Download presentation
Presentation is loading. Please wait.

1
CARDIAC EXAMINATION

2
GENERAL EXAMINATION Introduce yourself to the patient & take permission. HANDS: cyanosis, clubbing (congenital cyanotic heart disease, infective endocarditis), tar stain, palmar erythema, osler nodes, jenway lesions. PULSE: rate, regularity, volume, special character, equal in both sides, peripheral pulses r felt.
, tar stain, palmar erythema, osler nodes, jenway lesions. PULSE: rate, regularity, volume, special character, equal in both sides, peripheral pulses r felt.")
3
PULSE RATE newborn (0–3 months old) infants (3 – 6 months)
children (1 – 10 years) children over 10 years & adults, including seniors well-trained adult athletes 90–120 80-120 70–130 60–100 40–60 PULSE RATE
 children over 10 years & adults, including seniors. well-trained adult athletes – – – –60. PULSE RATE.")
4
PULSE VOLUME

5
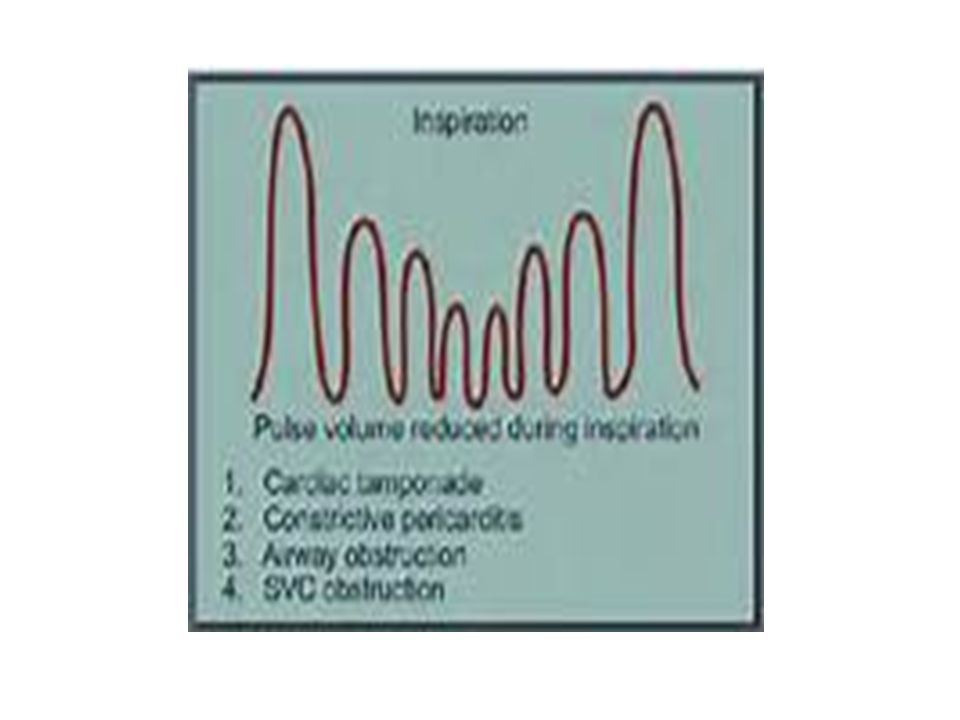
PULSE PATTERNS Pulsus alternans: an ominous medical sign that indicates progressive systolic heart failure. To trained fingertips, the examiner notes a pattern of a strong pulse followed by a weak pulse over and over again. This pulse signals a flagging effort of the heart to sustain itself in systole. Pulsus bigeminus: indicates a pair of hoofbeats within each heartbeat. Concurrent auscultation of the heart may reveal agallop rhythm of the native heartbeat. Pulsus bisferiens: an unusual physical finding typically seen in patients with aortic valve diseases. If the aortic valve does not normally open and close, trained fingertips will observe two pulses to each heartbeat instead of one. Pulsus tardus et parvus or anacrotic pulse: a slower than normal rise in the tactile pulse caused by an increasingly stiff aortic valve. Loss of compliance in the aortic valve makes it progressively harder to open, thus requiring increased generation of blood pressure in the left ventricle. Pulsus paradoxus: a condition in which some heartbeats cannot be detected at the radial artery during the inspiration phase of respiration. It is caused by an exaggerated decrease in blood pressure during this phase, and is diagnostic of a variety of cardiac and respiratory conditions of varying urgency.

