Download presentation
Presentation is loading. Please wait.

1
NEOPLASIA (M ) Dr. Mohammed Alorjani, MD EBP
 Dr. Mohammed Alorjani, MD EBP")
2
Definitions: Neoplasm = New growth of
transformed cells producing a mass What are TRANSFORMED cells? Cells that have undergone several mutations leading to features of: Uncontrolled growth Uselessness Persistence

3
According to behavior, two main types of neoplasms:
Benign neoplasm = Limited new growth without local invasion or spread Malignant neoplasm = invasive growth locally, which also spreads to distant sites. Both are of many types

4
Cancer is a general term for all malignant growths of whatever type
Oncology: study of tumors in all their aspects

5
NEOPLASM: Abnormal mass of tissue, the growth of which EXCEEDS and is UNCOORDINATED with that of the normal tissues, and PERSISTS in the same way even AFTER REMOVAL of the stimulus which produced the change.

6
Classification of neoplasms:
What is the purpose of classification? To provide help in diagnosis To allow correct treatment

7
How are tumors Classified?
Cell of origin Behavior of tumor Degree of differentiation

8
Structure of neoplasms:
Parenchymal cell & Stromal cell Amount & type of stromal cells may contribute to the consistency and appearance of tumors If there is stromal proliferation hardness of the tumor Scirrhous tumor Desmoplasia If there is lack of stromal cells, the tumor may be soft or cystic

9
The parenchymal cell may arise from:
A- One germ cell layer: Endoderm Mesoderm Ectoderm e.g: epithelial cell, connective tissue; e.g. endothelial cell, blood , BM, lymph node, others… B- More than one germ layer **Mixed tumors: from one or more germ cell layer

10
Serous cystadenoma of ovary

11
Scirrhous Carcinoma of breast

12
Epithelial Cell Origin
- Benign Epithelial tumors: Adenoma - Glandular epithelial tumor often producing a secretion e.g. (mucin) which may be intraepithelial or intraluminal * Cystadenoma
 which may be. intraepithelial or intraluminal. * Cystadenoma.")
13
Papilloma - Epithelial tumor forming finger-like fronds/projections from any epithelial surface, with a connective tissue core/center. Polyp - General term: !neoplastic/non-neoplastic! Projecting from the mucosal surface of a hollow organ

14
Squamous Papilloma

15
Structure of Adenoma (Adenomatous Polyp)
")
16
- Malignant epithelial tumors (Carcinomas):
Squamous cell carcinoma e.g. skin, mouth, cervix, bronchus…etc Adenocarcinoma from glandular origin, e.g. G.I.T., endometrium, breast, kidney, thyroid…etc

17
Connective tissue cell origin:
- Benign: Named by tissue of origin with attached suffix – oma e.g. fibroma, lipoma, chondroma…etc

18
- Malignant connective tissue tumors:
SARCOMA: Prefix (origin)+ suffix (sarcoma) e.g. Osteosarcoma, liposarcoma, angiosarcoma, leiomyosarcoma, rhabdomyosarcoma…
+ suffix (sarcoma) e.g. Osteosarcoma, liposarcoma, angiosarcoma, leiomyosarcoma, rhabdomyosarcoma…")
19
Nomenclature: Cell of origin + Suffix
Suffix - oma Fibroma Osteoma Adenoma Papilloma Chondroma Carcinoma / Sarcoma Fibrosarcoma Osteosarcoma Adencarcinoma Squamous cell carcinoma Chondrosarcoma Exceptions: Leukemia, Lymphoma, Glioma, Melanoma…

20
Some tumors are MIXED !!!

21
Mixed Tumors: OR: Single germ cell tumors:
Derived from one germ cell layer that differentiates into more than one cell type.. e.g. *Mixed tumor of Salivary Gland, *Fibroadenoma of breast OR:

22
Teratomas: Made of a variety of parenchymal cell types that derive from more than one germ cell layer formed by totipotential germ cells that are able to form ectoderm, endoderm & mesoderm

