%)")
7
Endocervical Adenocarcinoma
Epithelial dysplasia (atypical glandular cells) Adenocarcinoma in situ (AIS) Invasive adenocarcinoma Well differentiated adenocarcinoma without mucin formation Well differentiated mucus-secretory adenocarcinoma Poorly differentiated adenocarcinoma
 Adenocarcinoma in situ (AIS) Invasive adenocarcinoma. Well differentiated adenocarcinoma without mucin formation. Well differentiated mucus-secretory adenocarcinoma. Poorly differentiated adenocarcinoma.")
8
Adenocarcinoma in Situ (AIS)
10~25% of adenocarcinoma of the cervix Age: usually 10~20 yrs younger than invasive Ca. Symptom; Usually asymptomatic Vaginal bleeding Coexists with SIL or SqCC in 2/3 of cases

9
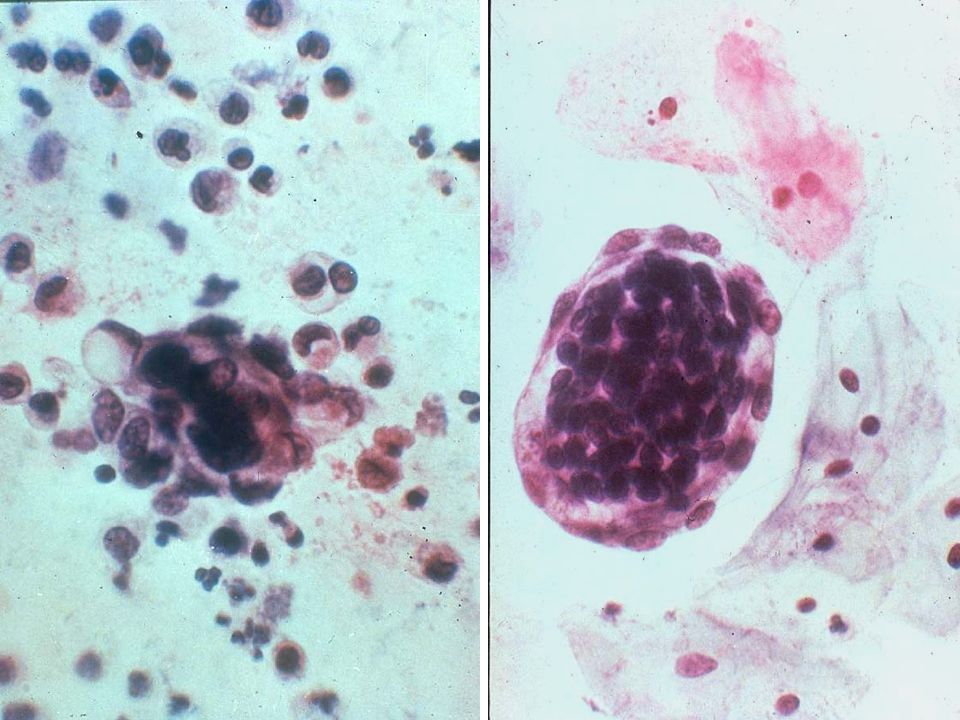
Cytologic Findings of AIS -Architectural Features-
Cohesive sheets and tissue fragments of varying size in clean background Loss of honeycomb pattern: crowding and overlap of nuclei Specific architectural features; Stratified strips of columnar epithelium Feathering (nuclear protrusion at group margins) Epithelial rosettes Crypt opening within an epithelial sheet
 Epithelial rosettes. Crypt opening within an epithelial sheet.")
10
Cytologic Findings of AIS -Architectural Features-
Exfoliation pattern; Cohesive sheets and tissue fragments of varying size in clean background

11
Cytologic Findings of AIS -Architectural Features-
Exfoliation pattern ; Loss of honeycomb pattern; crowding and overlap of nuclei

13
Cytologic Findings of AIS -Architectural Features-
Exfoliation pattern; Crypt opening may be seen within a sheet Strips pf columnar cells with crowded, basally oreinted nuclei and pale, foamy, or vacuolated cytoplasm

14
Cytologic Findings of AIS -Architectural Features-
Feathering; Perpendicular orientation of long axis Protrude radially

16
Cytologic Findings of AIS -Architectural Features-
Rosettes;

17
Cytologic Findings of AIS -Nuclear Features-
Higher than normal N/C ratio Nuclear enlargement with pleomorphism: elongation of nuclei common Distinctive coarsely granular, evenly distributed chromatin pattern Nucleoli are not typically prominent Mitoses and apoptotic bodies may be often present