6
PULSE PATTERN

8
Face: Dawn, Turner, Noonan or Marfan features.
Eyes: jaundice (infective endocarditis, dysfunction valve), anemia (heart failure). Mouth: tongue (cyanosis), dental care ( infective endocarditis), lost teeth ( poor diabetic control).
, anemia (heart failure). Mouth: tongue (cyanosis), dental care ( infective endocarditis), lost teeth ( poor diabetic control).")
9
JUGULAR VENOUS PRESSURE
Patient reclining with head elevated 45 ° Measure elevation of neck veins above the sternal angle (Lewis Method). Add 5 cm to measurement since right atrium is 5 cm below the sternal angle. Normal CVP <= 8 cm H2O Light should be tangential to illuminate highlights and shadows.
. Add 5 cm to measurement since right atrium is 5 cm below the sternal angle. Normal CVP <= 8 cm H2O. Light should be tangential to illuminate highlights and shadows.")
11
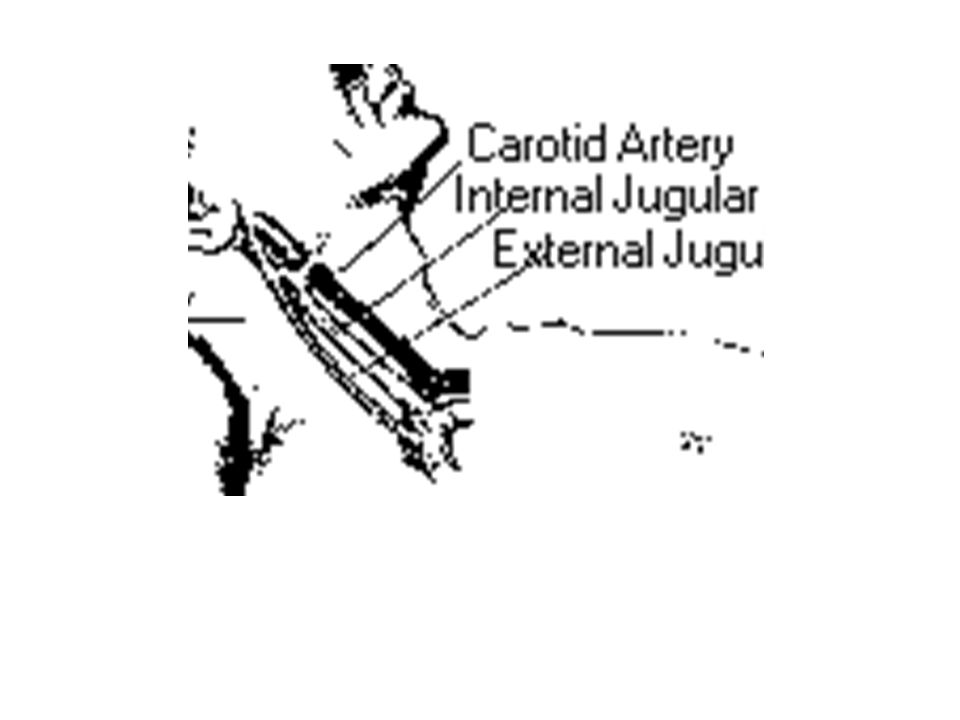
CAROTID ARTERY NECK VEINS
Medial anterior Lateral to sternomastoid Posterior triangle ANATOMICAL Jerky/sharp/outward felt Wavy/diffuse/inward seen CHARACTER ---- definite UPPER LEVEL persist Disappear by pressure at root of neck COMPRESSION engorge HEPATOJUGULAR PR. Reduce with siting POSITION Increased by inspiration RESPIRATION