23
TERATOMA continued: May be benign or malignant depending on structure, site, age, sex… May contain skin, sebaceous & mucus glands, hair, cartilage, bone, teeth, respiratory epithelium, glial tissue…etc. Usual location is ovary or testis

24
Dermoid cyst of ovary (a component of benign cystic teratoma)
Iowa Collection

25
A microscopic view of a similar tumor shows sebaceous glands, respiratory epithelium, bone, and bone marrow.

26
Tumors of primitive fetal origin: Blastoma: from immature tissue
May arise in kidney, liver, retina…etc e.g. * Nephroblastoma * Retinoblastoma The great majority of these tumors are malignant & occur in infants & children

27
Some tumors have names that do not conform with general rules:
Melanomas arise from nevus cells Seminomas arise from testicular germ cells Lymphomas arise from lymph nodes Some tumors are named eponymously e.g. Hodgkin lymphoma, Wilms’ tumor….etc Note : See table on page 164

28
Some ‘tumors’ are NOT true neoplasms
Hamartoma: Tumor-like develop. malformation in which there is abnormal mixing of normal components of the organ, either in the form of change in quantity or arrangement of tissue elements. e.g. Lung Hamartoma.

29
Choristoma: Congenital anomaly where different
types of tissue grow ectopic to the region. e.g. - Meckle’s Diverticulum in small intestine containing gastric tissue - Pancreatic heterotopia Both hamartoma & choristoma do not become malignant.

30
How do benign & malignant tumors differ?
Differentiation & anaplasia Rate of growth Presence of capsule Local invasion Distant metastasis

31
Benign versus malignant tumors

32
1- Differentiation: This indicates the degree of resemblance of the tumor cell to its cell of origin, functionally & morphologically. Example – Cells of a lipoma may look exactly like normal fat cells.

33
LIPOMA LIPOSARCOMA

34
Features of differentiation include:
Epithelial cells: - formation of glands - formation of keratin - formation of secretion…etc Connective tissue cells: - formation of osteoid - presence of lipoblasts - Striations in tumors of skeletal muscle….etc

35
1 NORMAL 2 3

36
When a tumor cell loses differentiation, it gradually gains features of DYSPLASIA
Dysplasia is a disorderly, non-neoplastic proliferation of cells with loss of architectural orientation Cells are either tumor stem cells or there is a process of gradual loss of differentiation of mature cells It may precede malignancy

37
Total loss of differentiation is
Severe Dysplasia= ANAPLASIA

38
Severe Dysplasia/ Anaplasia

39
Cytological Features of Dysplasia
Increased nuclear size , N/C ratio Variation in nuclear & cell size & shape: PLEOMORPHISM Loss of differentiating features Increased nuclear DNA content: HYPERCHROMATISM

40
Features of dysplasia (continued):-
Nucleoli: Prominent, may be multiple Mitotic figures: Increased Abnormal mitoses: may be present Loss of Polarity: Failure of orientation and polar arrangement of an epithelial surface

42
Intraepithelial Neoplasia
Dysplasia involving an epithelial surface: Low grade & High grade High grade (severe) dysplasia, still limited by the epithelial basement membrane CARCINOMA IN SITU
 dysplasia, still limited by the epithelial. basement membrane CARCINOMA IN SITU.")
43
Intraepithelial Neoplasia

44
Carcinoma in Situ B.M.

45
Invasive squamous cell carcinoma

46
NOTES:- Features of dysplasia can occur in both carcinomas & sarcomas, BUT there is No in-situ Sarcoma. Not all dysplasias progress to higher grade or carcinoma in situ. Not all carcinomas in situ progress to invasive CA.

47
2- Rate of growth Usually slow in benign & rapid in malignant tumors
Rate of growth usually correlates with level of differentiation Exceptions: Hormonal influences: e.g. Leiomyoma of uterus in pregnancy Pressure constraints Some malignant tumors may outgrow their blood supply -> C. ischemic n.

48
Some tumor growths are HORMONE-dependent:
This is through presence of receptors on surface - Breast CA - Endometrial CA - Prostatic CA IMPORTANT FACT !! WHY ??

