Download presentation
Presentation is loading. Please wait.

1
Congestive Heart Failure MUHAMMAD ALI PEDIATRIC CARDIOLOGY DIVISION

2
Definition Congestive heart failure (CHF) is a clinical syndrome in which the heart is unable to pump enough blood to the body to meet its needs, to dispose of venous return adequately, or a combination of the two. Cause CHF may result from congenital or acquired heart diseases with volume and/or pressure overload or from myocardial insufficiency.

3
CONGENITAL HEART DISEASE CHD with volume or pressure overload is the most common cause of CHF in the pediatric age group. Volume overload lesions, such as VSD, PDA and ECD, are the most common causes of CHF in the first 6 months of life. Children with TOF) do not develop CHF unless they have received a large aorta—to—pulmonary artery (PA) shunt procedure (such as the Waterston or Potts operation), which is no longer performed.
 do not develop CHF unless they have received a large aorta—to—pulmonary artery (PA) shunt procedure (such as the Waterston or Potts operation), which is no longer performed..")
4
ASD rarely causes CHF in the pediatric age group, although it causes CHF in adulthood. Large L-R shunt lesions, such as VSD and PDA, do not cause CHF before 6 to 8 weeks of age because the PVR does not fall low enough to cause a large left-to- right shunt until this age. The onset of CHF resulting from L-R shunt lesions may be earlier in premature infants (within the first month) because of an earlier fall in the PVR in these infants.
 because of an earlier fall in the PVR in these infants..")
7
ACQUIRED HEART DISEASE Metabolic abnormalities (severe hypoxia and acidosis, hypoglycemia and hypocalcemia) Endocardial fibroelastosis Viral myocarditis Acute rheumatic carditis Rheumatic valvular heart diseases Dilated cardiomyopathy Cardiomyopathies associated with muscular dystrophy and Friedreich's ataxia Doxorubicin cardiomyopathy
 Endocardial fibroelastosis Viral myocarditis Acute rheumatic carditis Rheumatic valvular heart diseases Dilated cardiomyopathy Cardiomyopathies associated with muscular dystrophy and Friedreich s ataxia Doxorubicin cardiomyopathy")
8
MISCELLANEOUS CAUSES Supraventricular Tachycardia (SVT) Complete heart block Severe anemia Acute hypertension Bronchopulmonary dysplasia Acute cor pulmonale caused by acute airway obstruction
 Complete heart block Severe anemia Acute hypertension Bronchopulmonary dysplasia Acute cor pulmonale caused by acute airway obstruction")
9
Physical Examination The following are compensatory responses to impaired cardiac function: –Tachycardia, gallop rhythm, and weak and thready pulse –Cardiomegaly –There are signs of increased sympathetic discharges (e.g., growth failure; perspiration; cold, wet skin). Pulmonary venous congestion (left-sided failure) results in the following: –Tachypnea is common. –Dyspnea on exertion (poor feeding in small infants) is common. –Orthopnea –Wheezing and pulmonary crackles
 results in the following: –Tachypnea is common. –Dyspnea on exertion (poor feeding in small infants) is common. –Orthopnea –Wheezing and pulmonary crackles.")
10
. Systemic venous congestion (right-sided failure) results in the following: - Hepatomegaly - Puffy eyelids - Distended neck veins and ankle edema - Splenomegaly
 results in the following: - Hepatomegaly - Puffy eyelids - Distended neck veins and ankle edema - Splenomegaly")
11
X-ray Studies The presence of cardiomegaly should be demonstrated by chest x-ray films. The absence of cardiomegaly almost rules out the diagnosis of CHF Electrocardiography ECGs help determine the type of defect but are not helpful in deciding whether CHF is present Echocardiography Echo may confirm an enlarged chamber or impaired left ventricle (LV) function (decreased fractional shortening or ejection fraction, increased left preejection period/left ventricular ejection time).