12
Inspect on one side & feel the carotid on the other side: pulse = S1

13
The " a " wave corresponds to right Atrial contraction and ends synchronously with the carotid artery pulse. The peak of the 'a' wave demarcates the end of atrial systole. The " c " wave corresponds to right ventricular Contraction causing the triCuspid valve to bulge towards the right atrium. The " x " descent follows the 'a' wave and corresponds to atrial relaXation and rapid atrial filling due to low pressure The " v " wave corresponds to Venous filling when the tricuspid valve is closed and venous pressure increases from venous return - this occurs during and following the carotid pulse. The " y " descent corresponds to the rapid emptYing of the atrium into the ventricle following the opening of the tricuspid valve.

14
JVP ABNORMALITIES Raised JVP, normal waveform
Bradycardia Fluid overload Heart Failure Raised JVP, absent pulsation Superior vena cava syndrome Large 'a' wave (increased atrial contraction pressure) tricuspid stenosis Right heart failure Pulmonary hypertension
 tricuspid stenosis. Right heart failure. Pulmonary hypertension.")
15
Cannon 'a' wave (atria contracting against closed tricuspid valve)
Atrial flutter Premature atrial rhythm (or tachycardia) third degree heart block Ventricular ectopics Ventricular tachycardia Absent 'a' wave (no unifocal atrial depolarisation) atrial fibrillation Large 'v' wave (c-v wave) Tricuspid regurgitation Absent 'x' descent Tricuspid regurgitation (sometimes 'x' wave is replaced by a positive wave)
 third degree heart block. Ventricular ectopics. Ventricular tachycardia. Absent a wave (no unifocal atrial depolarisation) atrial fibrillation. Large v wave (c-v wave) Tricuspid regurgitation. Absent x descent. Tricuspid regurgitation (sometimes x wave is replaced by a positive wave)")
16
Prominent & Deep 'y' descent
Prominent 'x' descent Constrictive pericarditis Slow 'y' descent Tricuspid stenosis Cardiac tamponade Prominent & Deep 'y' descent Parodoxical JVP (Kussmaul's sign: JVP rises with inspiration, drops with expiration) Pericardial effusion Pericardial tamponade
 Pericardial effusion. Pericardial tamponade.")
17
LOWER LIMB EXAMINATION
Inspect for atrophic changes, diabetic skin changes, scar on the medial side of the knee. Ask for pain, assess for edema, then peripheral pulsation: dorsalis pedis along distal 1/3 of ext. hallucis longus, tendon came prominent with extension of big toe, posterior tibialis midway between medial malleolus & heal & if not felt popliteal with your both thumbs on the patella& fingers pushing in popliteal fossa

18
PRECORDIAL EXAMINATION
Inspection: at foot of bed for precordial pulge in congenital heart disease or midsternotomy scar, inframammary, gynecomastia in pt taking spironolactone then inspect for apex beat (the outermost, lower most beat). Palpation put palmar surface of your fingers over the visible apical beats or the suspected anatomy (inframammary between midclavicular & anterior axillary) & comment on palpable first heart sound, character as hyperdynamic or tapping then if there is thrill)
. Palpation put palmar surface of your fingers over the visible apical beats or the suspected anatomy (inframammary between midclavicular & anterior axillary) & comment on palpable first heart sound, character as hyperdynamic or tapping then if there is thrill)")
19
APEX BEATS

20
Put pad of your hand on the Lt
Put pad of your hand on the Lt. parasternal line for parasternal heave (Rt. Ventricular hypertrophy). Put tips of your fingers in the Lt,Rt. Intercostal spaceas to feel papable second sound & if thril felt put the pad of your hand on the sound felt & fingers on the carotid in same side to detect the propagation of the thril to the neck.
. Put tips of your fingers in the Lt,Rt. Intercostal spaceas to feel papable second sound & if thril felt put the pad of your hand on the sound felt & fingers on the carotid in same side to detect the propagation of the thril to the neck.")
21
AUSCULTATION Palpate carotid pulse by 2fingers at the upper medial border of the sternomastoid muscle at the level of the cricoid cartilage & press to differentiate S1, S2. then remove fingers & comment on intensity of heart sounds, if murmur comment on timing, site of maximum intensity, radiation & if increased by certain posture.