49
3- Local invasion & Encapsulation
Benign tumors frequently have a capsule or are well-demarcated Malignant tumors progressively invade & destroy surrounding tissue e.g. *Breast cancer infiltrating skin *Basal cell carcinoma face infiltrating nerve *Second most important feature distinguishing malignant tumors

50
4- Metastasis: Spread of malignant tumors to distant sites away from the main tumor Proportionate to the size and differentiation of the primary tumor Most important factor in diagnosis of malignancy All tumors can potentially metastasize except BASAL CELL CARCINOMA & most 1ry brain tumors

51
Routes of metastases: Lymphatics Blood vessels
Seeding within body cavities/ Transcoelomic Spread

52
1- Lymphatic Spread: All cancers, but more characteristic in Carcinoma Spread follows the anatomical route of drainage e.g. Breast cancer in left upper outer quadrant Left axillary L.N. Lung Ca: Peribronchial L.N.s tracheobronchial L.N.s hilar L.N.s

53
IMPORTANT IN SURGICAL RESECTION: Sentinel Lymph Node:
First lymph node in pathway of a primary tumor. Usually outlined by a dye. Not all enlarged L.N.s indicate Mets. e.g. Reactive hyperplasia Histiocytic infiltrate in sinuses

54
2- Hematogenous spread:
Usually venous first following anatomical drainage: Lung & Liver More characteristic of Sarcoma, but may occur in carcinoma Certain carcinomas invade veins early: RENAL Carcinoma renal vein IVC Hepatocellular Carcinoma Portal & Hepatic v.

55
3- Transcoelomic spread:
Within peritoneal or pleural cavity e.g.: CA of ovary tends to spread widely through peritoneal surface CA of upper lobe of lung to lower lobe CA of stomach to ovary CA of colon across peritoneum to S.I. & distant parts of colon

56
Summary : Differences between benign & malignant neoplasms
BENIGN vs MALIGNANT Well-differentiated Low mitotic index Slow Growth With capsule No invasion No metastases Various or Anaplastic High mitotic index Rapid growth No capsule Invasion Metastases

57
Grading & Staging of Tumors

58
Grade of tumor: Based on level of differentiation:
This indicates the degree of resemblance of tumor cells to cell of origin and is always based on microscopic criteria. Grade I: Well differentiated tumor Grade II: Moderately differentiated tumor Grade III: Poorly differentiated tumor Grade IV: Anaplastic tumor

59
GRADING for Squamous Cell Carcinoma
NORMAL GRADING for Squamous Cell Carcinoma 59

60
STAGE of Tumor: This indicates the extent of spread of tumor.
Clinical, investigative procedures and pathological appearance of tumor have to be used to assess it. It depends on: * Size of tumor * Regional lymph node involvement * Metastases to distant organs

61
TNM Staging System: T : Size and extent of primary tumor (1-4) N : Presence and extent of lymph node involvement (0-3) M : Presence or absence of distant metastasis (0-1) e.g. T1,N1, M0 Staging is more important than grading because it affects treatment
 M : Presence or absence of distant. metastasis (0-1) e.g. T1,N1, M Staging is more important than. grading because it affects treatment.")
62
Must be documented for all malignant
tumors: To quantify the aggressiveness of tumor To outline mode of therapy To compare different modes of therapy To give an approximate prognosis

63
Prognosis: This indicates the final outcome of the disease in terms of 5 year or 10 year survival. This is influenced by: Tumor Type e.g. Lung CA versus Lip CA Tumor Grade & Stage Host reactions

64
EPIDEMIOLOGY of CANCER
The branch of medicine dealing with the incidence and prevalence of disease in large populations and with detection of the source and cause of epidemics of disease.

65
CANCER: Worldwide Problem Increasing
USA: 1.5 million new cancers & 596,000 cancer deaths in 2011. Increasing Due to genetic mutations in cells, which may be spontaneous or environmentally induced.

