Download presentation
Presentation is loading. Please wait.

1
Precancerous lesion of FGT

2
Premalignant or precancerous lesions are epithelial changes of the FGT, which if left without treatment could progress (over an interval; may extend into several years) into carcinoma.
 into carcinoma.")
3
The general features of precancerous cells
Loss of stratification: loss of the normal arrangement of epithelial cells into layers. Distorted cells with enlarged irregular hyperchromatic nuclei. Increased Nuclear / Cytoplasm (N/C) ratio Nuclear mitosis are present at high level at the top layer more than the basal layers.
 ratio. Nuclear mitosis are present at high level at the top layer more than the basal layers.")
4
Types of precancerous lesions
Epithelial endometrial and cervical hyperplasia Leukoplakia: patches of keratosis. It is visible as adherent white patches on the mucous membranes. Atypical squamous metaplasia of the cervix Parakeratosis: mode of keratinization characterized by the retention of nuclei in the stratum corneum. Cervical dysplasia: abnormality of development show expansion of immature cells, with decrease in the number and location of mature cells. Endocervical polyp (Adenoma of the cervix) Cervical intraepithelial neoplasm (CIN)
 Cervical intraepithelial neoplasm (CIN)")
5
Epithelial hyperplasia

6
Cervical hyperplasia Squamous cell hyperplasia:
Thickness of the whole epithelium due to chronic irritation. Basal cell hyperplasia: Hyperactive proliferation of the basal cell layer to form several layers instead one or two layers. Reserve cell hyperplasia: Presence of patchy layer of small cells immediately beneath basal cell layer.

7
Endometrial hyperplasia
Endometrial hyperplasia is overgrowth of both glandular and stromal endometrial layers due to over-stimulation by estrogen . Types: Mild (cystic) hyperplasia (G I) Moderate (adenomatous) hyperplasia (GII) Sever (atypical) hyperplasia (GIII)
 hyperplasia (G I) Moderate (adenomatous) hyperplasia (GII) Sever (atypical) hyperplasia (GIII)")
8
Cervical smear: Thick clusters of reactive endometrial cells with or without atypia.
N.B. Sever atypical endometrial hyperplasia is considered as GI (well differentiated) endometrial adenocarcinoma.
 endometrial adenocarcinoma.")
9
Cervical atypical squamous metaplasia
Definition: It is a transformation of the fragile cervical cells at the squamo-columnar junction of endocervical canal into more resistant stratified squamous epithelial cells with cellular atypia. Cervical smear: Squamous cells with a nuclear enlargement (increased N/C ratio), binucleated, irregular nuclear membrane and slightly hyperchromasia.
, binucleated, irregular nuclear membrane and slightly hyperchromasia.")
11
Endocervical polyp (cervical adinoma)
Definition: It is a pedunculated vascular connective tissue core containing inflammatory cells (acute & chronic), with dilated endocervical glands, and covered by ulcerated cervical epithilium or squamous metaplasia
, with dilated endocervical glands, and covered by ulcerated cervical epithilium or squamous metaplasia.")
12
Cervical dysplasia Cervical intraepithelial neoplasia (CIN)
Definition: It is an abnormal growth or disordered development of primitive immature basal cell layer and abnormal cell maturation; i.e. begin in the lower portion of cervical epithelium. Site: Usually at squamo-columnar junction ; it may be multifocal and involve the endocervical cleft.