19
Invasive Adenocarcinoma
8~25% of primary carcinoma of the cervix Age: usually 45~53 yrs Symptom; Watery discharge or vaginal bleeding Coexists with SIL or SqCC in 2/3 of cases

20
Invasive Adenocarcinoma
Well differentiated adenocarcinoma without mucin formation Well differentiated mucus-secretory adenocarcinoma Poorly differentiated adenocarcinoma

21
Well differentiated adenocarcinoma without mucin formation
Pattern: - Flat cell groups with nuclear crowding forming rosette pattern - Nuclear palisading arrangement, common Mitosis in 1/3 of the cases Cells: columnar with basal nuclei Nuclei: oval and hyperchromatic with coarse chromatin Nucleoli: may be present with halo

23
Well differentiated mucus-secretory adenocarcinoma
Pattern: papillary groups / disorganized honeycomb pattern with unequal vacuoles Nuclei: - hyperchromatic, anisokaryotic - flattened by large mucous vacuoles

24
Poorly differentiated adenoCa.
Pattern: Three-dimensional Cells: rounded Nuclei: round, hyperchromatic, several nucleoli, abnormal-shaped Cytoplasm: absent vacuoles Tumor diathesis: always present

25
Endocervical AIS vs. Invasive adenocarcinoma
In situ Adenocarcinoma Invasive Adenocarcinoma Architecture Crowded gland/sheet, strips, rosettes Irregular and crowded glands Pseudostratification Stratification with supercrowding Polarity preserved Loss of polarity Peripheral feathering Peripheral feathering may be present Cells: normal or small in size Cells: large N/C: high Single malignant cells: uncommon Single malignant cells: common Nucleus Large Large, pleomorphic Hyperchromasia with evenly distributed chromatin Hyperchromasia, clearing and irregularly distributed chromatin Inconspicuous nucleoli Prominent nucleoli Cytoplsam Focal mucin loss Secretion varies Background: Clear or bloody with intact RBCs Necroinflammatory of bloody, with broken-down RBCs

26
Distinguishing Points Between SqCC and Adenocarcinoma
Cell shape Polygonal Cuboidal, columnar Nuclei Central Eccentric Chromatin Coarse, compact Vesicular Nucleoli Not prominent Prominent Cytoplasm Thick , eosinophlic Thin, vacuoles Cell group Irregular Round, oval Lumen No Gland, acini, rosettes Row Yes

28
Endometrial Glandular Lesions
Endometrial hyperplasia Endometrial atypical hyperplasia and adenocarcinoma in situ Endometrial adenocarcinoma

29
“TBS” – Glandular cells
Atypical endocervical cells (NOS or specify in comments) endometrial cells (NOS or specify in comments) glandular cells (NOS or specify in comments) endocervical cells, favor neoplastic glandular cells, favor neoplastic Endocervical carcinoma in situ Adenocarcinoma endocervical, endometrial, extrauterine, NOS
 endometrial cells (NOS or specify in comments) glandular cells (NOS or specify in comments) endocervical cells, favor neoplastic. glandular cells, favor neoplastic. Endocervical carcinoma in situ. Adenocarcinoma. endocervical, endometrial, extrauterine, NOS.")
32
Endometrial hyperplasia
Should be suspected when benign endometrial cells are found 10 days after the end of the last menstrual period Abundance of thick clusters of reactive endometrial cells In postmenopausal women, any crowded clusters of reactive endometrial cells

35
Endometrial atypical hyperplasia and adenocarcinoma in situ (AIS)
Variable numbers of polymorphic endometrial cells Cytoplasm: abundant and eosinophilic Nuclei: enlarged with granular chromatin, irregularly distributed Nucleoli: often prominent

37
Normal Atypical hyperplasia Atypical hyperplasia, day 25

38
Malignant glandular lesions
Endometrial adenocarcinoma Detection rate; Cervical scraping only: 15% Vaginal pool smear and cervical scraping: 45% Endocervical aspiration & vaginal pool smears: 65% Intrauterine & endocervical aspiration and lavage: 90%