67
CANCERS in USA Females Prostate Lung & bronchus Colon & Rectum
Cancer Deaths Lung & Bronchus Colon & rectum Breast Lung & Bronchus Colon & Rectum Cancer Deaths Colon & rectum

70
CANCERS common in JORDAN 2008:
Colorectal Lung Urinary Bladder Prostate Leukemia Breast Colo-rectal Corpus Uteri Thyroid Non-Hodgkin Lymphoma M A L E S F E M A L S

71
WHAT FACTORS may influence the incidence of cancer?

72
Incidence may be related to
Genetic polymorphism: Individual predisposition to disease Individual response to environmental agents Individual response to drugs e.g. P450 Ethnic Factors

73
& other factors (Multifactorial)
1&2- Geographic & environment & other factors (Multifactorial) Prostatic CA ---- High in USA Colorectal CA ----High in USA Breast CA ---- High in USA Gastric CA -- High in Japan Skin CA High in New Zealand Hepatocellular CA --- High in Africa & China Nasopharyngeal CA --- Far East Burkitt Lymphoma --- Africa 73
 Prostatic CA ---- High in USA. Colorectal CA ----High in USA. Breast CA ---- High in USA. Gastric CA -- High in Japan. Skin CA High in New Zealand. Hepatocellular CA --- High in Africa. & China. Nasopharyngeal CA --- Far East. Burkitt Lymphoma --- Africa. 73.")
74
Environment: Diet Occupation Sunlight Personal habits Overweight

76
In general, cancer incidence ≈ AGE However, certain cancers occur
more in children Acute Leukemia Some Lymphomas Some CNS Tumors Bone & soft tissue Sarcomas Blastomas

77
A- Inherited AD Cancer Syndromes:
4- Heredity: % of tumors A- Inherited AD Cancer Syndromes: Presence of defined genetic abnormality, usually AD, often specific phenotype e.g. APC gene : Familial Adenomatous Polyposis Coli MEN1 & RET genes : MEN syndromes NF1 & NF2 genes : Neurofibromatosis ± skin pigmentation RB gene : Retinoblastoma TP53 : Li Fraumeni Syndrome

79
NEUROFIBROMATOSIS TYPE I

80
B - AR syndromes of DNA Repair:
Chromosomal & DNA instability Best example: XERODERMA PIGMENTOSUM

81
C- Familial cancers with no specific phenotype & multifactorial
Family members have higher incidence to common cancers - CA of COLON - CA of BREAST - CA of OVARY Younger age groups, multiple or bilateral, two or more family members are affected. Some linked to inheritance of mutant genes e.g. BRCA-1 & BRCA-2 (AD)
")
82
5- Acquired Preneoplastic Syndromes
These are associated with increased risk for CA and most are related to rapid or abnormal cell proliferation. 1- Endometrial Hyperplasia & carcinoma 2- Cervical Leukoplakia (Dysplasia) & Cervical Squamous cell CA. Also oral leukoplakia. 3- Bronchial epithelial dysplasia & lung & Squamous cell CA 82
 & Cervical Squamous cell CA. Also oral leukoplakia. 3- Bronchial epithelial dysplasia & lung & Squamous cell CA. 82.")
83
Acquired preneoplastic syndromes (continued)
4- Liver Cirrhosis & Hepatocellular CA 5- Ulcerative Colitis & Colorectal CA 6- Villous Adenoma & Colorectal CA 7- Others

84
MOLECULAR BASIS OF CANCER
CARCINOGENESIS: MOLECULAR BASIS OF CANCER

85
Neoplasms arising from a single clone of cells:
MONOCLONAL proliferation

86
What is a CLONE ? A. a cell, cell product, or organism that is genetically identical to the unit or individual from which it was derived. B. a population of identical units, cells, or individuals that derive from the same ancestral line.