13
Features of cytological smears of dysplastic cells
Enlarged hyperchromatic nucleus ( N/C ratio). Increased number of abnormal mitotic figures according to the severity of dysplasia Nuclear chromatin clumping.
. Increased number of abnormal mitotic figures according to the severity of dysplasia. Nuclear chromatin clumping.")
14
Classification (types) of Dysplasia (CIN)
Dysplasias are subclassified according to the degree by which the epithelium is replaced by immature dysplastic cells;- Mild (GI) CIN dysplasia: involve the lower 1/3 of the cervical epithelium. Moderate (GII) CIN dysplasia: involve the lower 2/3of the cervical epithelium. Severe (GIII) CIN dysplasia or carcinoma in situ: involve the whole thickness of the covrring epithelium
 CIN dysplasia: involve the lower 1/3 of the cervical epithelium. Moderate (GII) CIN dysplasia: involve the lower 2/3of the cervical epithelium. Severe (GIII) CIN dysplasia or carcinoma in situ: involve the whole thickness of the covrring epithelium.")
15
Cervical Disease Progression in Cells of the Basement Membrane
Normal squamous epithelium HSIL Koilocytosis LSIL Mild Moderate in situ Severe Carcinoma CIN1 CIN2 CIN3 Dysplasia This illustration shows progressive degrees of dysplasia and neoplasia in the cervical epithelium basement membrane. Note how the degrees of dysplasia are categorized. LSIL cells are identified as either koilocytosis or CIN 1 (mild dysplasia), and both of these are considered the same. HSIL cells are identified as either CIN 2 (moderate dysplasia) or CIN3 (severe dysplasia). CIN 3 and carcinoma in situ are the same histologic diagnosis. Beyond CIN 3 is invasive carcinoma. Koilocytosis - Cell changes showing perinuclear vacuolization LSIL - Low-grade Squamous Intraepithelial Lesion HGSIL or HSIL - High-grade Squamous Intraepithelial Lesion CIN - Cervical Intraepithelial Neoplasia CIN1 - Mild dysplasia CIN2 - Moderate dysplasia CIN3 - Severe dysplasia to carcinoma in situ (CIS) 15
, and both of these are considered the same. HSIL cells are identified as either CIN 2 (moderate dysplasia) or CIN3 (severe dysplasia). CIN 3 and carcinoma in situ are the same histologic diagnosis. Beyond CIN 3 is invasive carcinoma. Koilocytosis - Cell changes showing perinuclear vacuolization. LSIL - Low-grade Squamous Intraepithelial Lesion. HGSIL or HSIL - High-grade Squamous Intraepithelial Lesion. CIN - Cervical Intraepithelial Neoplasia. CIN1 - Mild dysplasia. CIN2 - Moderate dysplasia. CIN3 - Severe dysplasia to carcinoma in situ (CIS) 15.")
16
Precursor Lesions of Cervical Carcinoma
LSIL HSIL CIN CIN CIN 3 Normal Mild Moderate Severe Carcinoma Dysplasia Dysplasia Dysplasia in situ Precancerous Lesions of the Cervix. LSIL = Low Grade Squamous Intraepithelial Lesion CIN = Cervical Intraepithelial Neoplasia HSIL = High Grade Squamous Intraepithelial Lesion

17
Above, left. Squamous carcinoma in situ (CIS), cervix
Above, left. Squamous carcinoma in situ (CIS), cervix. To the right is normal squamous epithelium with its basal cell layer & orderly maturation upwards. The left side shows CIS characterized by lack of maturation, altered cell polarity, nuclear pleomorphism & increased nuclear / cytoplasmic ratio. As is characteristic of CIS, neoplastic cells are confined to the epithelial layer & have not invaded through the epithelial basement membrane, under which, the submucosal stroma contains chronic inflammatory cells.
, cervix. To the right is normal squamous epithelium with its basal cell layer & orderly maturation upwards. The left side shows CIS characterized by lack of maturation, altered cell polarity, nuclear pleomorphism & increased nuclear / cytoplasmic ratio. As is characteristic of CIS, neoplastic cells are confined to the epithelial layer & have not invaded through the epithelial basement membrane, under which, the submucosal stroma contains chronic inflammatory cells.")
18
A B C D

19
Carcinoma of the cervix

20
1- Carcinoma in situ: It is a lesion in which all thickness of cervical epithelium is replaced by malignant cells without invasion of the underlying stroma; i.e. with intact basement membrane.

21
2- Micro-invasive carcinoma
These are buds of malignant epithelial cells invading the cervical stroma beneath the carcinoma in situ to a depth of 2-3 mm from the site of the origin, without lymphatic or vascular invasion.

22
3- Invasive carcinoma Malignant epithelial cells that invade the underlying stroma of the cervical epithelium by infiltration or destruction of the basement membrane, with or without lymphatic or vascular invasion.

23
Types of invasive carcinoma
Primary type Secondary type Squamous cell carcinoma Adenocarcinoma Adeno-squamous carcinoma Adeno-acanthoma (squamous cell mataplasia + adenocarcinoma). Choriocarcinoma (Malignant tumor of the placenta). Metastatic
. Choriocarcinoma (Malignant tumor of the placenta). Metastatic.")
24
Cytology of malignant cells

25
Cytological features of normal and benign tumors
The cells are uniform in size and shape. The cells are uniform in nuclear and cytoplasmic ratio. The normal C/N = ½ Normal polarity (normal arrangement of cells to neighbouring cells). In benign tumors, the appearance of cells are usually give normal appearance of origin cells; E.g. fibroma: show the increased number of normal appearance of fibroblasts.
. In benign tumors, the appearance of cells are usually give normal appearance of origin cells; E.g. fibroma: show the increased number of normal appearance of fibroblasts.")
26
Cytological features of malignant tumors