39
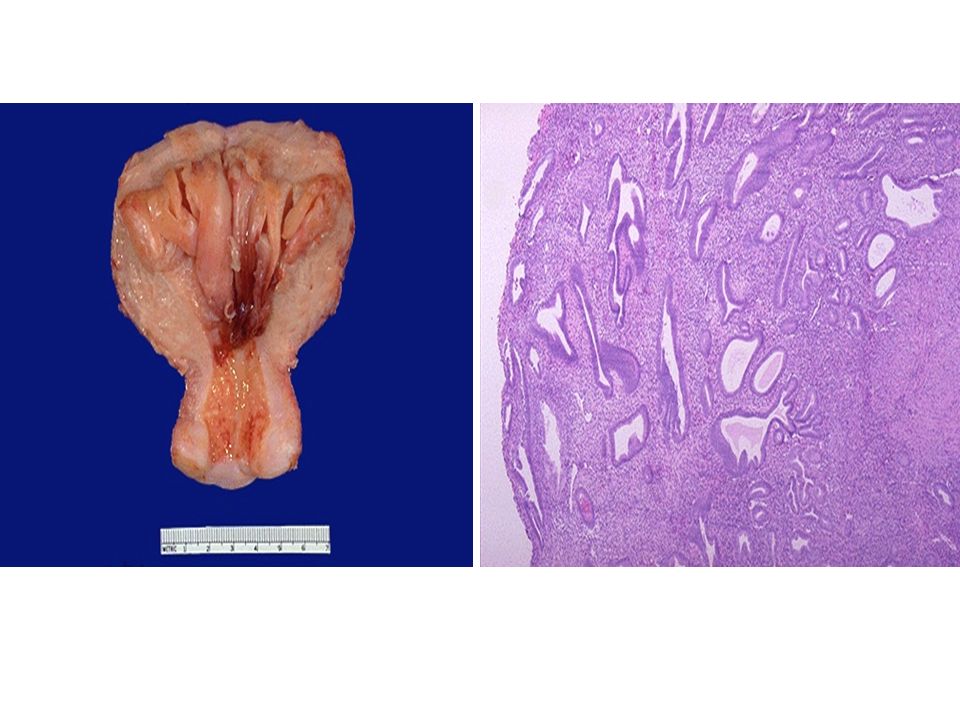
Endometrial adenocarcinoma
50-65세 Risk factors; Estrogen (granulosa cell tumor) - 독신자, 아이를 낳은 적이 없는 여자(불임) Obesity Hypertension Diabetes mellitus High socio-economic status
 - 독신자, 아이를 낳은 적이 없는 여자(불임) Obesity. Hypertension. Diabetes mellitus. High socio-economic status.")
40
Helpful hints for diagnosis of endometrial adenocarcinoma (1)
Presence of degenerate or well-preserved normal endometrial cells in a post-menopausal woman In an asymptomatic premenopausal woman, the presence of normal-appearing endometrial cells at mid-cycle or post-ovulatory time Presence of an increased number of small or large histiocytes, often with phagocytized necrotic cellular debris, in the non-atrophic smear of any post-menopausal woman (small: 4%, large: 17%)
")
41
Helpful hints for diagnosis of endometrial adenocarcinoma (2)
Increased number of foreign body giant cells in the non-atrophic smear of any post-menopausal woman Presence of unexplained fresh and old blood or an increase in necrotic debris or fibrin (tumor diathesis) in the smear of a post-menopausal woman A history of DM, obesity, hypertension, breast cancer, family history of breast and ovarian cancer, late menopause, or post-menopausal bleeding
 in the smear of a post-menopausal woman. A history of DM, obesity, hypertension, breast cancer, family history of breast and ovarian cancer, late menopause, or post-menopausal bleeding.")
42
General diagnostic cellular criteria in endometrial adenocarcinoma
Number of diagnostic cells: very scanty or abundant Imitate the appearance of the benign columnar cells (arranged in row) Shed in tight clumps, in loose clusters, or singly Background: usually dirty (tumor diathesis)
 Shed in tight clumps, in loose clusters, or singly. Background: usually dirty (tumor diathesis)")
44
Differentiation Well Moderate Poor

46
DDx. between endometrial and endocervical adenocarcinoma
Number of cells Less abundant Abundant Degeneration Marked Mild Size 160±40 u2 190±60 u2 Ingestion of leukocytes Rare Nuclear size 60±10 u2 80±20 u2 Chromatin Moderately coarse Finely granular Nucleoli Multiple 20%, Macronucleoli 20% Multiple 60%, Macronucleoli 40% Background Very dirty Relatively clean Squamous dyskaryosis Very rare Occasional