87
Principles: Tumors arise from clonal growth of
transformed cells that have developed mutations in several classes of genes: Growth promoting proto-oncogenes Growth inhibiting tumor suppressor genes Regular suppressor (RB) & Guardians (TP53) Genes regulating apoptosis Genes involved in DNA repair More than one mutation in above result in abnormal growth of cells
 & Guardians (TP53) Genes regulating apoptosis. Genes involved in DNA repair. More than one mutation in above result in abnormal growth of cells.")
88
Genes in Neoplastic Transformation:

89
Gene Lesions in Tumors

90
- Non detectable - Detectable

91
Different Gene Lesions:
1- Point mutation: Change in a single base in a nucleotide sequence may activate an oncogene, or inactivate a tumor suppressor e.g. RAS oncogene (codon 12, 13) in Pancreatic carcinoma
 in Pancreatic carcinoma.")
92
2- Translocation: Balanced t. mainly in lymphoid and
hematopoietic tumors: Burkitt Lymphoma : 8;14 Follicular B cell Lymphoma : 14;18 Chronic myeloid leukemia : 9;22 ( PHILADELPHIA Chromosome) Fusion Gene is produced: BCR-ABL (tyrosine kinase activity)
 Fusion Gene is produced: BCR-ABL. (tyrosine kinase activity)")
94
Other fusions identified in some
prostate & lung CA. Balanced translocation seen in some solid tumors: Ewing Sarcoma t.(11;22)(q24;q12)
(q24;q12)")
95
Downloaded from: StudentConsult (on 16 October 2012 10:05 AM)
© 2005 Elsevier

96
3- Gene amplification: - Double minutes: Small fragments of extrachromosomal DNA - Homogenous staining regions produced by chromosomal segments with various lengths and uniform staining intensity Examples: - Neuroblastoma : N-MYC - Breast carcinoma : HER2/Neu

97
Gene Amplification :

98
in nonhematopoietic & solid tumors e.g. Retinoblastoma 13q band14
4- Chromosomal deletions: More in nonhematopoietic & solid tumors e.g. Retinoblastoma 13q band14 also several in colorectal CA 5- Chromosomes loss or gain: Change from the normal multiples of 23 (Aneuploidy) Result: Change in structure or quantity of gene product
 Result: Change in structure or quantity of gene product.")
99
6- Micro RNAs: Single stranded RNA of about 22 nucleotides act as regulators of genes
Overexpression of miRNAs can contribute to carcinogenesis by ↓ the expression of tumor suppressors. Deletion or loss of expression of miRNAs can lead to overexpression of proto-oncogenes.

100
7- Epigenetic changes: Heritable change that occurs without mutation, but through methylation. This may silence tumor suppressor genes & repair genes leading to carcinogenesis.

101
Carcinogenesis is a MULTISTEP PROCESS!

102
Transformed Cell

104
Tumor Progression: This is the stepwise accumulation of
mutations resulting in increasing features of malignancy.

105
Downloaded from: StudentConsult (on 16 October 2012 10:05 AM)
© 2005 Elsevier

106
GENES IN NEOPLASTIC TRANSFORMATION

107
TRANSFORMATION Self-sufficiency in growth signals
Insensitivity to growth-inhibiting signals Evasion of apoptosis & repair Angiogenesis Limitless replicative potential: Telomerase Ability to invade & metastasize The various aspects of “malignant transformation”. Just like cancer itself is a progression of increasingly disturbing processes, so is malignant transformation. These are not necessarily exactly linear events, but close.

108
Downloaded from: StudentConsult (on 16 October 2012 10:05 AM)
© 2005 Elsevier

109
1-Genes coding for growth: Classified by site of action
Proto-oncogenes are dominant genes. Mutant proto-oncogenes Oncogenes oncoproteins They include: Growth factors Cell surface receptors Signal transduction proteins Nuclear transcription factors Cell cycle proteins Inhibitors of apoptosis