27
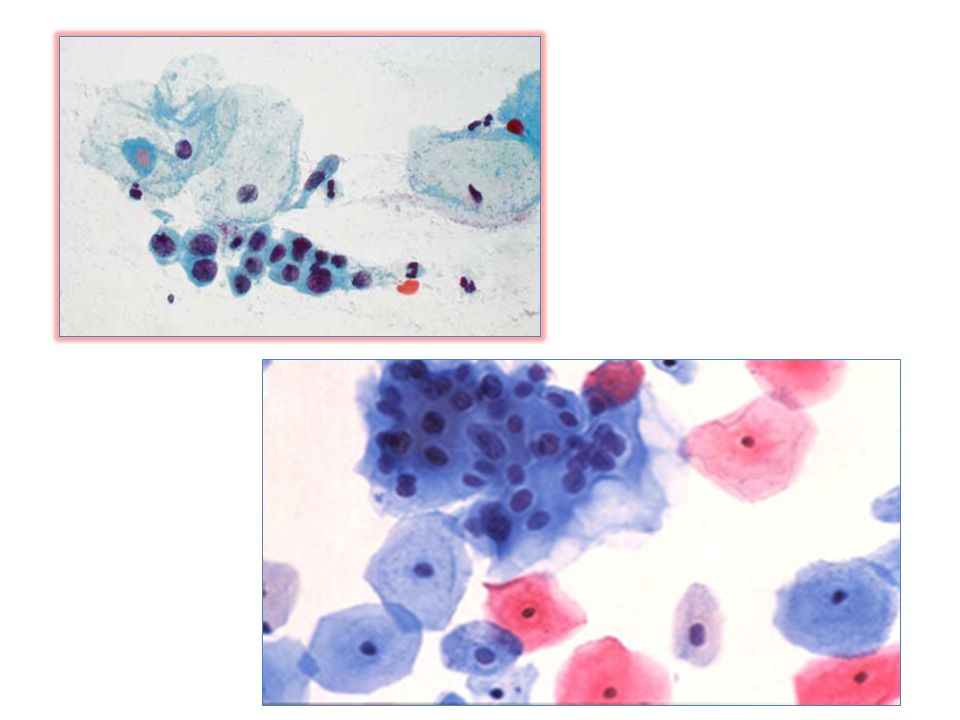
A and B: mature squamous metaplasia.
C: immature squamous metaplasia. D: immature squamous metaplasia with pattern of transitional metaplasia.

28
Cervical dyskaryosis Changes in nuclear-cytoplasmic ratio
Changes in nucleoli Changes in mitotic index Severe dyskaryosis Atypical immature metaplastic squamous cells with increased nuclear/cytoplasmic ratio and hyperchromasia. Mild-moderate dyskaryosis Squamous carcinoma

29
1- Nuclear criteria Nuclear enlargement
Nuclear shape and size variation Disturbed chromatin (abnormal chromatin distribution in the nucleus) Changes of nuclear membrane Irregular enlarged prominent nucleoli. Multinucleated malignant giant cells Abnormal mitosis Hyperchromasia: deep blue hyperchromatic nuclei due to increase DNA content of the nucleus.
 Changes of nuclear membrane. Irregular enlarged prominent nucleoli. Multinucleated malignant giant cells. Abnormal mitosis. Hyperchromasia: deep blue hyperchromatic nuclei due to increase DNA content of the nucleus.")
30
Enlarged nuclei with increased N/C ratio
Enlarged nuclei with irregular nuclear membrane

31
2- Cytoplasmic criteria
Scanty cytoplasm Increased N/C ratio Tight holding of membrane around nucleus Secretory or inclusion of cytoplasm

32
3- Malignant cells intrcellular relationship
Variation of the size and shape of malignant cells Decreased cohesiveness between cells Abnormal stratification and polarity

33
General consideration about malignant criteria
1- No single morphologic malignant criteria alone is pathogenic for malignancy; a combination of criteria is necessary. 2- Nucleus is the most important part of the ell to show malignant changes; but the cytoplasmic changes could help in cell differentiation and cell typing.

34
3- The presence of acini or papillae in an abnormal location (such as in pleural cavity) increase suspicion of malignancy even in absence of the prominent features of malignancy because of their high degree of differentiation. So, the question should always to be answered in this form: - It is a cancer? - What type of cancer is it?

35
Factors affecting the distribution of malignant cells
Collection and processing technique: Direct smearing or scraping exfoliate malignant cells in clusters or sheets rather than isolated cells in spontaneous exfoliation (aspiration).
.")
36
Nature of the lesion: Adenocarcinoma exfoliate malignant cells in clusters as acini or papillary structures. Dysplastic cells and carcinoma in situ of squamous cell carcinoma single scattered exfoliated squamous cancer cells throughout the smear. Sarcomatous cells are usually arranged as single malignant cells and are separated by thin fibrous tissue.

Similar presentations






 Reactive endocervical cells B) HSIL C) LSIL D) Squamous metaplasia E) ASCUS 1.>")


 {AJCC} from Cummings.please see handouts as well for updated AJCC Tx Minimum requirements.>")

>")