47
Effects of Irradiation and Other Techniques
Cellular changes from radiotherapy; Inhibit the formation of DNA or RNA or cause cross-links and breaks in the DNA double strands of benign & malignant cells (G2-M) Cytoplasm: more abundant, may have peri-nuclear halo Nuclei: - often enlarged and hyperchromatic with prominent Nu. - differ from dysplasia or cancer cells by (1) finely granular or amorphous chromatin (2) smooth regularity of the nuclear membrane
 Cytoplasm: more abundant, may have peri-nuclear halo. Nuclei: - often enlarged and hyperchromatic with prominent Nu. - differ from dysplasia or cancer cells by. (1) finely granular or amorphous chromatin. (2) smooth regularity of the nuclear membrane.")
48
Cellular changes from radiation (radiation response)
Mechanism of action; 1. Prevent the synthesis of DNA proteins → rapid death of cells 2. Inhibit cellular mitosis 3. Change the chromosomal or genetic information of cells Radiation responses = cellular changes resulting from irradiation appear first in the nuclei, then in the cytoplasm

49
Cellular changes from radiation (radiation response)
Some irradiation cellular changes may persist for the whole life of patients Acute reaction : - appear about 1 day after the start of irradiation and continue for 6 weeks after the end of the treatment - cellular necrosis and increase in the exfoliation of degenerated, nonviable, benign or malignant cells Healing stage: mixed with repair & inflammatory cells