110
1- Oncogenes coding Growth Factors
Cell growth is stimulated by its own GF or from other cells: Platelet derived growth factor (PDGF) seen in glioblastomas Fibroblast growth factor (FGF) - stomach CA & melanoma……etc Transforming Growth Factor (TGF-) in sarcomas Products of other oncogenes (e.g. RAS) may cause overexpression of GF
 seen in glioblastomas. Fibroblast growth factor (FGF) - stomach CA. & melanoma……etc. Transforming Growth Factor (TGF-) in sarcomas. Products of other oncogenes (e.g. RAS) may cause overexpression of GF.")
111
2- Oncogenes coding Growth Factor Receptors
GF integrate with membrane receptors tyrosine kinase activity nucleus Mutant receptor continuous signals even in the absence of GF…..OR Normal but overexpressed hypersensitive to GF Epidermal GF receptor family: ERBB1 in 80% of sq. CA lung & 50% of GBM ERBB2 ( HER 2 NEU) in 25-30% of breast & ovarian CA --- Increase = POOR PROGNOSIS
 in 25-30% of breast. & ovarian CA --- Increase = POOR PROGNOSIS.")
112
RAS & non receptor ABL RAS action:

113
GTPase activity by (GAP)
RAS action: GDP GTP proliferation Active RAS Signal transduction (RAF/MAP-K or PI3-K/AKT pathways) transcription activation Commonest oncogene mutation Point mutations in codon 12, 13 are present in 30% of cancers, especially CA pancreas & Colon Mutations in GAPs (NF1): Neurofibromatosis Active RAS GTPase activity by (GAP)
 transcription activation. Commonest oncogene mutation. Point mutations in codon 12, 13 are present. in 30% of cancers, especially CA pancreas & Colon. Mutations in GAPs (NF1): Neurofibromatosis. Active RAS. GTPase activity by (GAP)")
114
Normal ABL is located in nucleus where it promotes apoptosis
Action of ABL: Non receptor associated tyrosine kinase signal transmission Normal ABL is located in nucleus where it promotes apoptosis Chronic myeloid leukemia: 9;22 translocation BCR-ABL hybrid gene This new gene protein is retained in cytoplasm where it has tyrosine kinase activity cell proliferation New action is Proliferation + No Apoptosis

115
4- Nuclear Transcription Factors:
DNA transcription regulated by genes e.g. MYC*, JUN, FOS….etc. In normal: MYC protein + DNA Activation of Cyclin Dependant Kinases (CDKs) initiation of cell cycle MYC MYC mutation sustained activation Examples: Dysregulation of MYC present in Burkitt lymphoma due to translocation t (8;14) Breast, colon, lung CA & neuroblastoma
 initiation of cell cycle MYC. MYC mutation sustained activation. Examples: Dysregulation of MYC present in Burkitt lymphoma due to translocation t (8;14) Breast, colon, lung CA & neuroblastoma.")
116
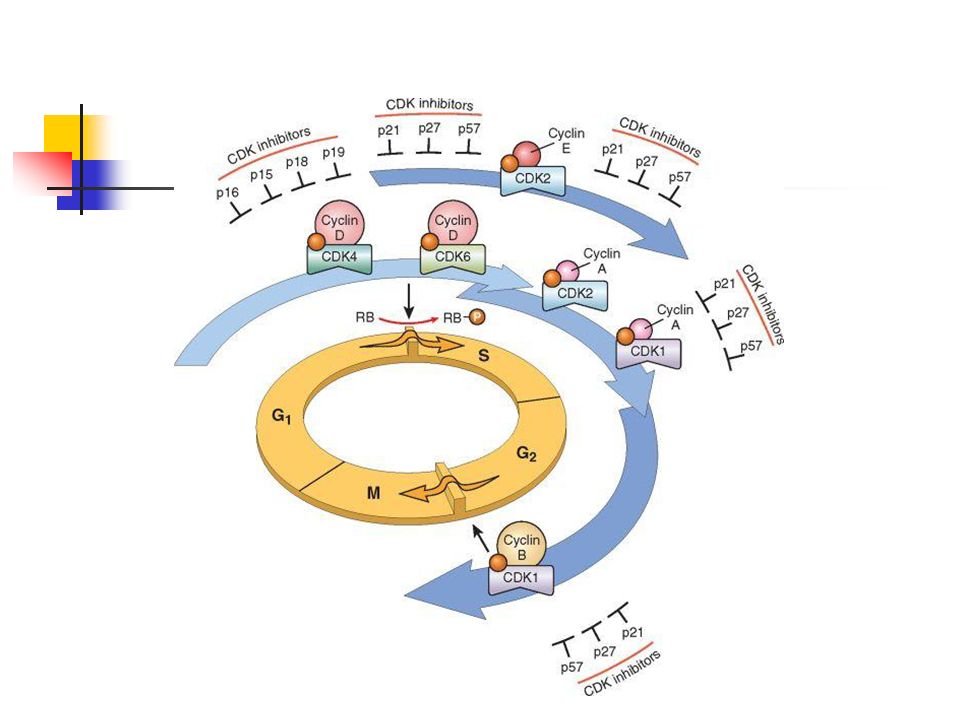
5- Cyclins & Cyclin Dependant – Kinases regulate Cell Cycle phases
Family of proteins that control entry of the cells at specific stages of cell cycle ( D, E, A, B….etc.) Level of a specific cyclin increases at a specific stage, then decreases rapidly after the cell departs that stage Function by phosphorylating certain proteins ( e.g. RB protein) Cyclins bind to CDKs, activating them
 Level of a specific cyclin increases at a specific stage, then decreases rapidly after the cell departs that stage. Function by phosphorylating certain proteins ( e.g. RB protein) Cyclins bind to CDKs, activating them.")
117
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 November 2007 08:09 AM)
© 2007 Elsevier