23
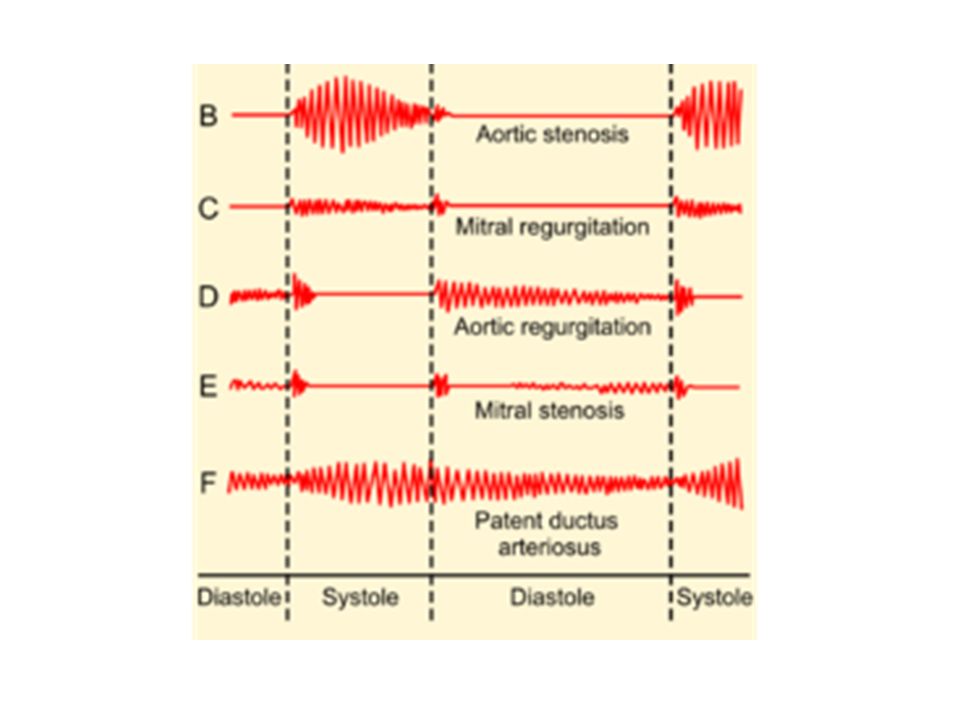
Mitral murmur: left lateral decubitis + valsalva.
Tricuspid murmur: sitting upright. Aortic & metallic murmur: leaning forward and exhaling with the metallic best heard over the lower half of the left sternal border. Systolic murmur radiate: mitral to anterior axillary line, tricuspid to apex, pulmonary to Lt.carotid, aortic to Rt.carotid. Aortic regurge best heard over A2 in the 3rd,4th intercostal space in Lt. parasternal line.

24
DIAGNOSIS I had pleasure to examine this gentlman with pulse, JVP, general manifestation of heart failure or infective endocarditis. Valve lesions, discribe & possible underlying cause (young: congenital/rheumatic/collagen—old: ischemic/cardiomyopathy/degenerative). Metallic ( which valve/complication as dysfunction..diastolic murmur or systolic radiating or heart failure/ overcoagulation as bleeding,ecchymosis or undercoagulation as FND)
. Metallic ( which valve/complication as dysfunction..diastolic murmur or systolic radiating or heart failure/ overcoagulation as bleeding,ecchymosis or undercoagulation as FND)")
Similar presentations



















Chapter (8) Assessment of Cardiovascular SystemAssessment of Cardiovascular System.>")