 function (decreased fractional shortening or ejection fraction, increased left preejection period/left ventricular ejection time)..")
12
Management The treatment of CHF consists of: (1) elimination of the underlying causes (2) elimination of the precipitating or contributing causes (e.g., infection, anemia, arrhythmias, fever) (3) control of heart failure state by the use of multiple drugs, usually inotropic agents, diuretics, and afterload-reducing agents.
 elimination of the underlying causes (2) elimination of the precipitating or contributing causes (e.g., infection, anemia, arrhythmias, fever) (3) control of heart failure state by the use of multiple drugs, usually inotropic agents, diuretics, and afterload-reducing agents.")
13
GENERAL MEASURES A “cardiac chair” or “infant seat” is used to relieve respiratory distress Oxygen (40% to 50%) with humidity is administered to infants with respiratory distress Sedation with morphine sulfate (0.1 to 0.2 mg/kg per dose subcutaneously every 4 hours as needed) or phenobarbital (2 to 3 mg/kg per dose by mouth or intramuscularly every 8 hours as necessary) In older children, salt restriction (<0.5 g/day) and avoidance of salty snacks (chips, pretzels) and table salt are recommended Daily weight measurement Predisposing factors, such as fever, anemia, and infection, are eliminated Underlying causes such as hypertension, arrhythmias, and thyrotoxicosis are treated.
 with humidity is administered to infants with respiratory distress Sedation with morphine sulfate (0.1 to 0.2 mg/kg per dose subcutaneously every 4 hours as needed) or phenobarbital (2 to 3 mg/kg per dose by mouth or intramuscularly every 8 hours as necessary) In older children, salt restriction (<0.5 g/day) and avoidance of salty snacks (chips, pretzels) and table salt are recommended Daily weight measurement Predisposing factors, such as fever, anemia, and infection, are eliminated Underlying causes such as hypertension, arrhythmias, and thyrotoxicosis are treated.")
14
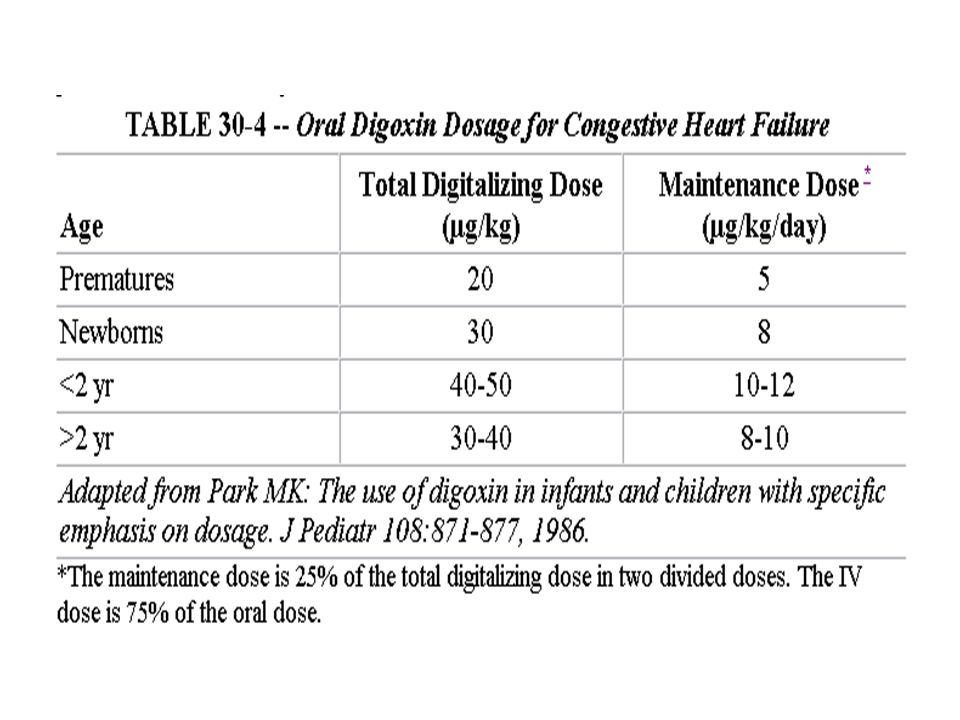
DRUG THERAPY Three major classes of drugs are used in the treatment of CHF in children: inotropic agents, diuretics, and afterload-reducing agents. Rapidly acting inotropic agents (dopamine, dobutamine) are used in critically or acutely ill infants and children. Digoxin is used in all noncritically ill patients. The use of digoxin is contraindicated in hypertrophic cardiomyopathy, complete heart block, or cardiac tamponade. Diuretics are almost always used with inotropic agents. Afterload-reducing agents have gained popularity because they can increase cardiac output without increasing myocardial oxygen consumption.
 are used in critically or acutely ill infants and children. Digoxin is used in all noncritically ill patients. The use of digoxin is contraindicated in hypertrophic cardiomyopathy, complete heart block, or cardiac tamponade. Diuretics are almost always used with inotropic agents. Afterload-reducing agents have gained popularity because they can increase cardiac output without increasing myocardial oxygen consumption..")
20
THANK YOU

Similar presentations











 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")


 ASST. PROFESSOR CLINICAL APPROACH & MANAGEMENT OF CHF.>")



. “Heart (or cardiac) failure is the pathophysiological state in which the heart is unable to pump blood at a rate commensurate.>")
, means your heart can't pump enough blood to meet your body's.>")




, F.R.C.P.( E ) F.R.C.P. ( LONDON.>")