51
Cellular changes from radiation (radiation response)
Cytoplasmic changes; Similar changes in chemotherapy, UV irradiation, or cautery 1) Edema and hypertrophy (3~4 times) 2) Biphasic stain and loss of normal fine granularity → amorphous, homogeneous, amphophilic, or eosinophilic 3) Cytoplasmic fibrils, often seen in concentric or irregular 4) Vacuolization 5) Pseudo-cannibalism 6) Cytoplasmic fragments and naked nuclei: -mainly in the late stage of irradiation -indicate the death of cells
 Edema and hypertrophy (3~4 times) 2) Biphasic stain and loss of normal fine granularity. → amorphous, homogeneous, amphophilic, or eosinophilic. 3) Cytoplasmic fibrils, often seen in concentric or irregular. 4) Vacuolization. 5) Pseudo-cannibalism. 6) Cytoplasmic fragments and naked nuclei: -mainly in the late stage of irradiation. -indicate the death of cells.")
52
Cellular changes from radiation (radiation response)
Changes in the nuclei; 1) Nuclear hypertrophy (2-10 times): - most consistent and common changes - may be extremely irregular, with nuclear wrinkling 2) N/C ratio remains within the normal limits 3) Peri-nuclear halo, sometimes with pyknotic nuclei 4) Vacuolization: indicates death of the cell 5) Chromatin (the amount of DNA): -increases but finely granular & uniformly distributed -decreases: pale and empty-appearing nuclei 6) Multi-nucleation
 Nuclear hypertrophy (2-10 times): - most consistent and common changes. - may be extremely irregular, with nuclear wrinkling. 2) N/C ratio remains within the normal limits. 3) Peri-nuclear halo, sometimes with pyknotic nuclei. 4) Vacuolization: indicates death of the cell. 5) Chromatin (the amount of DNA): -increases but finely granular & uniformly distributed. -decreases: pale and empty-appearing nuclei. 6) Multi-nucleation.")
53
Other irradiation changes;
7) Nucleoli: enlarged, remain round and regular in shape 8) Changes indicating the death of the cells (benign or malignant) (1) Peripheral condensation of the chromatin (2) Vacuolization (3) Fragmentation (4) Nuclear pyknosis (5) Karyorrhexis Other irradiation changes; 1) Soon after irradiation: large No. of inflammatory cells 2) In the healing stage: an increase in repair cells 3) Increase in mucus secretion during radiation
 Nucleoli: enlarged, remain round and regular in shape. 8) Changes indicating the death of the cells. (benign or malignant) (1) Peripheral condensation of the chromatin. (2) Vacuolization (3) Fragmentation (4) Nuclear pyknosis. (5) Karyorrhexis. Other irradiation changes; 1) Soon after irradiation: large No. of inflammatory cells. 2) In the healing stage: an increase in repair cells. 3) Increase in mucus secretion during radiation.")
57
Cytology of irradiated malignant lesions
During RTx. & in the 2 wks following it; (1) Cancer cells are shed in large numbers (2) Absence of cancer cells may indicate a poor prognosis (3) Most of malignant cells show irradiation changes similar to those described for benign cells (4) The diagnosis of persistent carcinoma should not be made at this time, because the exfoliated cells with these changes are dead or are still alive (5) The death of a malignant cell should be suspected when the nucleus show pyknosis, karyorrhexis, and karyolysis or vacuolization.
 Cancer cells are shed in large numbers. (2) Absence of cancer cells may indicate a poor prognosis. (3) Most of malignant cells show irradiation changes. similar to those described for benign cells. (4) The diagnosis of persistent carcinoma should not be. made at this time, because the exfoliated cells with. these changes are dead or are still alive. (5) The death of a malignant cell should be suspected. when the nucleus show pyknosis, karyorrhexis, and. karyolysis or vacuolization.")
58
Cytology of irradiated malignant lesions
B. 4 wks after irradiation; (1) The presence of malignant cells showing minimal irradiation changes suggest the possibility of persisting cancer (2) These cells usually have the same features as the original non-irradiated malignant cells
 The presence of malignant cells showing minimal irradiation changes suggest the possibility of persisting cancer. (2) These cells usually have the same features as the original non-irradiated malignant cells.")
59
Cytology of irradiated malignant lesions
C. Recurrence of carcinoma; (1) Should be suspected when malignant cells appear after an interval of smears free of tumor cells (2) Recurrent cancer cells tend to be smaller and less differentiated D. All patients after radiotherapy; Need to be closely followed by periodic repeated smears, taken every 3 ~ 6 months
 Should be suspected when malignant cells appear after an interval of smears free of tumor cells (2) Recurrent cancer cells tend to be smaller and less differentiated D. All patients after radiotherapy; Need to be closely followed by periodic repeated smears, taken every 3 ~ 6 months")
61
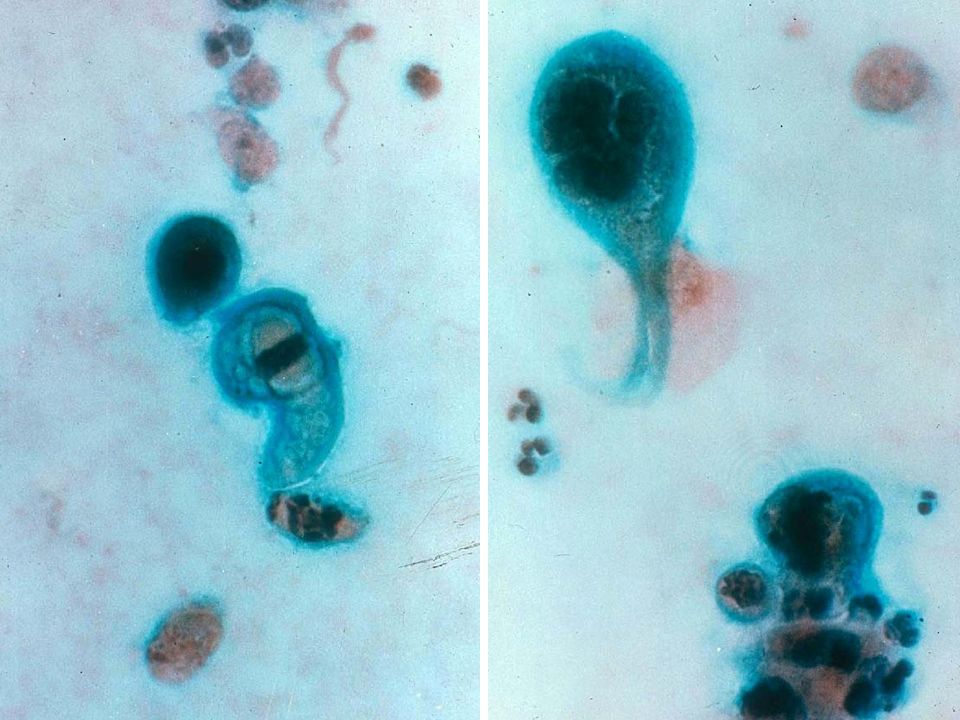
SqCC, radiotherapy 2 wks

62
Endometrial adenoCa, radiotherapy 3 wks

63
Cellular changes from chemotheraphy
Similar to cellular changes of irradiation Systemic effect Cyclophosphamide (urinary bladder) & busulfan (lung, pancreas, spleen, urinary tract, uterine cervix) More prominent in nuclei Atrophic smear Need close long-term follow-up: 3 ~ 6 months
 & busulfan (lung, pancreas, spleen, urinary tract, uterine cervix) More prominent in nuclei. Atrophic smear. Need close long-term follow-up: 3 ~ 6 months.")
64
수고했습니다

Similar presentations

















>")








>")