118
Two important groups: - Cyclin D family CDK4 & CDK6 at G1 S phase checkpoint - Cyclin B-CDK1 activate G2 M transition

119
Activity of CDK/ Cyclin regulated by
CDK inhibitors Selective or nonselective inhibition Examples: p21, p27 & p57 inhibit all CDKs while INK4 Inhibitors (p15, p16, p18 & p19) inhibit CDK4 & CDK6 Expression of p21 is controlled by the tumor suppressor protein p53 G1 phase arrest in response to a variety of stress stimuli.
 inhibit CDK4 & CDK6. Expression of p21 is controlled by the tumor suppressor protein p53 G1 phase arrest in response to a variety of stress stimuli.")
121
Disabling mutations of p16 (CDKN2A)
Mutations that dysregulate activity of cyclins & CDKs → cell proliferation Examples: Cyclin D is overexpressed in breast, liver & esophageal cancers Amplification of CDK4 gene is present in melanoma, sarcomas, glioblastoma Disabling mutations of p16 (CDKN2A)
")
122
2- Cancer Suppressor Genes:-
Growth inhibitory pathway by: * Regulate cell cycle: Rb gene * Regulate cycle & apoptosis: TP 53 * Block GF signals: TGF- * APC regulates -catenin Cancer suppressor genes are recessive genes which may be lost in familial or sporadic cases. TGF- stimulated production of CDK inhibitors & inhibits CDK2 &CDK4.Present in most pancreatic & GIT cancers. APC present in multiple adenomatosis coli 100% risk Present in sporadic cases 70-80% OR, if absent ,mutation in -catenin

123
In cases with familial predisposition for development of tumors, affected persons inherit one defective (nonfunctional) copy of a tumor suppressor gene and lose the second one through somatic mutation. In sporadic cases, both copies are lost through somatic mutations.

124
1- RB gene: First studied in Retinoblastoma: Called RB gene
Both copies of gene must be lost for neoplastic transformation to occur This is called loss of heterozygosity Familial ( RB RB ) or Sporadic ( RB RB RB ) TGF- stimulated production of CDK inhibitors & inhibits CDK2 &CDK4.Present in most pancreatic & GIT cancers. APC present in multiple adenomatosis coli 100% risk Present in sporadic cases 70-80% OR, if absent ,mutation in -catenin
 or. Sporadic ( RB RB RB ) TGF- stimulated production of CDK inhibitors & inhibits CDK2 &CDK4.Present in most pancreatic & GIT cancers. APC present in multiple adenomatosis coli 100% risk. Present in sporadic cases 70-80% OR, if absent ,mutation in -catenin.")
125
Retinoblastoma: Autosomal dominant hereditary disease (40%)
May be sporadic (60%) In familial form, patients carry one mutation in their genome, followed by second mutation in retinal cells No tumor develops unless two alleles in 13q14 become mutant (two hit theory) ↑incidence of bilateral Retinoblastoma and ↑ osteosarcoma in hereditary forms
 In familial form, patients carry one mutation in their genome, followed by second mutation in retinal cells. No tumor develops unless two alleles. in 13q14 become mutant (two hit theory) ↑incidence of bilateral Retinoblastoma and ↑ osteosarcoma in hereditary forms.")
126
Inheritance of Retinoblastoma

127
Mode of action of RB gene:

128
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 November 2007 08:09 AM)
© 2007 Elsevier

129
In G1 S, requires the activity of
cyclin E/CDK2 Cyclin E is dependent on the E2F family of transcription factors. Active hypophosphorylated Rb binds to & inhibits the E2F family of transcription factors NO TRANSCRIPTION of cyclin E. Growth factor signaling leads to cyclin D expression and activation of cyclin D-CDK4/6 complexes which phosphorylate Rb, inactivating the protein and releasing E2F TRANSCRIPTION (G1 S phase )
")
130
Many oncogenic DNA viruses, like HPV, encode proteins (e. g
Many oncogenic DNA viruses, like HPV, encode proteins (e.g., E7) that bind to Rb and render it nonfunctional
 that bind to Rb and render it nonfunctional.")
131
2- TP 53 TP 53 is a negative regulator of cell cycle
(protein product is p53) 70% of tumors show homozygous loss of TP 53 (commonest suppressor) ‘Guardian of the Genome’ OR (Policeman) preventing genetically damaged cells from progressing through new cycle.
 70% of tumors show homozygous loss of. TP 53 (commonest suppressor) ‘Guardian of the Genome’ OR (Policeman) preventing genetically damaged cells from progressing through new cycle.")
132
p53 is inactivated by its negative regulator MDM2.
Upon DNA damage or other stresses, various pathways will lead to the dissociation of the p53 and MDM2 complex.

133
Mode of activation & action:
P53 senses DNA damage through various sensors, like protein kinases e.g. Ataxia telangiectasia mutated (ATM) protein ** P53 is activated by anoxia & others Activated p53 → Transcription of CDKI (p21) → cell cycle arrest at G1 Result in more time for repair Normal
 protein ** P53 is activated by anoxia & others. Activated p53 → Transcription of CDKI (p21) → cell cycle arrest at G1. Result in more time for repair Normal.")
134
OR: Failed repair Apoptosis or Senescence
(permanent cell cycle arrest) OR Fixed mutation NEOPLASIA More functions of TP53: Transcription of certain repair genes, micro RNAs (inhibit cyclins and BCL2)...etc p53 is a regulator of apoptosis P 21 is CDK inhibitor & GADD45 is Growth Arrest & DNA Repair LF s. have 25% increase risk of CA by age 50. Overall, 70% of CA’s have defective PT53. Rest have defectin genes controlling its level.
 OR Fixed mutation NEOPLASIA. More functions of TP53: Transcription of certain repair genes, micro RNAs (inhibit cyclins and BCL2)...etc. p53 is a regulator of apoptosis. P 21 is CDK inhibitor & GADD45 is Growth Arrest & DNA Repair. LF s. have 25% increase risk of CA by age 50. Overall, 70% of CA’s have defective PT53. Rest have defectin genes controlling its level.")
135
Significance of TP53 mutation:
Acquired mutation in many cancers e.g. colon, breast, lung , leukemia…etc Inherited mutation in one allele Li - Fraumeni S. 25 fold malignancy: sarcoma, leukemia, breast carcinoma and gliomas ….. etc May be blocked by some DNA viruses (oncogenic HPV, HBV & EBV) producing viral-induced cancers
 producing viral-induced cancers.")
Similar presentations














>")





 have two basic components. Proliferating neoplastic cells that constitute.>")

 –Lung tissue –Breast tissue (glands/ducts) –Prostate (gland) –White blood cells.>")




